


Abstract
Objectives: To identified vitamin K2 deficiency rate and risk factors among newborns in China and assess the importance of high-risk maternal intakes of vitamin K2.
Methods: This retrospective study was performed at the Neonatology Department, the Affiliated Hospital of Guangdong Medical University, China. Routinely collected mother-neonate hospitalization data from July 2020 to January 2021 were analyzed. In total, data from 200 neonates who had completed vitamin K2 tests were utilized to assess the prevalence of vitamin K2 deficiency and identify the potential risk factors. According to the vitamin K2 level, the neonates were divided into 2 groups: cases (vitamin K2 deficiency) and controls (no vitamin K2 deficiency). The potential risk factors for vitamin K2 deficiency were evaluated by univariate and multivariate logistic regression.
Results: The vitamin K2 level in 24 of the 200 neonates was undetectable (<0.05 ng/mL). The prevalence of low serum vitamin K2 (<0.1 ng/ml) was 33%. Study subjects with antenatal corticosteroids use had an approximately 5-fold greater risk of developing vitamin K2 deficiency. In the univariate analyses, small-for-gestational-age (SGA), caesarean section, maternal gestational diabetes and premature rupture of the membranes were risk factors for vitamin K2 deficiency. In the multivariate logistic regression analysis, high antenatal corticosteroids use, cesarean section, and SGA were independently associated with vitamin K2 deficiency.
Conclusion: The present study demonstrated that antenatal corticosteroids use is independently associated with vitamin K2 deficiency. This finding highlights the importance of routine vitamin K2 supplementation in late-stage pregnant women and neonates in China.
Vitamin K2 mostly originates from bacterial synthesis and is found in fermented foods, such as the Japanese food “natto”.1,2 Vitamin K2 is mainly distributed in circulatory system and exerts biological effects in the bones and vasculature.3 Vitamin K2 was initially thought to play a primary role in coagulation, bone health, bacterial energy production, brain development, inhibition of vascular stiffness and optimal body weight.2,4 In a Dutch study, increased vitamin K2 was related to a reduced risk of cardiovascular disorders, suggesting a protective effect of vitamin K2 in cardiovascular system.5,6 Although cardiovascular events are rare in children, study had found that the beginnings of arterial calcification have been observed in children.2 Therefore, an optimal vitamin K2 intake is critical to support cardiovascular health. Prolonged use of corticosteroids may lead to glucocorticoid-induced osteoporosis (GIOP).7 Researchers found that vitamin K2 treatment could decrease the osteoporotic bone loss and prevent bone fracture in GIOP.8 Chen et al7 found that vitamin K2 supplementation has been shown to augment osteoblast autophagy/mitophagy may significantly improve clinical outcomes of GIOP patients.
Because of changes in food habits over the last 5 decades, vitamin K2 intake has significantly decreased, leading to serious health implications.2 Optimizing outcome for preterm infants with RDS includes appropriate and timely use of antenatal corticosteroids (administration of corticosteroids during pregnancy).9 A systematic review found that prophylactic corticosteroids before elective caesarean section at term probably reduces admission to the neonatal intensive care unit for respiratory morbidity.10 The use of antenatal corticosteroids could accelerate fetal lung maturation in women at risk of preterm birth.11 Although antenatal corticosteroids are very frequent in preterm infants, the effect of antenatal corticosteroids on vitamin K2 status is unknown. Few case–control studies have examined the prevalence of vitamin K2 deficiency and its risk factors among neonates in China. To fill this gap, this study examined vitamin K2 concentrations in approximately 200 neonates. Our objective was to identify vitamin K2 deficiency rate in neonates in western guangdong region of China, especially among preterm infants, and to further explore the risk factors of vitamin K2 deficiency and emphasize the importance of vitamin K2 supplementation for high-risk pregnant women.
Methods
This is a retrospective single-center clinical study. The sample for this case-control study comprised neonates who had completed vitamin K2 testing from July 2020 to January 2021 at the Neonatology Department, the Affiliated Hospital of Guangdong Medical University. Based on their vitamin K2 levels, the neonates were divided into 2 groups: vitamin K2 deficiency (vitamin K2 <0.1 ng/ml) and normal group (vitamin K2: 0.1-0.86 ng/ml). At present, we refer to the standard of MDI laboratory in Germany. In terms of potential risk factors, the definition of small-for-gestational age (SGA) was birth weight <10th percentile for the same gestational age (GA). Prematurity refers to GA of less than 37 weeks. The inclusion criteria for this study were: admission within 24 hours of birth at the study hospital; complete clinical case notes; written informed consent provided by the family of the neonate. Participants were excluded if they had one or more of the following conditions: inherited metabolic diseases or chromosomal abnormalities; liver injury; anti-vitamin K treatment; death. In total, 200 neonates were recruited for this study. The study was approved by the Ethics Committee of the Affiliated Hospital of Guangdong Medical University (approval number: PJ2021-097); All legal guardians of the newborns signed informed consent. This research was conducted according to principles of Helsinki Declaration.
Specimen collection and testing method
Within 24-72 hours of birth, 2 ml of venous blood was collected and stored in 2-8°C. Then, the blood samples were sent to Shenzhen Hehe Medical Laboratory for testing. The blood samples were purified with organic reagents such as methanol or acetonitrile. A mass spectrometer (Liquid chromatography [LC]/mass spectrometry [MS] model AB4500, USA) were used to analyze the purified blood samples. The LC mobile phase was adjusted and the chromatography parameters were altered, including the column, column temperature, and flow rate, to comprehensively determine the optimal detection parameters according to the separation characteristics of vitamins K1 and K2 and the peak shape of the target. This allowed for the effective separation of vitamin K1 and vitamin K2. At the same time, a compound with similar chemical properties to the target compound was selected as the internal standard substance. Liquid chromatography-mass spectrometry was then used to analyze the blood samples to quantify the ion pair peak areas of the internal standard substance and vitamin, after adjusting the parameters. Vitamin K values <0.1 ng/ml (detectable values) were taken to indicate vitamin K2 deficiency.
Baseline information and potential confounders
The baseline clinical data of the neonates were obtained from the medical records, and included: i) maternal characteristics: maternal age, gravidity, preeclampsia/eclampsia, premature rupture of membranes (PROM), antenatal corticosteroids, gestational diabetes, twins or multiples, intrauterine distress, antibiotic use, anemia, and placental abnormalities (placenta previa, placental abruption). Dexamethasone (6mg Q12h×4) is used as the antenatal corticosteroids in our center. ii) Neonatal factors: type of delivery, gender, GA, birth weight, SGA, Apgar score, hemoglobin value, coagulation function (PT, APTT and FIB), serum total calcium, blood phosphorus, and blood glucose level.
Statistical analysis
The data were analyzed using SPSS Statistics for Windows, version 26 (IBM Corp., Armonk, N.Y., USA). Continuous baseline variables are showed as the mean ± standard deviation (SD) or the median with the 25th and 75th percentiles [median (IQR)]. Differences in the baseline variables (namely, vitamin K2 deficiency and vitamin K2 normal groups) were evaluated using t-tests or Mann–Whitney tests for continuous variables and Chi-square tests for categorical variables. To investigate the risk factors for vitamin K2 deficiency, univariate analyses were first performed, and variables with p<0.1 were screened out for further analysis. These significant univariate predictors were then taken into a multivariable logistic regression to recognize the independent risk factors for vitamin K2 deficiency. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. A 2-sided p value of <0.05 was considered to be statistically significant.
Results
Baseline characteristics
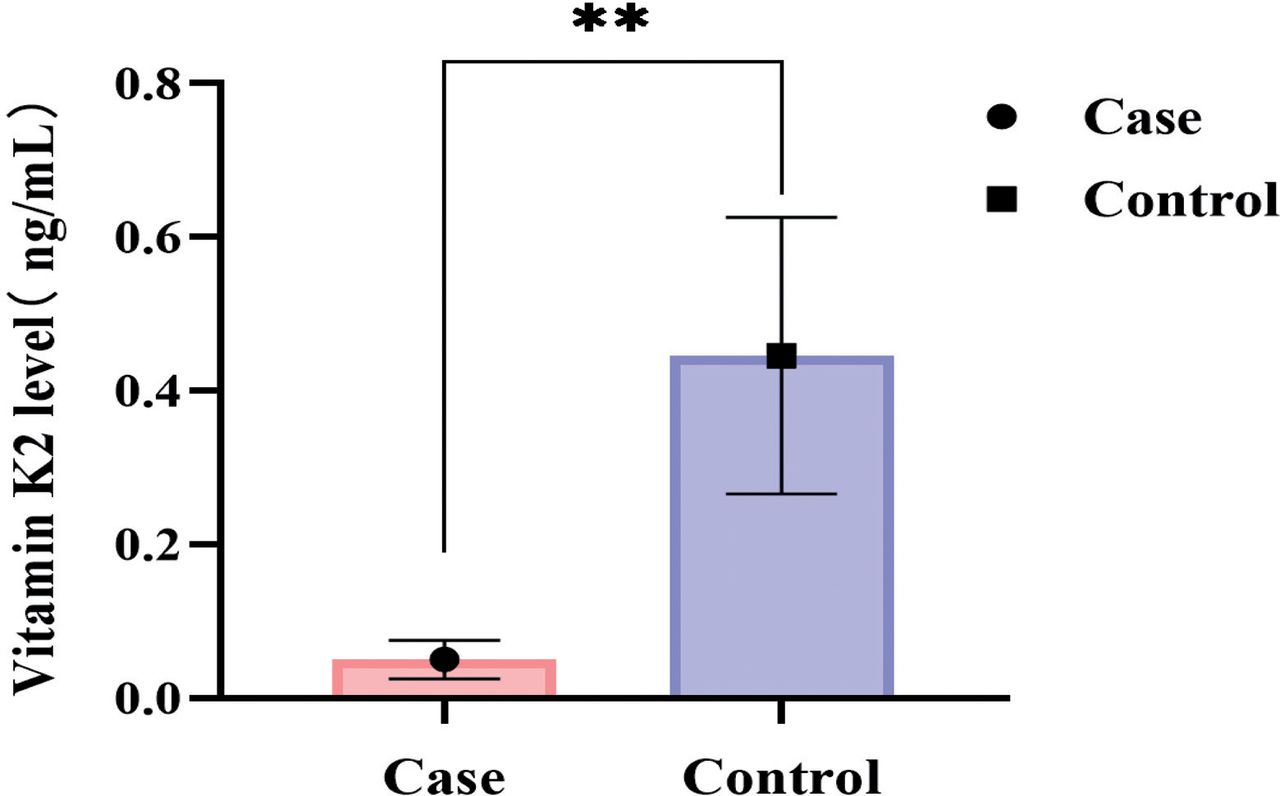
This retrospective study recruited 200 newborns (121 males and 79 females). Among them, 66 were enrolled in the vitamin K2 deficiency and 134 in the normal vitamin K2 group. Eight (4%) neonates had a GA <28 weeks, 17 (8.5%) were SGA, and 137 (68.5%) were premature. The basic clinical features, perinatal characteristics, measured parameters, and neonatal risk factors are presented in Table 1. The vitamin K2 level in 24 of the 200 neonates was undetectable (<0.05 ng/mL), suggesting low tissue stores. Overall, 66 (33%) neonates were classified as vitamin K2 deficiency. The difference in the vitamin K2 levels was statistically significant, as shown in Figure 1. There were significant differences in the incidence of gestational diabetes (p=0.008), use of antenatal corticosteroids (p=0.000), and premature rupture of of members)PROM in mothers (p=0.011) between the vitamin K2 deficiency group and the normal vitamin K2 group (Table 1). The vitamin K2 deficiency group also had a higher prevalence of cesarean section (75.7% vs 50.7%, p=0.001) and SGA (18.1% vs 4.47%, p=0.001). There were no statistically significant differences between the vitamin K2 deficiency group and the normal group in terms of maternal factors such as maternal age, gravidity, and preeclampsia/eclampsia, and neonatal factors such serum total calcium, blood phosphorus, coagulation indicators, and blood glucose (p>0.05).

- Comparison of vitamin K2 level in case and control group.
- Baseline characteristics of mothers and neonates between 2 groups.
Univariate analysis of vitamin K2 deficiency
The univariate logistic regression results are presented in Table 2. Infants with a history of antenatal corticosteroids use had an approximately 5-fold (OR=5.675, 95%CI=2.659-12.112, p=0.000) increased risk of developing vitamin K2 deficiency. Moreover, caesarean section (OR=3.151, 95%CI=1.586-6.263, p=0.001), SGA (OR=4.898, 95%CI=1.74-13.78, p=0.003), maternal gestational diabetes (OR=2.752, 95%CI=1.275-5.944, p=0.01), and PROM (OR=2.581, 95%CI=1.278-5.426, p=0.012) were associated with higher odds of vitamin K2 deficiency in neonates.
- Univariate analysis of vitamin K2 deficiency.
Multivariate analysis of vitamin K2 deficiency
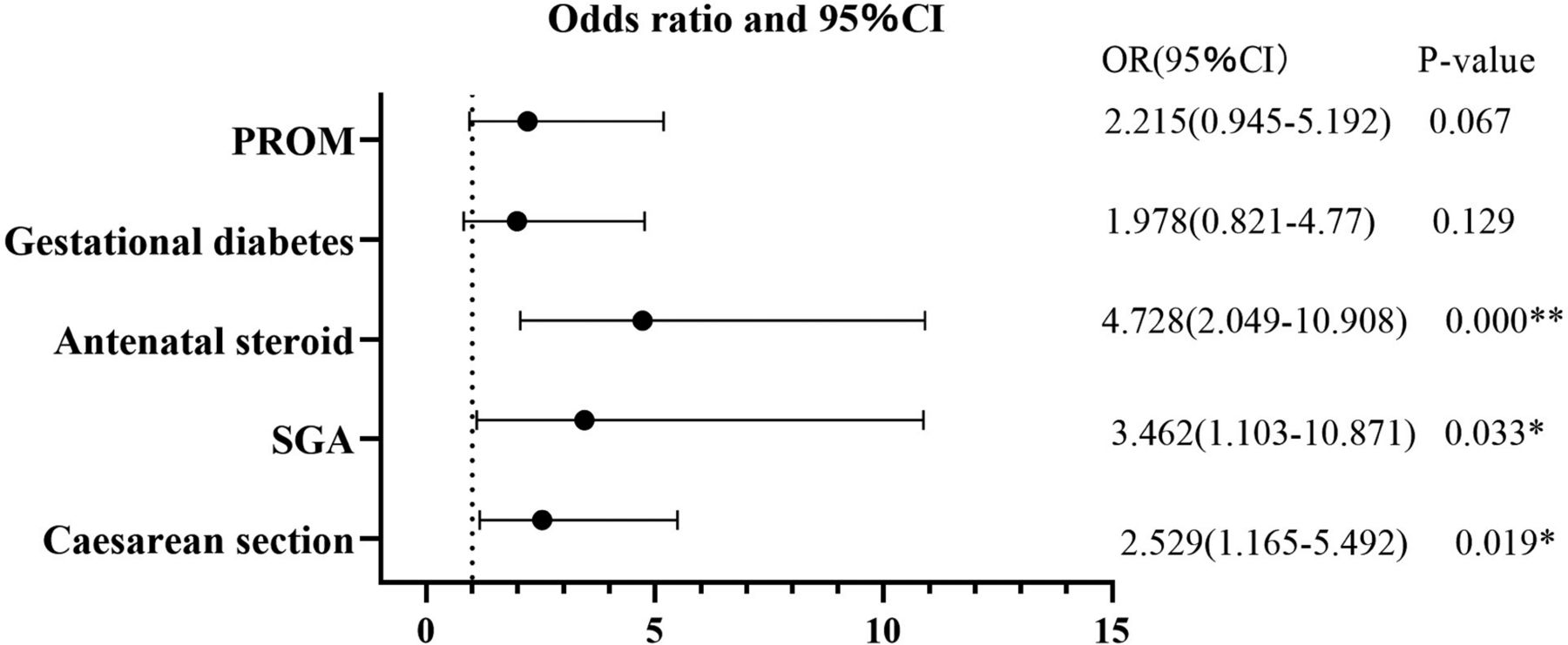
The multivariate regression analysis included the significant variables identified in the above univariate analyses. A forest plot containing all significant univariate predictors is shown in Figure 2. After adjusting for the influence of confounding factors in the multivariate analysis, antenatal corticosteroids use (odds ratio [OR]=4.728, 95% confidence interval [CI]=2.049-10.908, p=0.000), cesarean section (OR=2.529, 95% CI=1.165-5.492, p=0.019), and SGA (OR=3.462, 95%CI=1.103-10.871, p=0.033) were associated with increased risks of vitamin K2 deficiency.

- Adjusted odds ratios for calculating risk factors for vitamin K2 deficiency using multivariate logistic regression analysis. *P<0.05, **P<0.01.
Discussion
Vitamin K2 has attracted much research attention in recent years. However, few previous studies surveyed the prevalence of vitamin K2 deficiency of neonates and the associated risk factors in China. The results found a relatively high prevalence of vitamin K2 deficiency in neonates (33%), with antenatal corticosteroids use independently predicting vitamin K2 deficiency.
The etiology of vitamin K2 deficiency is multifactorial with various risk factors implicated. Previous reports indicated that neonates are prone to vitamin K2 deficiency because of limited stores at birth (endogenous insufficiencies) and insufficient intake (exogenous insufficiencies). Endogenous insufficiency is associated with insufficient intestinal colonisation by bacteria, while exogenous insufficiency may be due to limited vitamin K transport and resulting low stores, and the relatively low vitamin K2 concentration in breast milk.2,12 Thus, breastfeeding mothers should be encouraged to consider vitamin K2 supplementation.2 In the current study, vitamin K2 deficiency rate was 33% in all neonates and 32% in preterm infants. However, recent findings have suggested that preterm infants are of particular concern since vitamin K2 deficiency can develop more rapidly in preterm infants.13 Microfloral gut colonization of the gastrointestinal tract may be delayed because of a delay in feeding and repeated exposure to antibiotics of preterm infants.14 Together, these findings contribute to our understanding of the importance of vitamin K2 deficiency.
To date, few studies have investigated the potential risk factors for vitamin K2 deficiency. Exclusive breast-feeding is a common risk factor for vitamin K2 deficiency.15 Maternal drugs (such as warfarin, anticonvulsants), malabsorption diseases (such as cystic fifibrosis, biliary atresia, or other liver diseases with cholestasis) or chronic diarrhoea and antibiotic therapy are both risk factors for vitamin K deficiency.15,16 Ampaiwan Chuansumrit‘s study on vitamin K2 deficiency in Thai newborns found that premature, SGA and caesarean section were risk factor for significant vitamin K deficiency.17 In the current univariate analyses, antenatal steroid use, cesarean section, SGA, gestational diabetes, and PROM were associated with increased risks of vitamin K2 deficiency. However, in the multivariate logistic regression analysis, antenatal steroid use, cesarean section, and SGA were significant independent risk factors. There were no significant differences in neonatal and maternal factors, such as GA, birth weight, maternal age, gravidity, and preeclampsia/eclampsia, between the 2 groups.
Vitamin K2 is produced mainly by bacterial synthesis.18,19 Lactic acid bacteria, as a main source of vitamin K2 in the Western diet, which are used in food manufacturing to ferment and preserve dairy products, are a common route for vitamin K2 synthesis.1,20 Previous research has revealed changes in the gut microbiota due to antibacterial drugs which, in turn, affect intestinal vitamin K2 production.2 Because the circulation of vitamin K was disrupted, the level of vitamin K2 in the liver dropped in people taking antibiotics. Chatterjee et al19 found that vitamin K2 co-treatment with antibiotics improved beneficial gut microbiota and cognitive skills, partially reversed hippocampus neuronal damage by lowering brain inflammation and oxidative stress. Glucocorticoids have also been implicated in vitamin K2 deficiency.2 Glucocorticoids can be effective in treatment of many inflammatory and autoimmune diseases in children. In this study, a positive correlation relation was observed between antenatal corticocorticosteroids use and vitamin K2 deficiency. Liu et al21 found that combined dexamethasone and vitamin K administration decreased significantly periventricular-intraventricular hemorrhage. Chen et al7 shown that vitamin K2 may significantly treat GIOP patients through downregulation of osteoblast autophagy and mitophagy. It has been shown that corticosteroids could modulate gut microbiota, and might alter intestinal vitamin K production.22 Other study showed that vitamin K2 increased osteoblastogenesis through the steroid and xenobiotic receptor (SXR), and promoted the accumulation of collagen.23 Solmaz et al24 suggested that combination of vitamin K2 and vitamin D3 on ALL patients during the period of intensive steroid therapy improved certain parameters of bone formation and destruction. Moreover, SGA infants are prone to coagulation abnormalities, including vitamin K-dependent reductions in coagulation factors.25 Accordingly, in the current study, SGA was an independent risk factor of vitamin K2 deficiency.
Vitamin K2, an essential nutritional supplement, plays a beneficial role in osteoporotic bone loss, including glucocorticoid-induced osteoporosis, by increasing osteoblast autophagy/mitochondrial autophagy.7,26 Vitamin K2 is necessary to activate proteins that perform important biological functions in the body, including bone mineralization, cardiovascular protection, brain development, joint health, and body weight.2 Numerous studies have found that long-term vitamin K2 inadequacy would increase risks of the development of cancer, cardiovascular diseases, degenerative diseases of aging, atherosclerosis, soft tissue calcification, and osteoporosis.27,28 One study argued that for patients with long-term antibiotic use, vitamin K2 supplementation is recommended to reduce mortality of related diseases.2 In Japan, vitamin K2 was approved for the treatment of osteoporosis since 1995.29 With a deepening understanding of the biological function of vitamin K2, its application should be more widespread in the future.
Subclinical vitamin K2 deficiency is common and requires the consumption of foods with higher levels of vitamin K2.20 The current findings suggest that vitamin K2 supplementation should be considered in late pregnant women and neonates, particularly those at high risk for vitamin K2 deficiency, including those with a history of antenatal steroid use, SGA, and cesarean section. While the role of vitamin K2 has been highlighted, vitamin K2 is not routinely given in clinical practice. As vitamin K2 is crucial to extrahepatic tissues, it is recommended that vitamin K1 and K2 supplementation be promoted. Further research is required to determine the optimum content of vitamin K2 in infant formula.
Study limitations
There are several limitations to this study. Firstly, because the research is a retrospective single-center study, a well-designed prospective randomized multicenter study is needed. The findings might not be available in other regions. Secondly, this study lacked of long-term follow-up; thus, it is impossible to further explore the prognosis of vitamin K2 deficiency. Based on current evidence, it is not possible to determine the cause and effect of antenatal steroid use and SGA with vitamin K2 deficiency, this is a common limitation of observational studies. Thirdly, the sample size for the current analysis was insufficient to examine all relevant confounding variables. Thus, these findings need to be validated in a larger cohort of pregnant women. Furthermore, basic research should demonstrate the exact mechanism and potential causal relationship of antenatal steroid use and vitamin K2 deficiency.
In conclusion, the present study demonstrated that antenatal corticosteroids use is independently associated with vitamin K2 deficiency. The current findings suggest that vitamin K2 supplementation should be considered in late pregnant women and neonates, particularly those at high risk for vitamin K2 deficiency, including those with a history of antenatal steroid use, SGA, and cesarean section.
Acknowledgment
The authors gratefully acknowledge NATIVE English Editing (https:www.nativeee.com) for the English language editing.
Footnotes
Disclosure. This study was supported by the Affiliated Hospital of Guangdong Medical University Clinical Research Program (LCYJ2020DL01).
- Received February 13, 2023.
- Accepted July 11, 2023.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.