


Abstract
Objectives: To evaluate 2 new modifications to medically necessary, time-sensitive (MeNTS) scoring systems integrating functional capacity assessment in estimating intensive care unit (ICU) requirements.
Methods: This prospective observational study included patients undergoing elective surgeries between July 2021 and January 2022. The MeNTS scores and our 2 modified scores: MeNTS-METs (integrated Duke activity status index [DASI] as metabolic equivalents [METs]) and MeNTS-DASI-5Q (integrated modified DASI [M-DASI] as 5 questions) were calculated. The patients’ ICU requirements (group ICU+ and group ICU-), DASIs, patient-surgery-anesthesia characteristics, hospital stay lengths, rehospitalizations, postoperative complications, and mortality were recorded.
Results: This study analyzed 718 patients. The MeNTS, MeNTS-METs, and MeNTS-DASI-5Q scores were higher in group ICU+ than in group ICU- (p<0.001). Group ICU+ had longer operation durations and hospital stay lengths (p<0.001), lower DASI scores (p<0.001), and greater hospital readmissions, postoperative complications, and mortality (p<0.001). The MeNTS-METs and MeNTS-DASI-5Q scores better predicted ICU requirement with areas under the receiver operating characteristic curve (AUC) of 0.806 and 0.804, than the original MeNTS (AUC=0.782).
Conclusion: The 5-questionnaire M-DASI is easy to calculate and, when added to a triage score, is as reliable as the original DASI for predicting postoperative ICU requirements.
Coronavirus disease 2019 (COVID-19) diagnoses in patients with comorbidities are associated with severe COVID-19 illness that requires intensive care unit (ICU) care.1,2 Per global precautions, during the first surge of the COVID-19 pandemic, health authorities in several countries restricted elective surgeries to preserve resources for these critical patients and patients requiring urgent/emergent surgeries. Elective surgeries began to be scheduled after the first peak. The pandemic is now slowing, with fewer new COVID-19 diagnoses, after several surges in peak patient numbers.
Surgical prioritization is challenging under both surging and slowing pandemic conditions. During a pandemic, neither the possibility of overextending limited resources to cover elective cases, jeopardizing the care of infected patients, nor the possibility of disease advancement due to surgery postponement is desired. Furthermore, the post-pandemic era also requires a prioritization scoring system since a surgery backlog is created during the mandatory cancellation and restrictive capacity periods.
Several guidelines have been published for surgical decision and triage.3,4 The medically necessary, time sensitive (MeNTS) scoring system (Appendix 1) comprising parameters evaluating procedure, disease, and patient factors, was proposed by Prachand et al5 and promoted by the American College of Surgeons. Despite some improvements, patient characteristics relating to intensive care and hospital bed occupation and postoperative outcomes were not elucidated in these surgical studies.6-10 As perioperative physicians, anesthesiologists, and intensive care specialists should be involved in resource planning.
We had previously published a significant relationship between high MeNTS scores and moderate to severe outcomes. We speculated that incorporating a cardiovascular functional capacity parameter could improve the scoring system.11 Therefore, this observational, prospective study, carried out under the semi-restrictive status of our institution following the third surge of the pandemic, aimed to compare the original MeNTS scoring system with modified MeNTS scoring systems incorporating functional capacity for the primary outcome of ICU requirement. Our secondary outcomes were hospital stay length, hospital readmission, postoperative complications, and mortality.
Methods
This study was approved by the Ethics Committee of Istanbul Medical Faculty, Istanbul, Turkey (protocol number: 2021/1117) and was carried out in accordance with the Declaration of Helsinki principles. Written informed consent was obtained from all patients prior to participation. This study followed the strengthening the reporting of observational studies in epidemiology (STROBE) reporting guideline.12
The study was carried out in a university hospital, a tertiary center with approximately 25.000 surgeries/year in the pre-pandemic era. Out of 8 ICUs, 4 with a total capacity of 38 beds are managed primarily by anesthesiologists who care for adult postoperative surgical and medical patients. The study period was from July 2021 to January 2022, between the third and fourth surges of the pandemic for our country. The total number of operating rooms were 30 and ICU beds were 25 allocated to surgery during this period. A pandemic ICU also operated with 13 beds employing 8 anesthesiologists/day during this period.
All patients undergoing operation were screened and enrolled if eligible after consenting. This study included elective cases, and case priority was classified according to the need to carry out surgery following admission as urgent-elective (>24 hours but <2 weeks), essential-elective (within 1-3 months), and discretionary elective (>3 months).13 Emergent cases that had to be operated on within 24 hours of admission were excluded from this study. Patients aged <18 years or with whom communication was impossible were also excluded. All enrolled patients were screened for COVID-19 with a symptoms questionnaire, and the nasopharynx was sampled for a polymerase chain reaction (PCR) test.
We recorded the patients’ demographic data, surgery characteristics (including case priority and surgery type), anesthesia characteristics, American Society of Anesthesiologists (ASA) physical status class, malignancy status, smoking history, PCR-test-based COVID-19 screening results, and, if present, the clinical symptoms and signs of COVID-19 (namely, fever, cough, and dyspnea).
The MeNTS scores were calculated for each patient. A senior surgeon on the surgical team carried out the surgical evaluation, which was confirmed by the study surgeon (AFKG).
We computed Duke activity status index (DASI) scores to incorporate functional capacity data into the patient domain in MeNTS scoring.14 However, the 12-item DASI questionnaire is not a scoring system that could be divided into 5 or fewer parts and added easily to the patient domain of MeNTS because of the non-uniform weight of each item.
Therefore, the DASI was incorporated in 2 ways. In the first method, functional capacity computed by DASI was converted into metabolic equivalents (METs) using the formula: ([0.43×DASI]+9.6)/3.5.15 In this MeNTS-METs scoring system, an additional row categorized according to METs values was inserted into patient factors (5 points= <4 METs; 4 points= ≥4 and <7 METs; 2 points= ≥7 and <9.89 METs; and one point= 9.89 METs, Appendix 2). In the second method, a simplified (modified) DASI comprising 5 questions (M-DASI-5Q) was calculated as suggested by Riedel et al.16 In the MeNTS-DASI-5Q scoring system, the additional row was based on the number of questions answered positively: 5 points= none/one positive answer; 4 points= 2 positive answers; 3 points= 3 positive answers; 2 points= 4 positive answers; and one point= all questions answered positively (Appendix 3).
Anesthesia method (general, neuraxial, and peripheral nerve block), operation duration, ICU requirement (planned or unplanned), total hospital stay length, and rehospitalization were recorded. Planned ICU admissions were decided by the consultant anesthesiologist in charge of that operating theatre according to the patients’ comorbidities and surgical characteristics. Unplanned admissions immediately after the operation due to intraoperative complications were decided by the same consultant. Unplanned ICU admissions from the ward due to postoperative complications were decided by the consultant anesthesiologist in charge of the ICU.
Postoperative complications were analyzed and classified in severity according to Clavien-Dindo (CLD) classification.17 Postoperative pulmonary complications (PPCs), major adverse cardiac and cerebrovascular events (MACCEs), mortality within the first postoperative month, and postoperative COVID-19 infection within 14 days were recorded.18,19
Statistical analysis
In this exploratory study, we attempted to screen and approach all cases since the period between the third and fourth surges was unknown. Therefore, no sample size calculation was possible.
Patients were classified into 2 groups as group ICU+ and group ICU- according to their postoperative ICU requirements. Data are expressed as mean ± standard deviation (SD), median (interquartile range [IQR]), or number and precentages (%). The Shapiro-Wilk and Kolmogorov-Smirnov tests were used to assess the normality of quantitative data distributions. Student’s t-test was used to compare normally distributed data, while the Mann-Whitney-U test was used to compare non-normally distributed data. Where applicable, the mean difference and its 95% confidence interval (CI) are also given. Chi-square tests were used to compare qualitative data. Receiver operating characteristic (ROC) curves were created. The area under the ROC curve (AUC) was calculated to assess the predictive accuracy of MeNTS, MeNTS-METs, and MeNTS-DASI-5Q scores for the ICU requirement. Receiver operating characteristic curves were interpreted according to their AUC: poor= 0.60-0.69; fair= 0.70-0.79, good= 0.80-0.89; and excellent= ≥0.90. Statistical analysis was carried out using the Statistical Package for the Social Sciences, version 21.0 (IBM Corp., Armonk, NY, USA).
Results
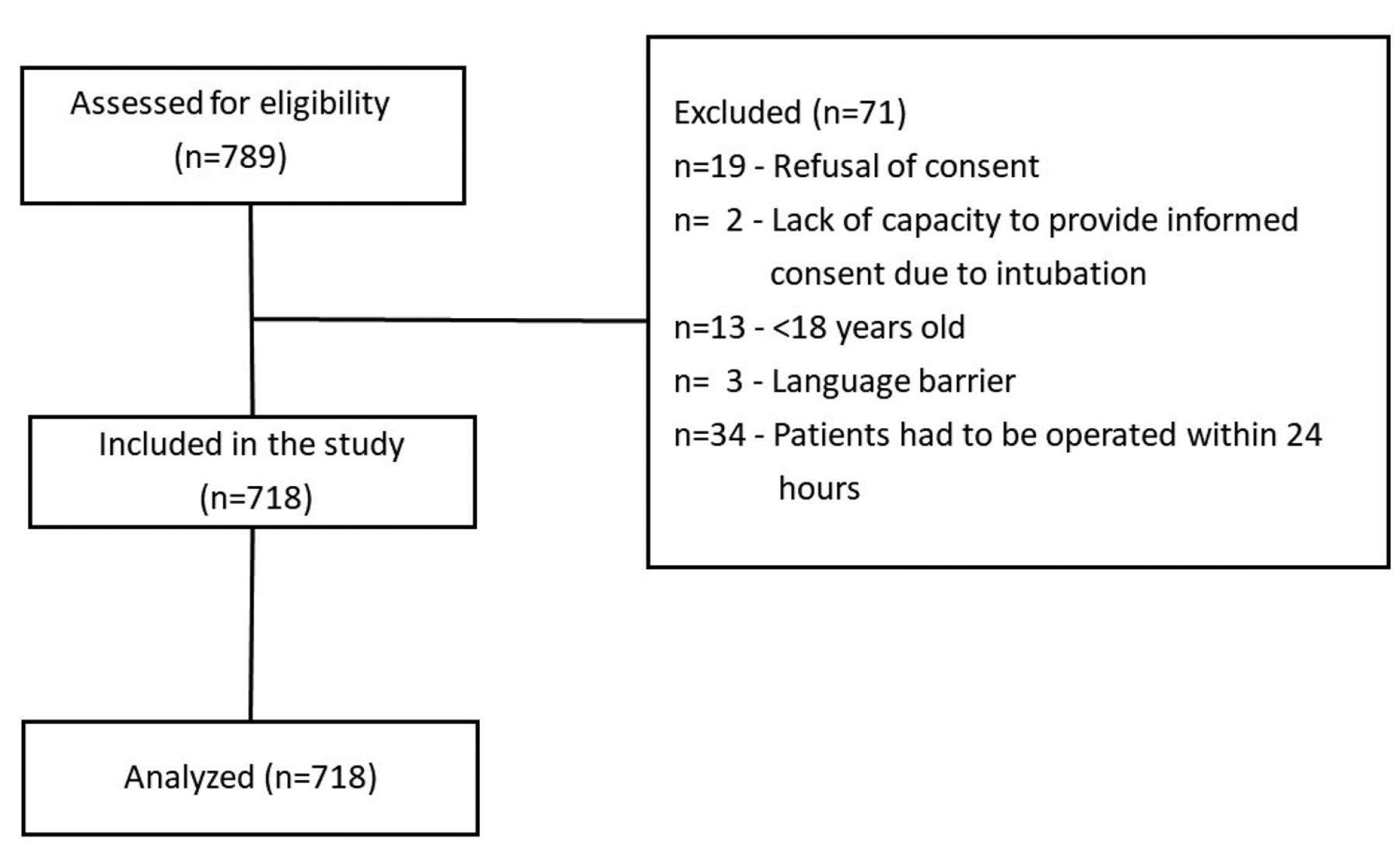
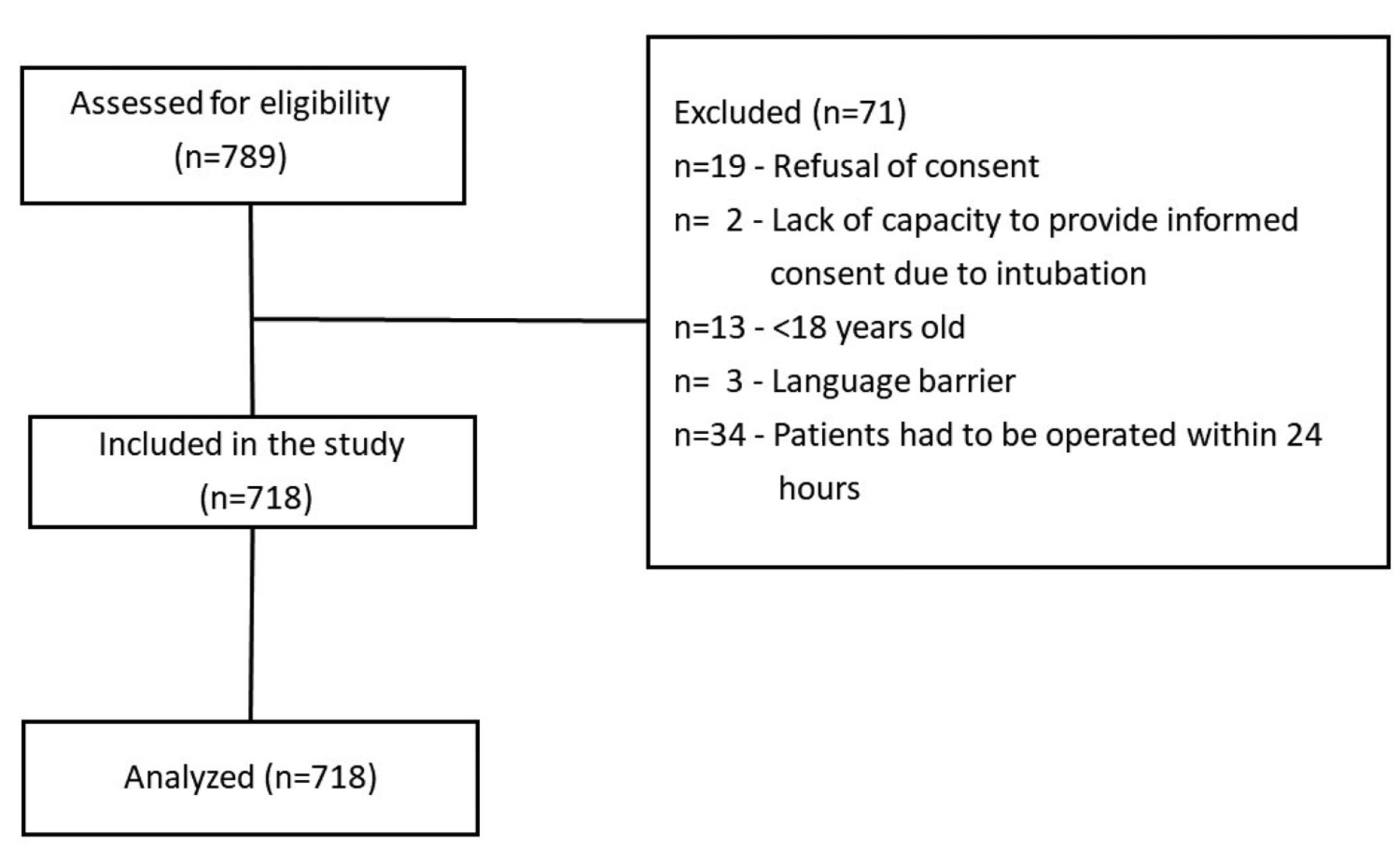
This prospective study screened 789 patients, of which 718 were included in the analysis (Figure 1). Case priority was listed as urgent-elective for 151 (21.0%), essential elective for 458 (63.8%), and discretionary elective for 109 (15.2%) patients. Patients’ surgical characteristics are shown in Table 1. For 22 (3.1%) patients, COVID-19 PCR tests were negative preoperatively but positive postoperatively with repeated testing; 11 had a COVID-19 infection during their hospital stay, of which 5 needed ICU care, and 3 died. A total of 11 of 22 patients were infected within the first 14 days after discharge; and 2 were rehospitalized and discharged without complications.
- Flow diagram.
- Patients’ surgical characteristics.
The participants’ median age was 48 (35-62) years, their mean body mass index (BMI) was 26.96±5.21 kg/m2, and 287 (40%) were male. Their mean MeNTS score was 49.93±8.30, and their median DASI score was 44.70 (26.95-58.20). The mean MeNTS-METs score was 52.33±8.92 and the mean MeNTS-DASI-5Q score was 52.45±8.89. General anesthesia was carried out for 594 (82.7%) patients, while neuraxial anesthesia was used alone for 98 (13.6%) patients and peripheral nerve blocks was used for 26 (3.6%) patients. The median operation time was 110 (65-180) minutes.
The group ICU+ comprised 178 (24.8%) patients, of which 12 were unplanned; 6 were admitted due to intraoperative complications, while the other 6 were admitted from the ward due to postoperative complications. Table 2 compares demographics, preoperative and intraoperative characteristics, DASI scores, the 3 different MeNTS scores with subdomains (procedure, disease, and patient factors), total hospital stay lengths, and rehospitalization rates in goup ICU+ and group ICU-.
- Comparison of group intensive care unit (-) and group intensive care unit (+).
When the subdomains of all 3 types of MeNTS scores were compared between groups ICU+ and ICU-, patients requiring an ICU stay had more complicated procedures with increased procedure domain scoring, operations requiring urgency with decreased disease domain scoring, and concomitant diseases with increased patient domain scoring (Table 2). Since the MeNTS-METs and MeNTS-DASI-5Q scores only change due to patient domain scoring, group ICU+ had higher patient domain scores for both MeNTS-METs and MeNTS-DASI-5Q (Table 2).
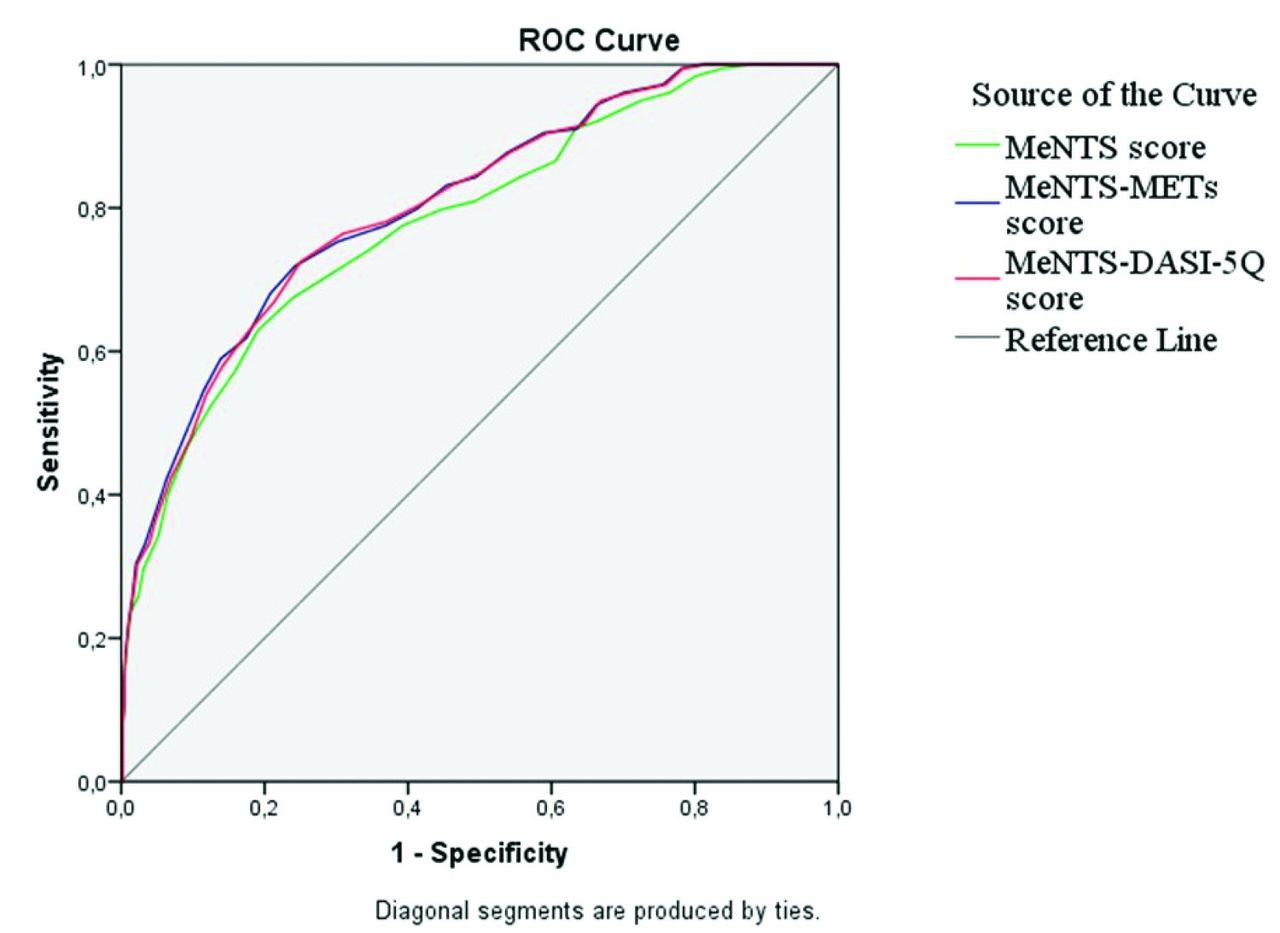
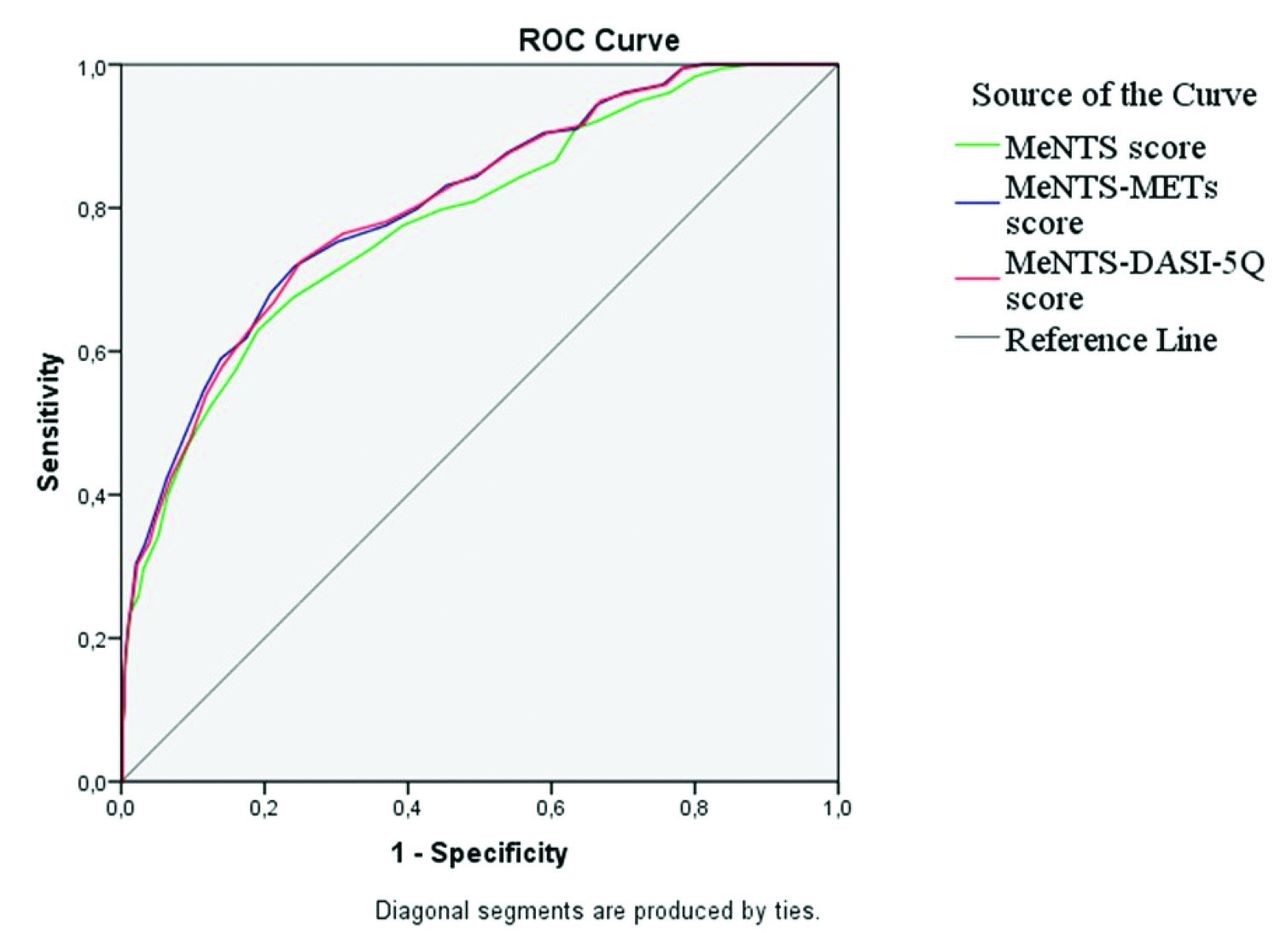
Figure 2 shows the ROC curves representing the carrying out of MeNTS, MeNTS-METs, and MeNTS-DASI-5Q scores for predicting ICU requirements. Area under the curves were good for the MeNTS-METs (AUC=0.806) and MeNTS-DASI-5Q (AUC=0.804) scores but fair for the original MeNTS score (AUC=0.782).
- Receiver operating characteristic (ROC) curve determining the carrying out of MeNTS, MeNTS-METs, and MeNTS-DASI-5Q score for predicting ICU requirement. Area under the curve (AUC)=0.782 (95% CI: [0.742-0.822]) for MeNTS score. Area under the curve=0.806 (95% CI: [0.769-0.843]) for MeNTS-METs, and AUC=0.804 (95% CI [0.766-0.841]) for MeNTS-DASI-5Q.
Postoperative complication severity, PCCs, MACCEs, and mortality in groups ICU+ and ICU- are shown in Table 3. Postoperative pulmonary complications were observed in 44 (6.1%) patients, of which 13 had 2 or more pulmonary complications, while postoperative MACCEs were observed in 22 (3.1%) patients. Three patients had pulmonary embolisms: 2 during their ICU stay and one on the ward on the ninth postoperative day, necessitating admittance to the ICU.
- Comparison of group intensive care unit (-) and group intensive care unit (+).
Median MeNTS scores were higher in patients with PPCs (58 [52.50-62] vs. 50 [44-55], p<0.001) and with MACCEs (57 [51-60] vs. 50 [44-56], p<0.001). The MeNTS, MeNTS-METs, and MeNTS-DASI-5Q subdomains were analysed according to the presence of PPCs and MACCEs (Table 4). According to Clavien-Dindo (CLD) classification, the total MeNTS scores were higher in patients with CLD ≥II than CLD <II (55 [48-61] vs. 49 [44-54], p<0.001). Mortality was observed in 9 (5.1%) patients and higher median MeNTS scores were calculated in these patients compared to survivors (58 [50.50-65] vs. 50 [44-56], p=0.018).
- Comparison according to the subdomains of medically necessary, time-sensitive, medically necessary, time-sensitive-metabolic equivalents, and medically necessary, time-sensitive-Duke activity status index-5 questions in patients with or without pulmonary and cardiovascular complications.
Discussion
In this study, we found that MeNTS scores were higher in patients requiring ICU care than in patients not requiring ICU care. Furthermore, the MeNTS scoring system incorporating functional capacity had better predictive accuracy for estimating ICU needs.
Determination of surgical patients requiring ICU admission is important. While underestimated admission might cause inadequate patient care on the ward, overestimation might misuse critical resources with increased stay length and costs.20 The ongoing COVID-19 pandemic further exacerbates this conundrum. In acute surges, prioritizing essential surgeries and predicting postoperative outcomes, ICU requirements, and prolonged stays are crucial for resource allocation strategies. Prioritization is also crucial in the remission era since a surgery backlog exists due to deferred cases, which can cause logistical and clinical challenges in an overloaded healthcare system.21,22 However, there are few tools to quantify prioritization.2-4,23 One of the most well-known tools is the MeNTS scoring system proposed by Prachand et al.5 It has been studied with several modifications to its surgical and patient domains in different surgery types and compared with other prioritization scales as detailed in Appendix 4.6-10,24-28 However, these studies have not focused on patient outcomes and ICU resource utilization.
In this study, we observed higher MeNTS scores than the full restriction period during the early phase of the pandemic.11 This finding is simply because increased operating room capacity and ICU beds result in more essential and discretionary elective surgeries. This dynamic change in prioritization due to resource availability and pandemic status had been predicted by Prachand et al.5
The MeNTS scoring can be discussed in terms of domains. The procedure domain mainly questions the severity and extensiveness of the operation. Procedure-related scores were higher in group ICU+ than in group ICU-. This finding is unsurprising since operation duration was longer in group ICU+, in which malignancy was also more prevalent, similar to other ICU admissions after non-cardiac major surgery.29,30 Notably, since one parameter of procedure factors is ICU need anticipation, ICU need for planned admissions may become a self-fulfilling prophecy. That is, high preoperative surgery anticipation may increase both the MeNTS score preoperatively and the frequency of our primary outcome postoperatively. Moreover, the anesthesia type may affect the procedure domain since general anesthesia and intubation increase procedure-related and total scores. We observed that patients with regional anesthesia had less ICU utilization, consistent with a meta-analysis that stated patients with regional anesthesia had decreased ICU admission odds.31 However, when patients with and without pulmonary and cardiovascular complications are compared, there is a marked increase in procedure-related scores, showing that other factors than ICU need anticipation are involved.
For the disease domain, group ICU+ had lower scores than group ICU-, indicating more patients in group ICU+ had limited non-surgical treatment options, and surgery could not be delayed without aggravating surgical difficulty or worsening outcomes. Moreover, patients with PPCs and MACCEs also had lower disease domain scores than those without complications, further showing that urgent surgery is associated with higher complications. Urgent surgeries have higher complication and mortality rates than elective surgeries, which can also explain the increased use of ICU resources by these patients.20,32
Finally, for the patient domain, group ICU+ had higher scores than group ICU- since patients needing ICU care were older, had higher ASA classes, and were frequent smokers, possibly indicating more comorbidities. Indeed, advanced age, prehospital comorbidities, higher ASA class, and elevated BMI were associated with more frequent ICU requirements postoperatively.29,30,33 In our study, the insignificant difference in BMI between group ICU+ and group ICU- is likely due to the relatively low number of obese or morbidly obese patients. We previously criticized the patient domain of MeNTS scoring since it is based on the presence of a limited number of comorbidities.11 Furthermore, the severity of comorbidities is determined from drug consumption rather than functional capacity measurements. Functional capacity is crucial for predicting perioperative risks and complications in surgical patients and can be incorporated by ASA physical status classification or DASI scores.34 While ASA classification had been incorporated into the MeNTS-OS scoring system in orthopedic surgery, all other patient domain items were excluded, which can be misleading since ASA classification is subject to substantial interobserver variability in score assignment.9,20,35
The DASI is a 12-item cardiopulmonary fitness index. Lower scores (<34) are associated with moderate-to-severe complications and new disability after elective non-cardiac operations.36 Integrating the DASI score into the preoperative assessment of surgical patients was suggested for estimating moderate to severe perioperative risks.36,37 In colorectal surgeries, patients with lower DASI scores had more overall and severe postoperative complications and more frequent hospital readmissions.38 We also found lower DASI scores in group ICU+ than in group ICU-. Furthermore, patient subdomain scores of the MeNTS and our 2 modifications were higher in patients with than without PPCs and MACCEs since comorbidities are also known to be associated with postoperative complications.39,40
Our study proposed incorporating patients’ functional status based on the DASI and tested its prognostic value for ICU resource planning. We added the original DASI as a METs value or the abbreviated 5-questionnaire DASI to the patient domain. We preferred not to exclude any item from the original MeNTS score. We did not incorporate ASA classification as proposed in MeNTS-OS.9 Instead, we preferred DASI scoring since the presence of disease is part of the ASA classification, which may cause the same data to incorrectly increase its weight in patient factor component scoring.
The DASI is not an easy score to compute preoperatively, especially with time and personnel shortages in the perioperative period. While the abbreviated 5-question DASI (M-DASI-5Q) does not fully reflect the main aggregated score information, it was similar to the original 12-question DASI in predicting anaerobic threshold and peak oxygen consumption. The M-DASI-5Q was advocated as a basic screening instrument for preoperative assessment of cardiopulmonary exercise testing to guide perioperative patient management.16 Our 2 modified MeNTS scores predicted the ICU requirement and ICU stay of ≥48 hours better than the original MeNTS score. Since both modified scores had similar predictive values, M-DASI-5Q integration can be preferred to the original scoring. Total MeNTS scores were higher in patients with moderate-to-severe postoperative complications than in patients with mild/no complications. As expected, hospital stays were prolonged and rehospitalization was more frequent in group ICU+, similar to other publications.29,30
While the COVID-19 pandemic is still ongoing, the number of patients diagnosed with COVID-19 is substantially lower than during its major surges. Elective surgery prioritization could be adapted to any situation with limited resources, not just pandemics. We showed that postoperative resource utilization could be predicted better when the functional capacity assessment was added to a triage score.
Study limitations
First, while all surgical specialties except ophthalmology were included, the surgical specialty distribution was not homogenous. Secondly, we included 718 patients who underwent elective operations, which might be low for analyzing ICU requirements. However, our study was limited to the period between the third and fourth surges of the pandemic which we had semi-restricted capacity; we stopped including patients at the beginning of the new surge. Prioritization which also assesses the functional capacity might be used in other resource-limited conditions. On the other hand, it is essential to note that this was a single-center exploratory study, and therefore, the findings might not be generalizable for other different settings and it could be accepted as a limitation. To validate the predictive accuracy of the modified MeNTS scores in various settings, prospective multicenter studies should be carried out. Finally, we did not carry out an actual cost analysis for ICU resource utilization expenses.
In conclusion, determining functional capacity during the perioperative process might help the clinician estimate postoperative patient outcomes. Additionally, incorporating functional capacity into a surgical triage scoring system might improve the prediction of resource utilization. The 5-questionnaire modified DASI is an easier score to compute. Its results were similar to the original DASI when added to an elective surgery triage scoring system to estimate ICU needs. Therefore, this easy adaptation could be applied in priority scoring.
Acknowledgment
The authors gratefully acknowledge Cambridge Proofreading LLC (www.proofreading.org) for English language editing.
Appendix
- Medically necessary, time-sensitive scoring system.5
- Patient factors domain of MeNTS-METs score.
- Patient factors domain of MeNTS-DASI-5Q score.
- MeNTS scoring system and characteristics of related studies.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 2, 2023.
- Accepted August 14, 2023.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.