


Article Figures & Data
Figures
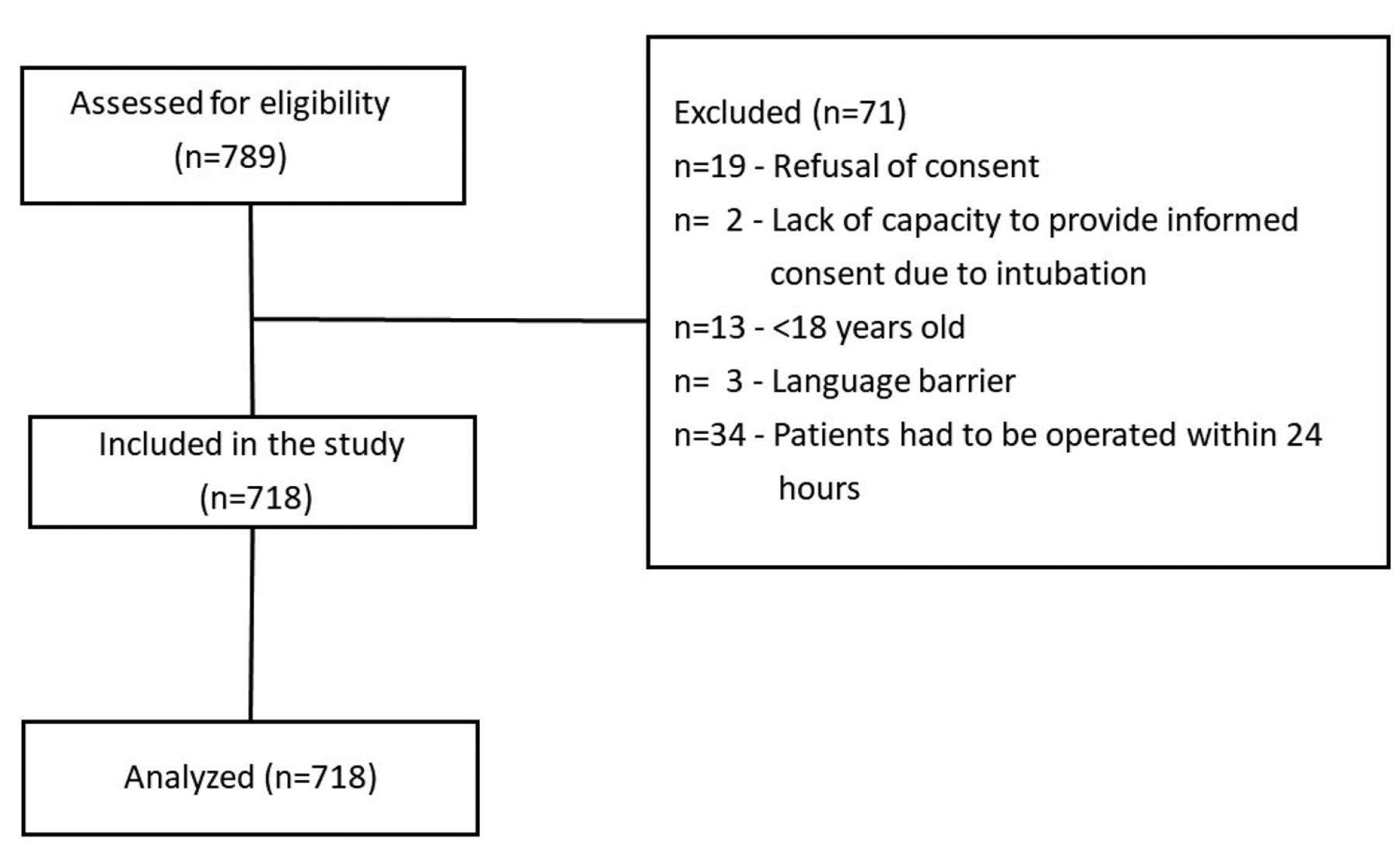
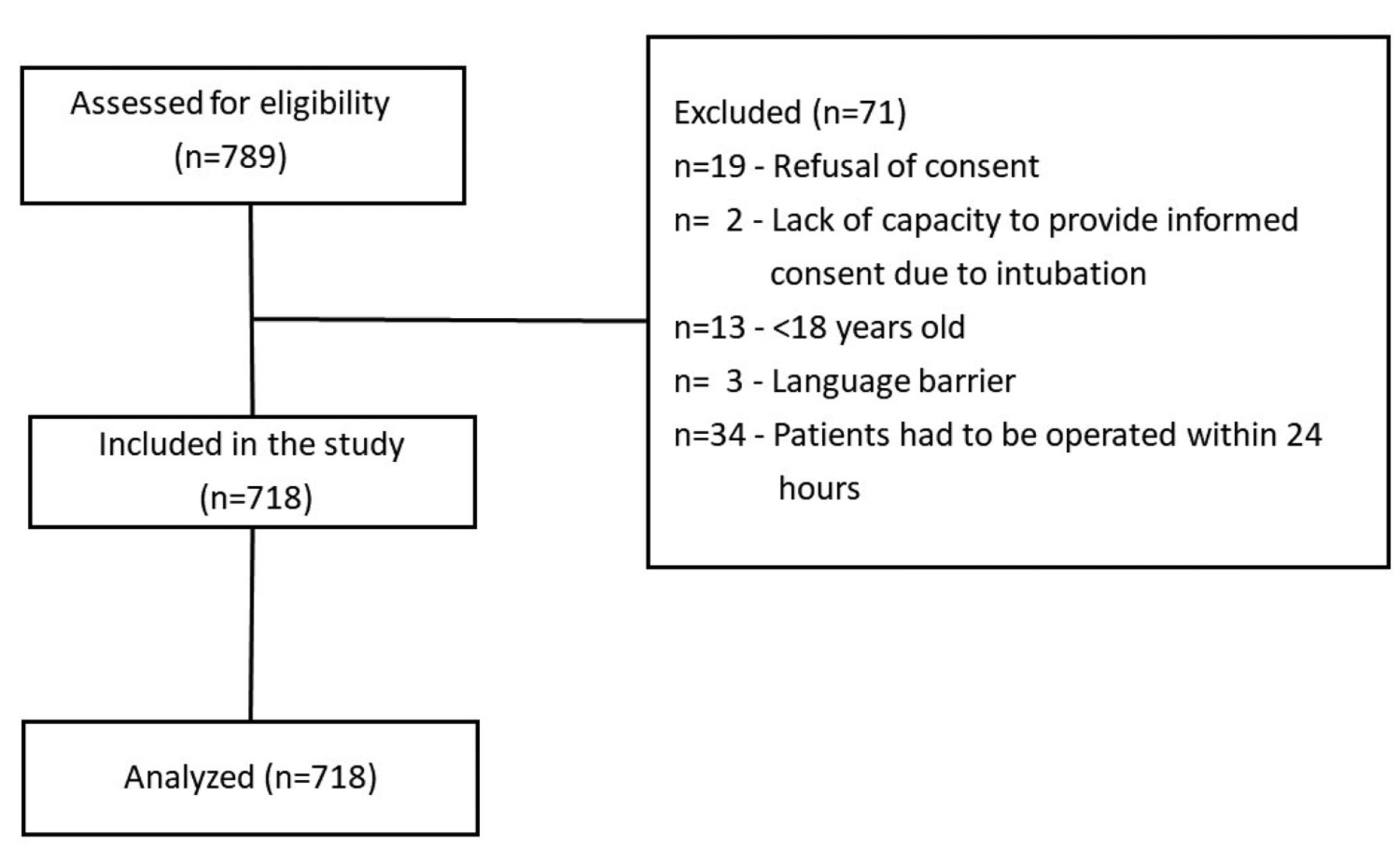
- Figure 1
- Flow diagram.
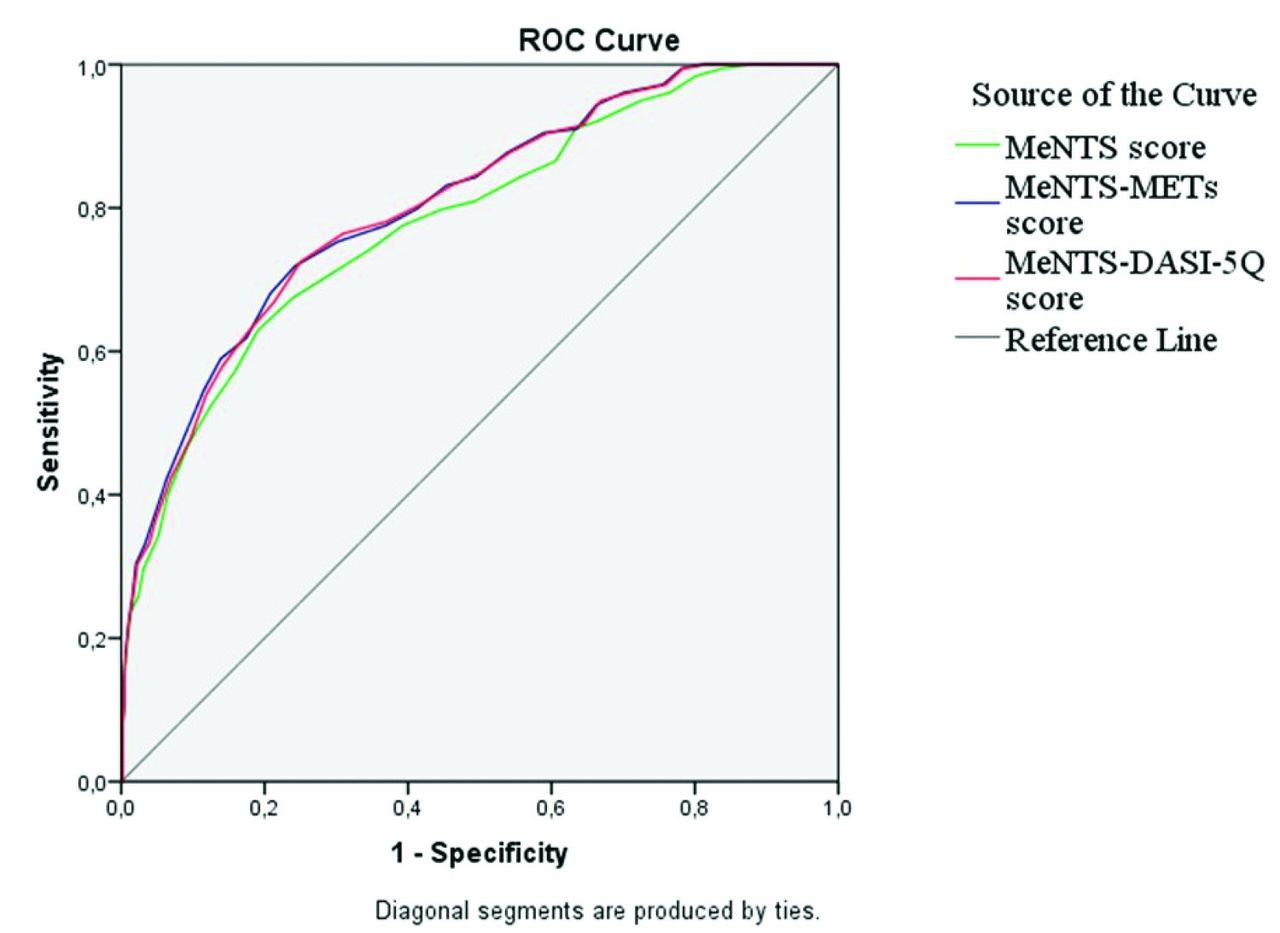
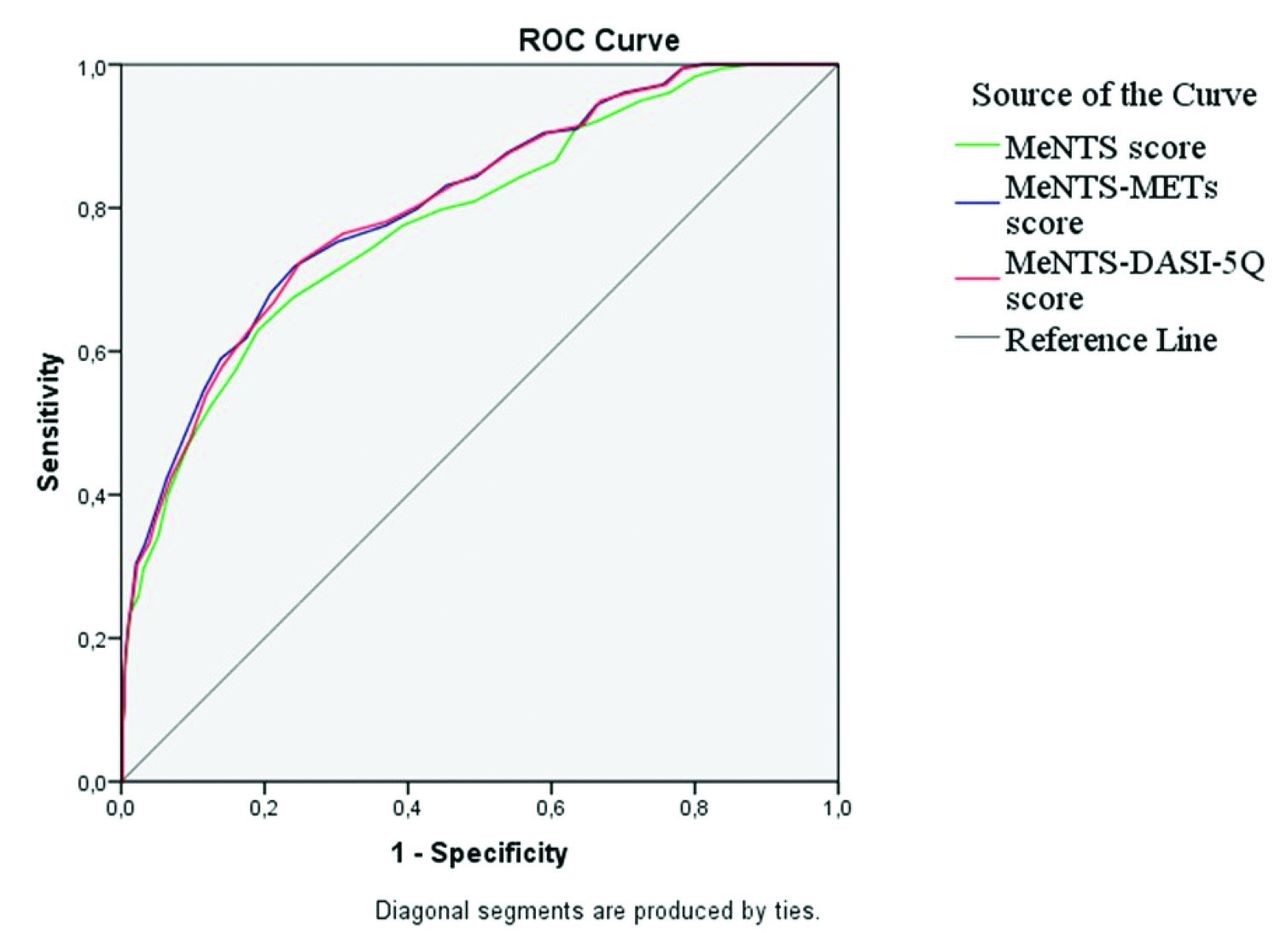
- Figure 2
- Receiver operating characteristic (ROC) curve determining the carrying out of MeNTS, MeNTS-METs, and MeNTS-DASI-5Q score for predicting ICU requirement. Area under the curve (AUC)=0.782 (95% CI: [0.742-0.822]) for MeNTS score. Area under the curve=0.806 (95% CI: [0.769-0.843]) for MeNTS-METs, and AUC=0.804 (95% CI [0.766-0.841]) for MeNTS-DASI-5Q.
Tables
Type of surgery n (%) General surgery 235 (32.7) Abdominal 167 (23.3) Breast 29 (4.0) Other 39 (5.4) Orthopedic surgery 101 (14.1) Gynecological and gynecologic oncological surgery 181 (25.2) Neurosurgery 55 (7.7) Ear-nose-throat surgery 54 (7.5) Plastic surgery 16 (2.2) Thoracic surgery 18 (2.5) Cardiovascular surgery 10 (1.4) Urology 48 (6.7) Values are presented as numbers and precentages (%).
Parameters Group ICU- (n=540) Group ICU+ (n=178) P-values Mean (95% CI) Age, years, median (IQR) 43 (32-56) 62.50 (51.75-70) <0.001 Gender, male 195 (36.1) 92 (51.7) <0.001 ASA physical status class <0.001 ASA 1 153 (28.3) 12 (6.7) ASA 2 358 (66.3) 89 (50.0) ASA 3 29 (5.4) 68 (38.2) ASA 4 0 (0.0) 9 (5.1) BMI (kg/m2), mean±SD 26.81±4.89 27.39±6.08 0.196 Presence of smoking 171 (31.7) 71 (39.9) 0.044 Type of anesthesia 0.016 General anesthesia 435 (80.6) 159 (89.3) Central nerve block-spinal 85 (15.7) 13 (7.3) Peripheral nerve block 20 (3.7) 6 (3.4) Duration of operation (min), median (IQR) 90 (60-138.75) 180 (120-300) <0.001 Malignancy 103 (19.1) 70 (39.3) <0.001 Type of operation <0.001 Urgent-elective 96 (17.8) 55 (30.9) Essential elective 341 (63.1) 117 (65.7) Discretionary elective 103 (19.1) 6 (3.4) DASI score, median (IQR) 50.70 (32.20-58.20) 26.95 (15.45-42.70) <0.001 Length of hospital stay (days), median (IQR) 2 (1-4) 8 (5-14.25) <0.001 Rehospitalization 11 (2.0%) 20 (11.2%) <0.001 MeNTS score, mean±SD 47.86±7.55 56.21±7.28 <0.001 8.35 (7.08-9.62) Procedure factors 18.07±5.03 26.53±3.78 <0.001 8.45 (7.65-9.26) Disease factors 18.47±5.24 15.37±5.54 <0.001 -3.10 (-4.00 - -2.20) Patient factors* 11.23±2.84 14.37±3.69 <0.001 3.13 (2.61-3.66) MeNTS-METs score, mean±SD 49.91±7.95 59.64±7.62 <0.001 9.72 (8.39-11.06) Patient factors-METs* 13.34±3.69 17.67±4.66 <0.001 4.33 (3.66-5.00) MeNTS-DASI-5Q score, mean±SD 50.07±7.94 59.69±7.61 <0.001 9.62 (8.28-10.95) Patient factors-DASI-5Q* 13.44±3.77 17.84±4.64 <0.001 4.40 (3.72-5.08) Values are presented as numbers and precentages (%), mean ± standard deviation (SD), or median interquartile range (IQR).
↵* Only patient factors domain was modified in MeNTS-METs and MeNTS-DASI-5Q scoring systems. Procedure and disease domains were not changed.
ICU: intensive care unit, CI: confidence interval, ASA: American Society of Anesthesiologists, BMI: body mass index, DASI: Duke activity status index, MeNTS: medically necessary, time-sensitive, METs: metabolic equivalents, 5Q: 5 questions
Parameters Group ICU- (n=540) Group ICU+ (n=178) P-values Clavien-Dindo ≥II 52 (9.6) 97 (54.5) <0.001 PPCs* 6 (1.1) 38 (21.3)† <0.001 Respiratory infection (n=19) 5 (0.9) 14 (7.9) Respiratory failure (n=5) 0 (0.0) 5 (2.8) Pleural effusion (n=9) 1 (0.2) 8 (4.5) Atelectasis (n=14) 2 (0.4) 12 (6.7) Pneumothorax (n=2) 0 (0.0) 2 (1.1) Bronchospasm (n=1) 0 (0.0) 1 (0.6) Aspiration pneumonitis (n=4) 0 (0.0) 4 (2.2) MACCEs 3 (0.6) 19 (10.7)‡ <0.001 Acute myocardial infarction (n=3, one mortal) 0 (0.0) 3 (1.7) Congestive heart failure (n=3) 0 (0.0) 3 (1.7) New cardiac arrhythmia (n=8) 2 (0.4) 6 (3.4) Angina (n=6) 1 (0.2) 5 (2.8) Stroke (n=2) 0 (0.0) 2 (1.1) Mortality 0 (0.0) 9 (5.1) <0.001§ Values are presented as numbers and precentages (%).
↵* Thirteen of 44 patients had two or more pulmonary complications.
↵† Two of the patients with PCC in group ICU+ had unplanned admission.
↵‡ One of the patients with MACCE in group ICU+ had unplanned admission.
↵§ Fisher-exact test.
ICU: intensive care unit, PCCs: postoperative pulmonary complications, MACCEs: major adverse cardiac and cerebrovascular events
- Table 4
- Comparison according to the subdomains of medically necessary, time-sensitive, medically necessary, time-sensitive-metabolic equivalents, and medically necessary, time-sensitive-Duke activity status index-5 questions in patients with or without pulmonary and cardiovascular complications.
Scores No PCCs (n=674) PCCs (n=44) P-values Mean (95%CI) Procedure domain (MeNTS) 19.75±5.8 26.7±4.5 <0.001 6.96 (5.19-8.72) Disease domain (MeNTS) 17.88±5.4 15.05±5.8 0.001 -2.83 (-4.5 - -1.18) Patient domain (MeNTS) 11.8±3.2 15.18±3.7 <0.001 3.37 (2.3-4.3) Patient domain (MeNTS-METs) 14.13±4.2 18.81±4.54 <0.001 4.68 (3.39-5.97) Patient domain (MeNTS-DASI-5Q) 14.24±4.28 18.93±4.48 <0.001 4.68 (3.37-5.99) Scores No MACCEs (n=696) MACCEs (n=22) P-values Mean (95%CI) Procedure domain (MeNTS) 19.9±5.9 27.5±3.9 <0.001 7.55 (5.06-10.04) Disease domain (MeNTS) 17.8±5.4 14.09±5.6 0.002 -3.73 (-6.05 - -1.4) Patient domain (MeNTS) 11.9±3.33 14.5±3.39 <0.001 2.56 (1.14-3.98) Patient domain (MeNTS-METs) 14.3±4.3 18.18±4.7 <0.001 3.88 (2.04-5.72) Patient domain (MeNTS-DASI-5Q) 14.41±4.38 18.36±4.15 <0.001 3.94 (2.08-5.81) Values are presented as mean ± standard deviation (SD) and mean difference (95% confidence interval [CI]). PCCs: postoperative pulmonary complications, MACCEs: major adverse cardiac and cerebrovascular events, MeNTS: medically necessary, time-sensitive, METs: metabolic equivalents, DASI: Duke activity status index, 5Q: 5 questions
Variables 1 2 3 4 5 Procedure factors OR time (min) <30 31-60 61-120 121-180 ≥181 Estimated LOS Outpatient <23 h 24-48 h 2-3 d ≥4 d Postoperative ICU need (%) Very unlikely <5 5-10 11-25 >25 Anticipated blood loss (cc) <100 100-250 250-500 500-750 ≥751 Surgical team size (n) 1 2 3 4 5 Intubation probability (%) ≤1 1-5 6-10 11-25 >25 Surgical site None Abdomino-pelvic MIS Abdomino-pelvic open surgery, infraumbilical Abdomino-pelvic open surgery, supraumbilical OHNS/upper GI/thoracic Disease factors Nonoperative treatment option effectiveness None available Available, <40% as effective as surgery Available, 40-60% as effective as surgery Available, 61-95% as effective as surgery Available, equally effective Nonoperative treatment option resource/exposure risk Significantlyworse/not applicable Somewhat worse Equivalent Somewhat better Significantly better Impact of 2-wk delay in disease outcome Significantly worse Worse Moderately worse Slightly worse No worse Impact of 2-wk delay in surgical difficulty/risk Significantly worse Worse Moderately worse Slightly worse No worse Impact of 6-wk delay in disease outcome Significantly worse Worse Moderately worse Slightly worse No worse Impact of 6-wk delay in surgical difficulty/risk Significantly worse Worse Moderately worse Slightly worse No worse Patient factors Age, years <20 21-40 41-50 51-65 >65 Lung disease (asthma, COPD, CF) None - - Minimal (rare inhaler) >Minimal Obstructive sleep apnea Not present - - Mild/moderate (no CPAP) On CPAP CV disease (HTN, CHF, and CAD) None Minimal (no meds) Mild (one med) Moderate (2 meds) Severe (≥3 meds) Diabetes None - Mild (no meds) Moderate (PO meds only) >Moderate (insulin) Immuno-compromised* No - - Moderate Severe ILI symptoms† None (asymptomatic) - - - Yes Exposure to a COVID-19 person in past 14 days No Probably not Possibly Probably Yes ↵* Hematologic malignancy, stem cell transplant, solid organ transplant, active/recent cytotoxic chemotherapy, anti-TNFa or other immunosuppressants, >20 mg prednisone equivalent/day, congenital immunodeficiency, hypogammaglobulinemia on intravenous immunoglobulin, and AIDS.
↵† Such as fever, cough, sore throat, body aches, and diarrhea.
OR: operating room, min: minutes, LOS: length of stay, h: hours, d: days, ICU: intensive care unit, MIS: minimally invasive surgery, OHNS: otolaryngology, head & neck surgery, GI: gastrointestinal, wk: week, COPD: chronic obstructive pulmonary disease, CF: cystic fibrosis, CPAP: continuous positive airway pressure, CV: cardiovascular, HTN: hypertension, CHF: congestive heart failure, CAD: coronary artery disease, meds: medication, PO: by mouth, ILI: influenza-like illness, COVID-19: coronavirus disease-19
Variables 1 2 3 4 5 Patient factors Age <20 21-40 41-50 51-65 >65 Lung disease (asthma, COPD, and CF) None - - Minimal (rare inhaler) >Minimal Obstructive sleep apnea Not present - - Mild/moderate (no CPAP) On CPAP CV disease (HTN, CHF, and CAD) None Minimal (no meds) Mild (one med) Moderate (2 meds) Severe (≥3 meds) Diabetes None - Mild (no meds) Moderate (PO meds only) >Moderate (insulin) Immuno-compromised* No - - Moderate Severe ILI symptoms† None (asymptomatic) - - - Yes Exposure to a COVID-19 person in past 14 days No Probably not Possibly Probably Yes METs‡ =9.89 ≥7 and <9.89 - ≥4 and <7 <4 ↵* Hematologic malignancy, stem cell transplant, solid organ transplant, active/recent cytotoxic chemotherapy, anti-TNFa or other immunosuppressants, >20 mg prednisone equivalent/day, congenital immunodeficiency, hypogammaglobulinemia on intravenous immunoglobulin, AIDS.
↵† Such as fever, cough, sore throat, body aches, and diarrhea.
↵‡ Maximum Duke activity status index: 58.2 [(0.43×DASI+9.6)/3.5] - [(0.43×58.2+9.6)/3.5]=9.89 (maximum METs value calculated according to the equation).
CAD: coronary artery disease, CF: cystic fibrosis, CHF: congestive heart failure, CPAP: continuous positive airway pressure, CV: cardiovascular, HTN: hypertension, ILI: influenza-like illness, med: medication, MeNTS: medically necessary, time-sensitive, METs: metabolic equivalents, PO: by mouth
Variables 1 2 3 4 5 Patient factors Age, years <20 21-40 41-50 51-65 >65 Lung disease (asthma, COPD, and CF) None - - Minimal (rare inhaler) > Minimal Obstructive sleep apnea Not present - - Mild/moderate (no CPAP) On CPAP CV disease (HTN, CHF, and CAD) None Minimal (no meds) Mild (one med) Moderate (2 meds) Severe (≥3 meds) Diabetes None - Mild (no meds) Moderate (PO meds only) > Moderate (insulin) Immuno-compromised* No - - Moderate Severe ILI symptoms† None (asymptomatic) - - - Yes Exposure to a COVID-19 person in past 14 days No Probably not Possibly Probably Yes M-DASI-5Q 1. Are you able to climb a flight of stairs or walk up a hill? 5 positive answers 4 positive answers 3 positive answers 2 positive answers None/one positive answer 2. Are you able to do heavy work around the house? 3. Are you able to do yard work? 4. Are you able to have sexual relations? 5. Are you able to participate in strenuous sports? ↵* Hematologic malignancy, stem cell transplant, solid organ transplant, active/recent cytotoxic chemotherapy, anti-TNFa or other immunosuppressants, >20 mg prednisone equivalent/day, congenital immunodeficiency, hypogammaglobulinemia on intravenous immunoglobulin, AIDS.
↵† Such as fever, cough, sore throat,body aches, diarrhea.
CAD: coronary artery disease, CF: cystic fibrosis, CHF: congestive heart failure, COVID-19: novel coronavirus, CPAP: continuous positive airway pressure, CV: cardiovascular, HTN: hypertension, ILI: influenza-like illness, med: medication, PO: by mouth, M-DASI-5Q: modified Duke activity status index-5 questions,
MeNTS: medically necessary, time-sensitive
Authors Score characteristics/modifications or comparisons of scales Surgery type Operation, disease, and patient factor characteristics and modifications Main findings Prachand et al5 Original described scoring system Non-specified Original operation, disease, and patient factors It was proposed high scores were associated with poorer perioperative patient outcome, increased risk of COVID-19 transmission to the healthcare team, or increased hospital resource use. Slidell et al24 Modified scoring system on pediatric patients (pMeNTS) Paediatric surgery Modified operation and patient factors Same disease factors Adaptation of the adult MeNTS system into a pediatric-specific scoring system better reflected the needs of the pediatric patient population. Dinçer et al11 Original described scoring system General, orthopedic, gynecologic-obstetric, neurosurgery, ear-nose-throat surgery, plastic, cardiovascular, urology, and ophthalmology Original operation, disease, and patient factors MeNTS scores were calculated prospectively and postoperative complications were analyzed. High scores were related with postoperative complications/poorer patient outcome. Cohn et al28 Comparison of questionnaire based (MeNTS), expert opinion based, and individual surgeon based approaches on patient triage Urologic surgery Original operation, disease, and patient factors MeNTS did not meaningfully reflect the triage decision of urologic surgeries. MeNTS, consensus/expert opinion, and individual surgeon based surgical prioritizations disagreed. Waxman et al7 Modified scoring system on CVS interventions (CV-MeNTS) Cardiovascular procedures in the Catheterization Laboratory Modified operation, disease, and patient factors CV-MeNTS could be a useful tool for the prioritization of CV procedures in a period with limited capacity. Marfori et al6 Assessment of interrater reliability and validity of modified elective surgery acuity scale (mESAS) and modified MeNTS scores (Gyn-MeNTS) Benign gynecologic surgeries Modified operation, disease, and patient factors Gyn-MeNTS scoring system did not strongly discriminate the most urgent cases as determined by mESAS. Saleeby et al10 Modified scoring system on gynecologic surgeries General gynecologic, gynecologic oncologic, and female pelvic reconstructive surgery Modified operation, disease, and patient factors The modified-MeNTS could be purposed as a quantitative method for decision-making rather than subjective assessments. Sharma et al8 Modified scoring system on otolaryngology surgeries (MeNTS-M) Otolaryngology-Head and Neck Surgery (adults and pediatrics) Mucosal score was incorporated into the original MeNTS The mucosal score integrated MeNTS-M was interpreted as a valuable tool on triaging otolaryngology-head and neck surgeries. Teja et al25 Modified scoring system on ophthalmic surgery Ophthalmic surgery Modified operation, disease, and patient factors Modified MeNTS could provide guidance to ophthalmologists to facilitate decision making in triaging elective procedures. Coello et al26 Comparison of modified MeNTS and subjective priority scale on operated, and deferred cases Urologic surgery Modified operation, disease, and patient factors Modified MeNTS scores did not show statistically significant difference between operated and non-operated patients. The score was not considered as a useful tool. Fernandez et al27 Modified scoring system on pediatric urology Pediatric urologic surgery Modified operation and patient factors Same disease factors Pediatric urology specific modified scoring system was proposed and allowed to prioritize surgeries with cut-off values of 12 and 16. Prabhakar et al9 Modified scoring system on orthopedic surgery (MeNTS-OS) Orthopedic surgery Modified operation, disease, and patient factors (consists of surgical and disease factors) MeNTS-OS scoring system was proposed as a useful tool to triage orthopedic surgeries. Higher scores were correlate with postponed cases.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.