


Abstract
Objectives: To evaluate the prevalence of severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infections among patients receiving in-center hemodialysis (ICHD), the relationship between the IgG antibody levels against the virus and SARS-CoV-2-associated symptoms, hemodialysis adequacy, and the antihypertensives used in order to control blood pressure.
Methods: A prospective observational study was carried out at a tertiary care center, King Fahad Kidney Center, Riyadh, Kingdom of Saudi Arabia, between November 2020 and January 2021. A total of 214 ICHD patients with end-stage renal disease (ESRD) were included, and the levels of their anti-SARS-CoV-2 IgG antibodies were assessed after obtaining their informed consent.
Results: Our tests indicated that 15% of the patients in the study’s population had detectable SARS-CoV-2 IgG antibodies, with more than half of them (53%) being asymptomatic. We also found that ESRD patients on angiotensin converting enzyme inhibitors or angiotensin receptor blockers (ACEIs/ARBs) had higher levels of SARS-CoV-2 IgG antibodies than patients not receiving this group of medications.
Conclusion: More studies are required to assess whether patients with a SARS-CoV-2 infection that do not have an indication for being prescribed ACEIs/ARBs would benefit from receiving these medications.
In the midst of the severe acute respiratory syndrome coronavirus- 2 (SARS-CoV-2) pandemic, measures have been taken to lower viral spread in end-stage renal disease (ESRD) patients receiving in-center hemodialysis (ICHD).1,2 Despite these interventions, confirmed SARS-CoV-2 infection rates have been high in hemodialysis (HD) centers, thereby adding pressure on isolation rooms and inpatient beds’ availability.3
Characterization of the human antibody response to SARS-CoV-2 infection is vitally important in interpretation of serological assays for surveillance purposes.4 It has been shown that SARS-CoV-2 IgG antibodies increase from the 11th day after symptom onset and their levels correlate with severity of the infection.5 The specificity rate of IgG was 95%, the negative predictive value of IgG was 94.8%, and the consistency rate of IgG was 88.9%.5 Serum IgG against highly purified receptor-binding domain (RBD) of the SARS-CoV-2 spike protein were found to reach a peak during 21-25 days after illness onset and is a powerful diagnostic tool at later stages of the infection.6 Furthermore, animal studies demonstrated that passive passage of SARS-CoV-2-specific antibodies alter pathogenicity and reduce infection virulence.7,8
According to a research by Zhao J et al,9 there were detectable antibodies in total Ab assays in patients with undetectable RNA in respiratory tract samples obtained on days 1-3 (28.6% [2/7]), day 4-7 (53.6% [15/28]), day 8-14 (98.2% [56/57]), and day 15-39 (100% [30/30]) since illness onset. Moreover, they found that age, gender, and antibody titer were strongly associated independent factors with the clinical classification based on severity. IgG antibodies could help in determining humoral immunity against the infection and are of use in understanding the epidemiology of SARS-CoV-2 infection.9
Our study aimed at evaluating the prevalence of asymptomatic SARS-CoV-2 infections among patient receiving ICHD at King Fahad Kidney Center in Riyadh, Kingdom of Saudi Arabia. We also examined the relationship between the patients’ IgG antibody levels against the virus and parameters such as the patients’ SARS-CoV-2- associated symptoms, their HD adequacy, and the antihypertensives used in order to control their blood pressure.
Methods
This is an observational, prospective, and single-center study. The study included male and female patients with ESRD receiving ICHD at King Fahad Kidney Center in Riyadh, Kingdom of Saudi Arabia. We used Crossref Metadata Search Engine for the literature related to this study.
All patients with ESRD receiving regular hemodialysis in our center were included in the study. Patients with insufficient data were excluded. Consents were obtained from all patients for their data collection and their blood sample for research purposes. Between November 2020 and January 2021, all participants underwent qualitative anti-SARS-CoV-2 IgG antibody testing through the use of SARS-CoV-2 IgG (sCOVG) serology assays (Atellica-IM, Siemens Healthcare Diagnostics Inc. Tarrytown, NY, USA.) according to the manufacturers’ instructions. Laboratory results are presented in numbers in terms of cut-off index (COI) values. The test result is negative if the COI is <1.0 and positive if the COI is ≥1.0.
Subsequently, all positive samples were tested for anti-spike IgG titers with the use of the sCOVG assay that detects IgG antibodies to the receptor-binding domain of the S1 spike antigen of SARS-CoV-2 (anti-S1-RBD Ig). This test is a chemiluminescent immunoassay intended for the semiquantitative detection of IgG antibodies against SARS-CoV-2 in human serum. The analytical measurement interval is stated as 41-140,000 AU/mL, and the positivity cut-off is ≥1,000 AU/mL (as defined by the manufacturer).
The study was approved by the Institutional Review Board as per the National Bioethics Rules and Regulations (Helsinki declaration). The written informed consent was obtained from all the participants. The confidentiality of the data was maintained as per the protocol.
Statistical analysis
The data were analyzed using the Statistical Package for Social Sciences, version 25.0 (IBM, Armonk, NY, USA) for Windows. The categorical variables are presented in the form of frequencies (n) or percentages (%). The associations between the nominal variables are tested through a Chi-squared test. Student’s t-test was used to identify statistically significant differences between the mean values of the categories of each variable for 33 SARS-CoV-2 antibody-positive patients’ log IgG titer values, as these exhibited a normal distribution. The Pearson coefficient of correlation was measured, and univariate and multivariate linear regression models were derived to identify the significant factors for the IgG titer. P-values of <0.05 were considered significant.
Results
Our study group consisted of 214 patients (57% [n=121] males and 43% [n=93] females), with a mean age of 51 years (range: 16-90 years). Of these, 89 (42%) suffered from diabetes mellitus (DM), 185 (86%) suffered from hypertension (HTN), and 16 (7%) suffered from ischemic heart disease (IHD). The age of the patients was classified according to percentiles (P25, P50, and P75; Table 1).
- Patient characteristics for the 214 hemodialysis-receiving patients included in our study.
A total of 33 (15 %) patients were found to be positive for sCOVG antibodies; of these, 64% were males and 36% were females. The typical signs and symptoms of the SARS-CoV-2 infection were noted in 15 (45%) out of the 33 patients. Two patients required oxygen therapy due to SARS-CoV-2, while the majority exhibited only mild symptoms in the form of fever, cough, fatigue, muscle pain, loss of smell, or loss of appetite. The remaining 18 (53%) patients denied a history of SARS-CoV-2-associated symptoms. Furthermore, 9 out of the 33 patients had no prior history of a SARS-CoV-2 infection, and their records showed no previous positive nasopharyngeal swab testing for the infection.
A student’s t-test was used in order to examine the difference in the means between the sCOVG antibodies’ titer and the patients’ age, the patients’ gender, the patients’ SARS-CoV-2 -associated symptoms, their HD adequacy, and the medications used in order to control the blood pressure in these patients (Table 2). Our results revealed that there is no statistically significant difference in the sCOVG antibodies’ titers in relation to the patients’ age (≤60 or >60 years) or gender (p=0.481 and p=0.883). Neither the presence of COVID-19 associated symptoms (p=0.591) nor the requirement for oxygen during the SARS-CoV-2 infection (p=0.544)had an effect on the antibodies’ titer. Comorbidities such as DM, HTN, and IHD did not have an impact on the antibody levels either.
- Mean IgG antibodies’ titer values for 33 patients with coronavirus disease-19.
In order to assess the relationship between the sCOVG antibodies’ titer and the quality of the delivered ICHD, Kt/V was measured among all participants at the same time with the blood sample extraction. We found that 23 (70%) patients had a Kt/V value that was within the recommended target (1.2 and above; Table 2). In our cohort, there was no significant correlation between the titer of the COVID-19 antibodies and the Kt/V (p=0.468).
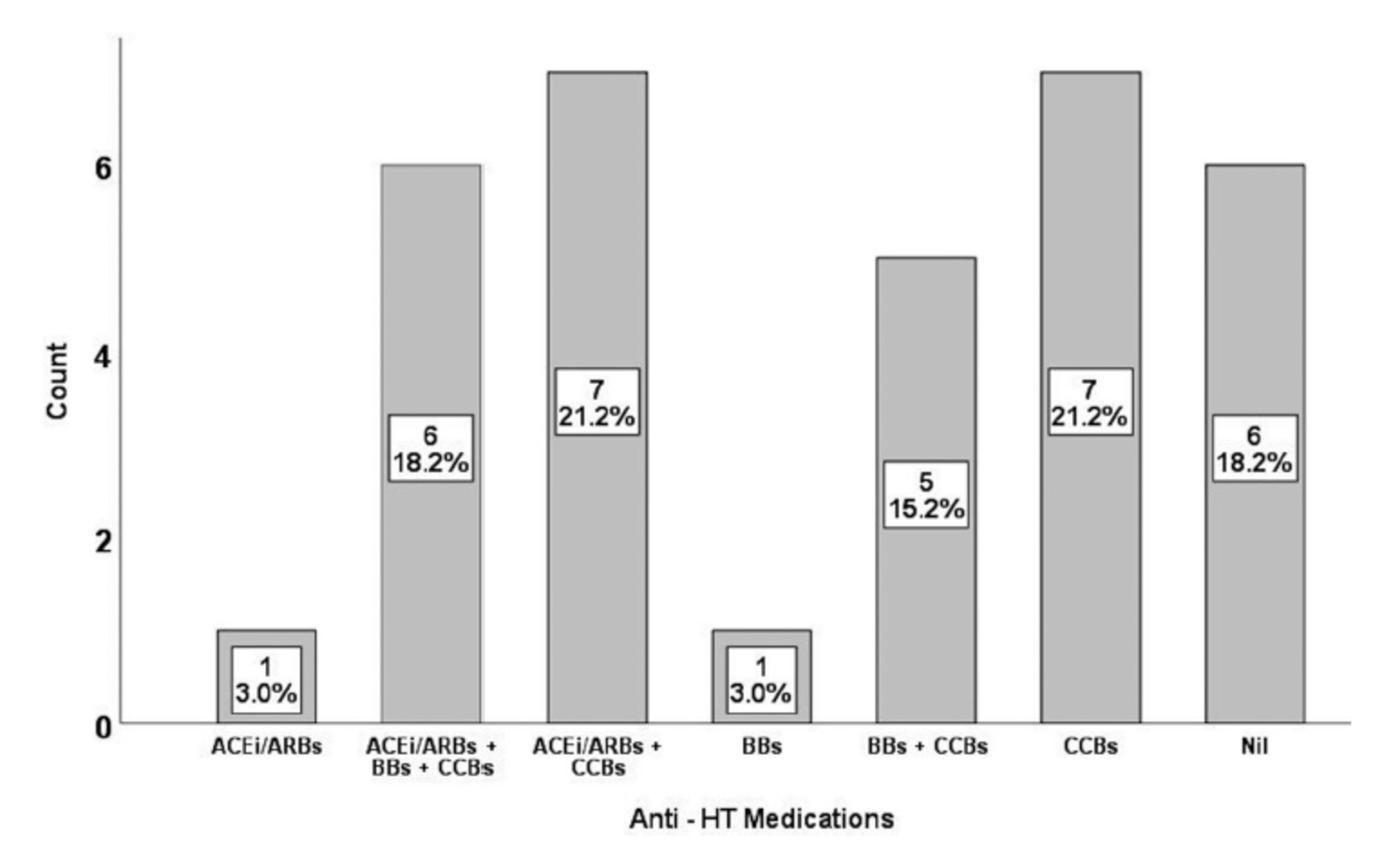
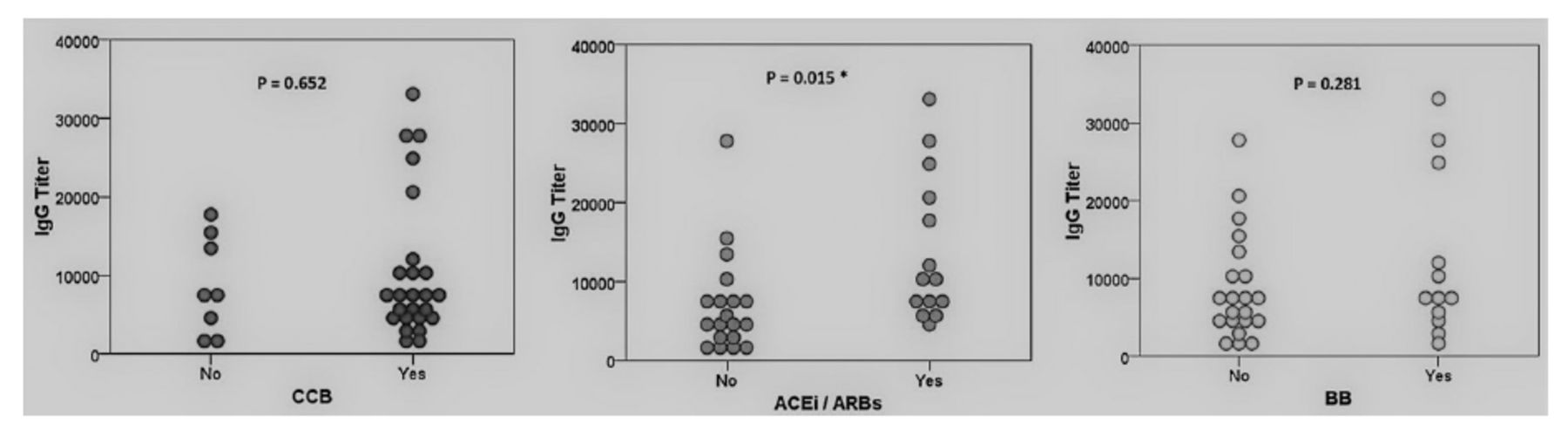
The majority of patients included in our study were hypertensive (88%). An overview of the medications used for the treatment of their HTN is provided in Figure 1. We examined the relationship between the types of the antihypertensive drugs used and the sCOVG antibodies titers (Table 2). A total of 14 out of 33 patients with positive serology were using angiotensin converting enzyme inhibitors or angiotensin receptor blockers (ACEis/ARBs), 7 (50%) were asymptomatic, 6 had mild symptoms, and one patient required oxygen and had severe infection according to the World Health Organization (WHO) classification. The analysis revealed that patients on ACEis/ARBs had significantly higher COVID-19 antibody titers than patients not treated with this group of medications (p=0.015). On the other hand, this association was not found in patients receiving calcium channel blockers (CCBs; p=0.652) or beta blockers (BBs; p=0.281). The distribution of titer values for the 33 COVID-19 antibody-positive patients based on the antihypertensive medication received by the same patients is presented in Figure 2. Our findings suggest that ESRD patients receiving ACEis/ARBs have a better immunological response to a naturally-acquired SARS-CoV-2 infection.

- Overview of the antihypertensives used in our cohort (N=33). Three patients were using hydralazine as a third or fourth medication in order to control their blood pressure. ACEIs/ARBs: angiotensin-converting enzyme inhibitors or angiotensin receptor blockers, BBs: beta-blockers, CCBs: calcium channel blockers

- Effect of the antihypertensive used on the mean coronavirus disease-19 antibodies’ IgG titer. *P-value of <0.05. ACEIs/ARBs: angiotensin-converting enzyme inhibitors or angiotensin receptor blockers, BBs: beta-blockers, CCBs: calcium channel blockers
Univariate linear regression analysis revealed that the addition of ACEis/ARBs on the regimen for the control of blood pressure had significantly increased the titer values by 7,019 AU/mL (Table 3) as compared to those not treated with ACEIs/ARBs (p=0.008).
- Univariate and multivariate linear regression model for 33 coronavirus disease-19 patients.
In the multivariate linear regression analysis model, the combined effect of the exposure variables in Table 3 revealed an amplified COVID-19 IgG antibody titers of 9,523.5 AU/mL in patients treated with ACEIs/ARBs, which was statistically significant (p<0.001).
Discussion
The current standard diagnostic test for the SARS-CoV-2 infection in Saudi Arabia is the identification of the viral ribonucleic acid (RNA) through the undertaking of real-time polymerase chain reaction (RT-PCR) on isolates from the upper respiratory tract swabs of suspected patients.10 However, this test comes with the limitation of potentially generating false negative results.11,12 Carrying out SARS-CoV-2 nasopharyngeal swabs for RT-PCR based on symptoms had the drawback of missing a good proportion of asymptomatic patients.13 On the other hand, the implementation of serology for the identification of SARS-CoV-2 IgG antibodies through the use of enzyme-linked immunosorbent assay can be particularly useful in identifying previous infections with high sensitivity (81%) and specificity (96%).14
Patients on HD are at higher risk of acquiring a SARS-CoV-2 infection. A study that was carried out on ESRD patients on ICHD has found that 79 (22%) out of 356 patients tested positive for SARS-CoV-2 through RT-PCR and 129 (36%) through the measurement of IgG antibodies.13 The high prevalence of SARS-CoV-2 infection in ESRD patients on ICHD was also reported in multiple HD centers in Al-Madinah Al-Munawarah, Saudi Arabia.14 In our study, we found an overall SARS-CoV-2 seroprevalence of 15% in ESRD patients receiving ICHD; 55% of the cases were asymptomatic for the infection, and were only identified as carriers of the infection with the use of either protocol nasopharyngeal swabs (based on exposure) or serological testing during our study. Furthermore, 11 patients in our study had negative nasopharyngeal swabs for SARS-CoV-2 prior to their recruitment. These patients were not isolated and posed a risk of transmitting the infection. Similarly, in a report from 2 units affiliated with the Imperial College Renal and Transplant Center, 40% out of 129 patients undergoing ICHD that were seropositive for a SARS-CoV-2 infection were found to be asymptomatic.13 These findings highlight the challenges faced by healthcare providers in identifying patients that can transmit the infection, and the limitations of nasopharyngeal swabs in identifying people with the infection. Therefore, the clinicians need to constantly alerted in order to avoid an outbreak in the dialysis unit.
Kt/V is a parameter used for the evaluation of the dialysis efficiency in patients on regular ICHD. The minimum recommended Kt/V (as defined by the National Kidney Foundation’s Kidney Disease Outcomes Quality Initiative clinical practice guidelines) is 1.2 and above.15 Two studies in Taiwan have reported a positive correlation between the HD adequacy (as measured by Kt/V) and the seroconversion after an anti-SARS-CoV-2 vaccination in ESRD patients on ICHD.16,17 We were not able to find any study evaluating the HD adequacy and the immune response to naturally-acquired SARS-CoV-2 infection in ESRD patients receiving ICHD. In our study, we could also not find a statistically significant relationship between the titers of the sCOVG antibodies post infection and the Kt/V in ESRD patients on ICHD. This finding suggests that the HD adequacy might play a role in the immune response to the vaccine, but not in the case of the naturally-acquired SARS-CoV-2 infection in ESRD patients.
The angiotensin converting enzyme 2 (ACE2) is known to be one of the main binding receptors for SARS-CoV-2. With the help of its spike protein, the coronavirus binds to host cells that express specific ACE2 receptors. The host cell protease cleaves off the spike protein and thereby facilitates the viral entry and replication.18
The effect of renin-angiotensin system (RAS) blockade on the clinical outcome in COVID-19 patients has been disputed, as some studies suggest beneficial outcomes and others suggest harmful outcomes. In terms of the unfavorable outcomes, Fang et al19 have hypothesized that since RAS blockers increase the ACE2 concentration, they will lead to an increased risk and severity of a SARS-CoV-2 infection in patients with DM and HTN. They have also suggested the use of CCBs as an alternative for the treatment of HTN. Based on a similar hypothesis, Sommerstein et al20 have also raised concerns over the use of ACEIs/ARBs, as they might increase the risk and severity of COVID-19.
On the other hand, several retrospective studies have shown mortality-related benefits in patients with HTN and COVID-19 receiving RAS inhibitors when compared with patients receiving other antihypertensives.21,22 In another study, Freng et al23 concluded that the use of RAS inhibitors had positive outcomes in COVID-19 patients, with reduced length of hospitalization and intensive care unit admissions. It was also demonstrated that patients receiving RAS inhibitors had lower viral loads, but comparable COVID-19-associated antibody levels. Higher antibody levels in patients using ACEIs/ARBs were observed in our study. Our study’s target group was different than those in the aforementioned study, as we only included ESRD patients receiving ICHD.
Study limitations
We consider lack of comparison group from the general population with normal kidney function the main limitation of the study. However, our study was carried out during lock down and it was difficult to recruit healthy individuals for routine antibody screening.
In conclusion, despite our efforts to minimize the risk of transmission of SARS-CoV-2 in our HD center, we found a high prevalence of the infection in our center (15%). This could be attributed to the fact that many of our patients were asymptomatic, and the limitations of nasopharyngeal RT-PCR testing in identifying all carriers of the virus. Therefore, one can conclude that a symptom-based screening has a limited utility within HD units when it comes to identifying patients with the infection. Among patients on chronic HD with COVID-19, the use of ACEIs/ARBs was associated with higher levels of COVID-19 IgG antibodies. More studies are required in order to assess whether COVID-19 patients without an indication for being treated with ACEIs/ARBs would benefit from this group of medications.
Acknowledgment
The authors gratefully acknowledge the Research and Innovation Center at King Saud Medical City, Riyadh, Saudi Arabia, for their services, and our research coordinator Ms. Kristine Espinola for her efforts. We also would like to thank Enago for their English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received February 23, 2023.
- Accepted August 1, 2023.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.