


Article Figures & Data
Figures
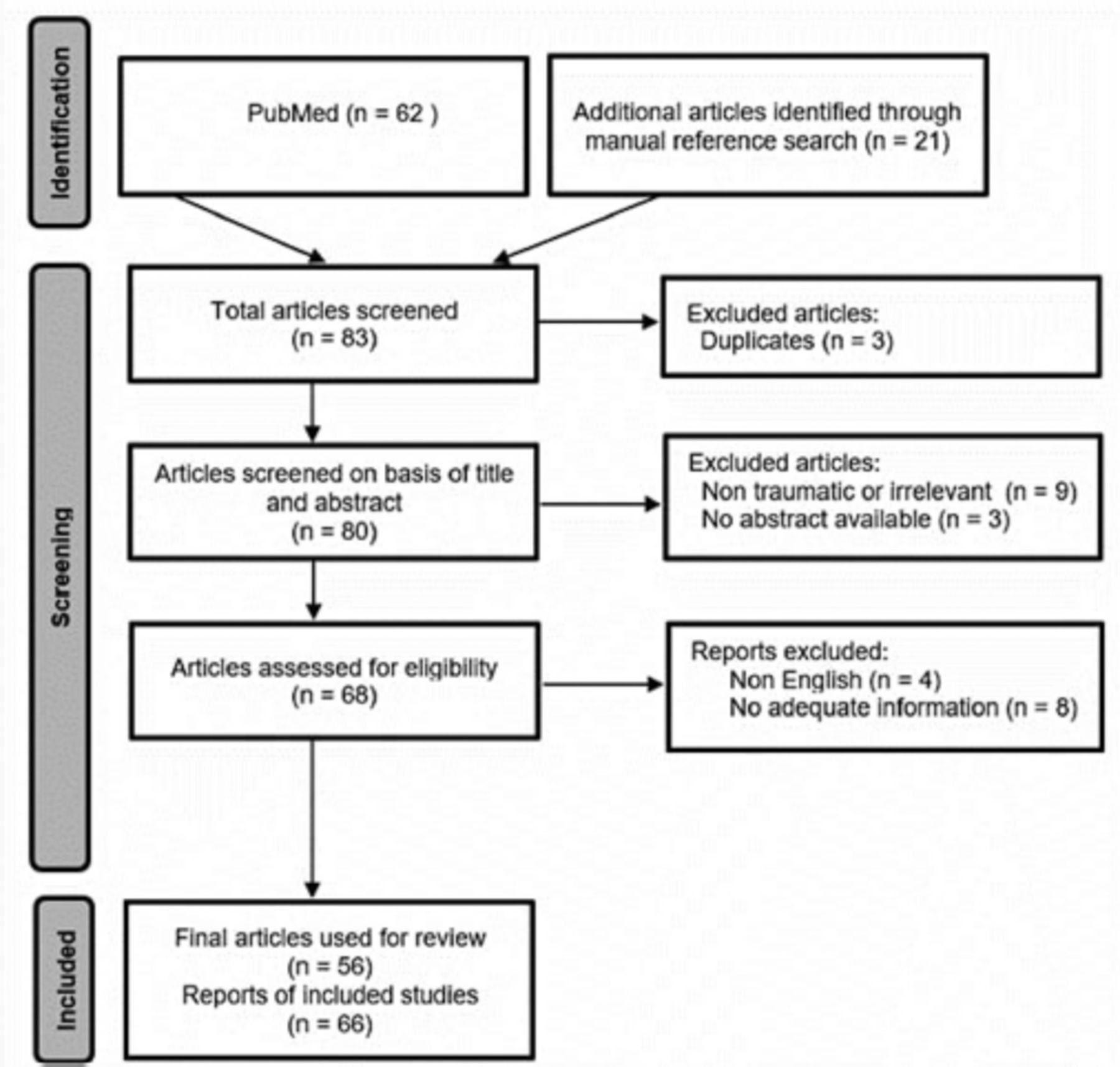
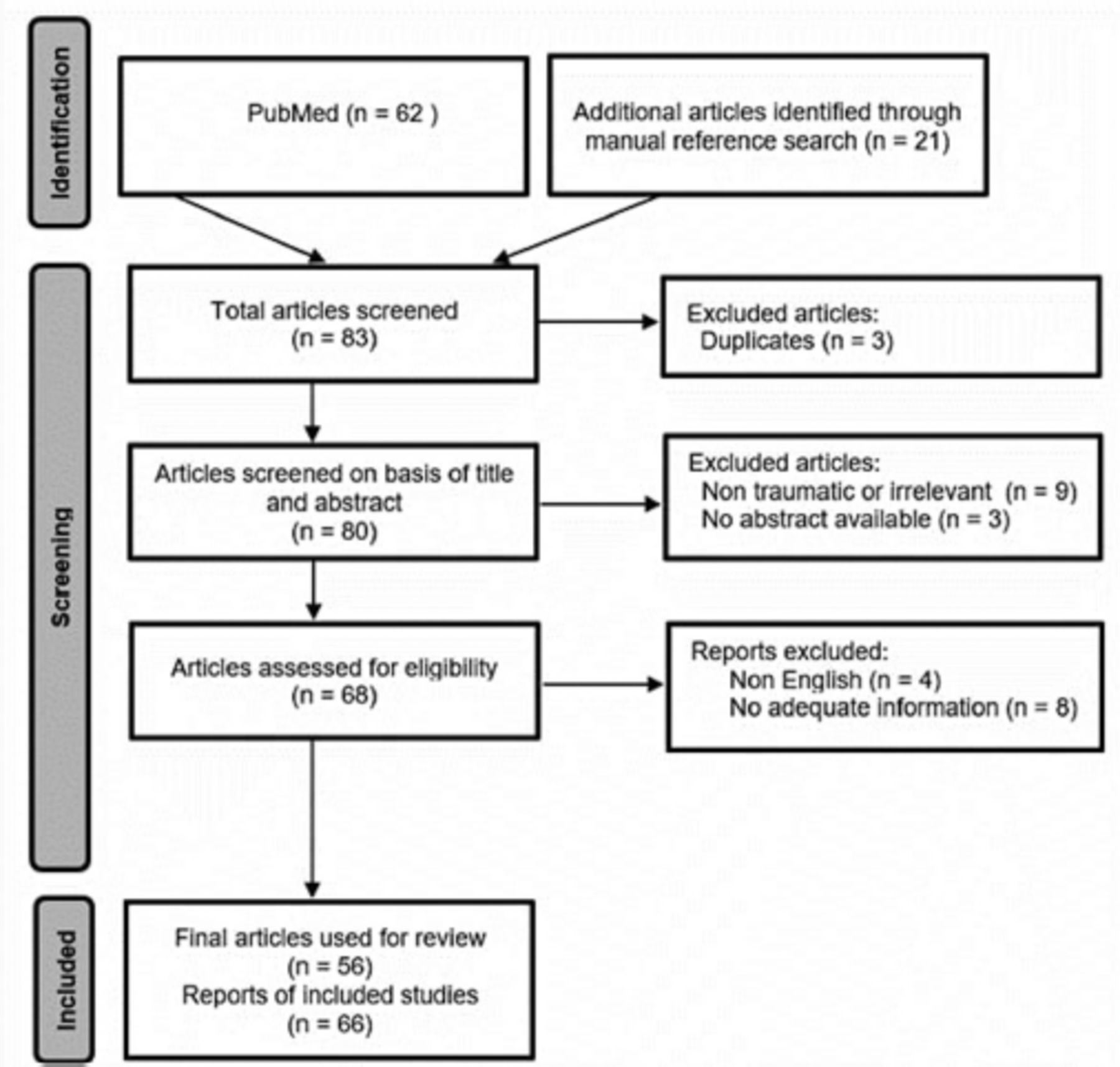
- Figure 1
- The Preferred Reporting Items of Systematic Reviews guidelines flow diagram.
- Figure 2
- Common symptoms for patients with traumatic retropharyngeal hematoma.
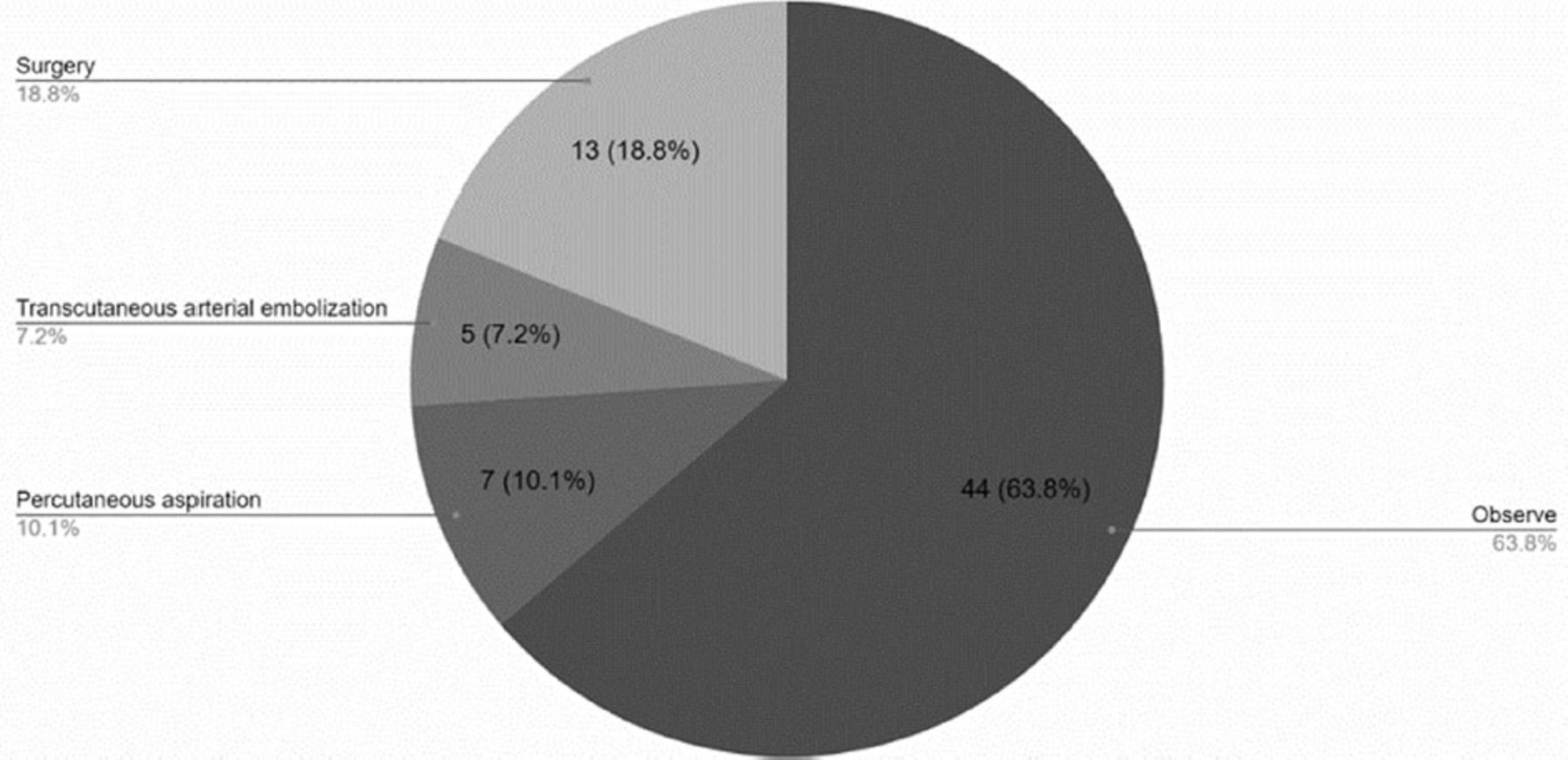
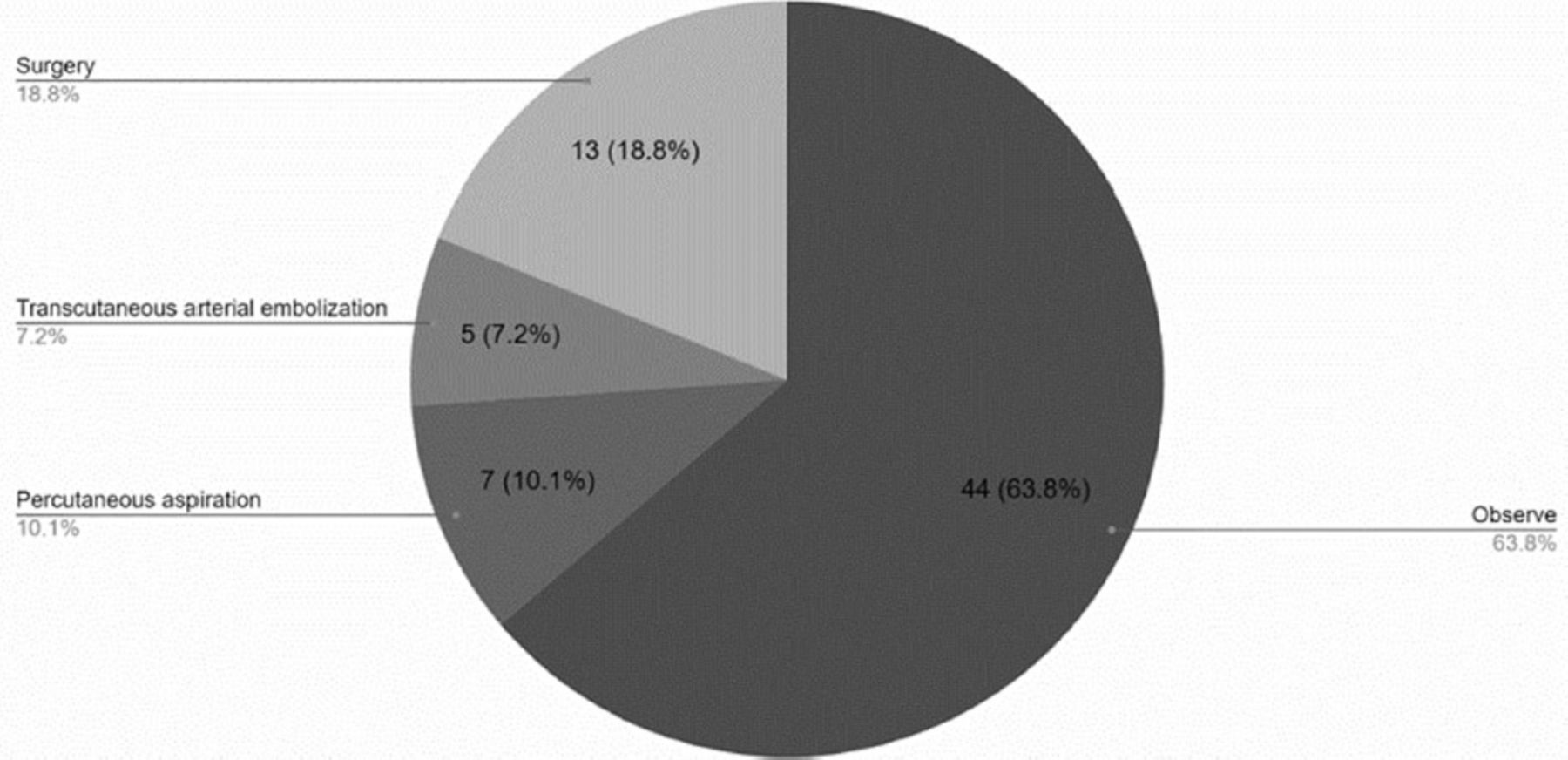
- Figure 3
- Treatment modalities.
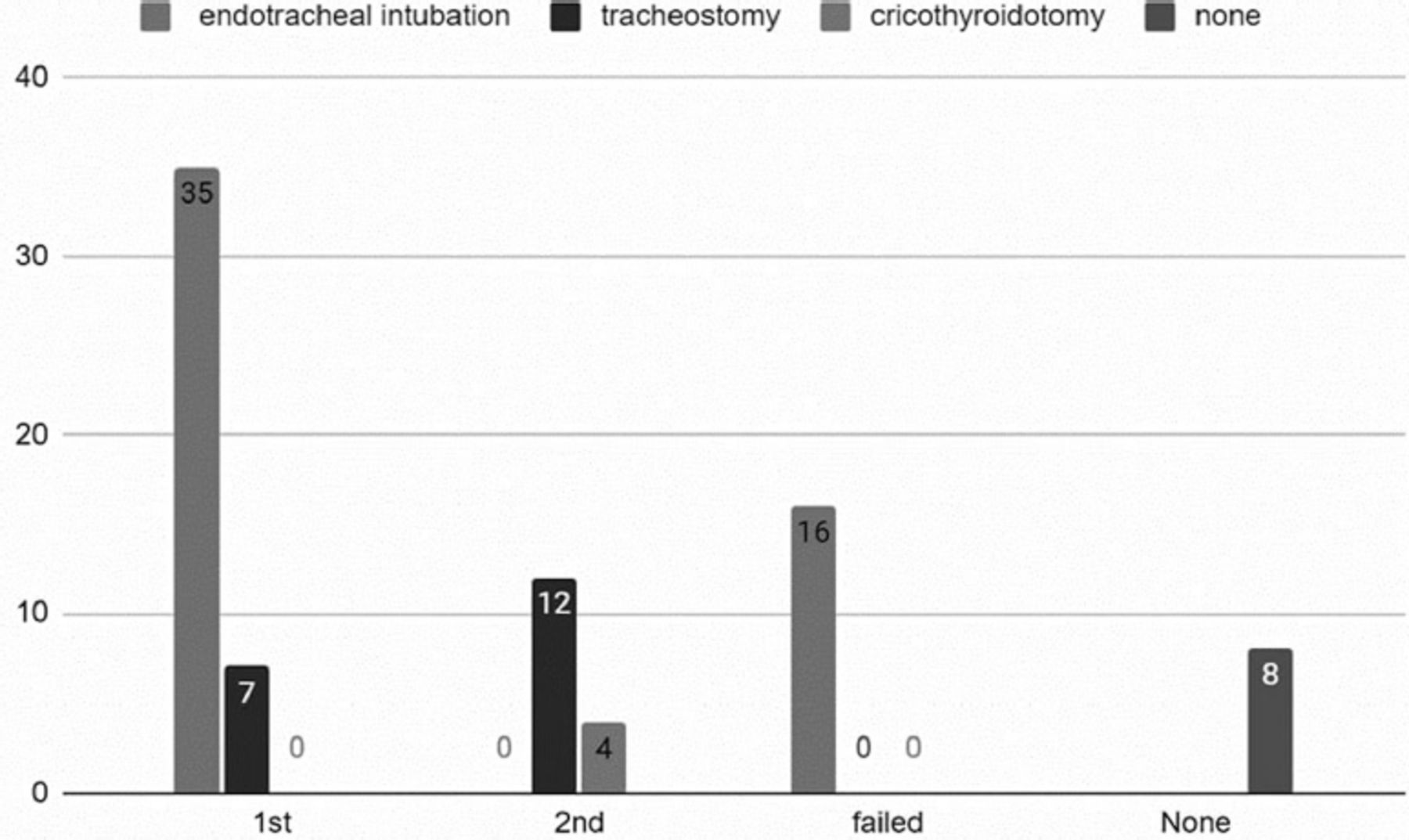
- Figure 4
- Patient’s airway management.

Tables
Case no. Authors Year of publication Ages Genders Anti-coagulation/coagulopathy Mechanism of injury Presenting symptoms Time from injury to symptoms (hours) Associated injuries 1. Smith et al39 1988 77 F No Hx Fall Neck pain, dysphagia, stridor, dyspnea, forehead ecchymosis Unknown 0 2. Myssiorek et al10 1989 80 M No Hx MVA Dysphagia, hoarseness, dyspnea 2 hrs. 0 3. Biby et al40 1990 27 F No Hx MVA AMS, neck pain, trismus, dysphagia Unknown Odontoid fracture, cranial nerve VI palsy 4. Kuhn et al29 1991 22 M No Hx Motorcycle accident Stridor, dyspnea, salivation Unknown Mandibular fracture, C5, 6 fracture subluxation 5. Kuhn et al29 1991 70 M No Hx MVA AMS, cyanosis, dyspnea Unknown Mandibular fracture, C2, 3 fracture subluxation, C7 fracture 6. Kuhn et al29 1991 58 M No Hx Fall Stridor, salivation Unknown C1-3 fractures 7. 1991 82 M No Hx Fall Dyspnea, stridor Unknown Clavicle fracture 8. 1991 22 M No Hx MVA Dyspnea Unknown C6 quadriplegia 9. 1991 75 M No Hx MVA Dyspnea ½ hrs. C4, 5 fractures 10. 1991 92 M No Hx Fall Dyspnea 1 hrs. T4 quadriplegia 11. 1991 83 M No Hx MVA Cardiac arrest 11 hrs. C4,5 fractures and dislocation, quadriplegia 12. Daniello et al41 1994 57 F No Hx Fall Dyspnea, dysphagia, epistaxis Unknown 0 13. Shaw et al42 1995 Unknown (elderly) M No Hx Pedestrian struck by a car Dysphagia, odynophagia, dyspnea, hoarseness, neck swelling Unknown 0 14. Mitchell et al11 1995 28 F No Hx MVA AMS, hoarseness, stridor, neck pain, agitation Unknown 0 15. O’Donnell et al43 1997 19 M No Hx Motorcycle accident Neck swelling, cyanosis, AMS, hematemesis, apnea, pulseless Unknown Atlantooccipital fracture and dislocation 16. Mazzon et al44 1998 81 M No Hx MVA Obtunded, cyanosis, symptoms of upper airway obstruction, neck swelling, AMS Unknown C4, 5 fractures 17. Cox et al45 1998 13 F No Hx Bicycle accident AMS, neck swelling, neck pain, stridor Unknown Skull fracture 18. Senthuran et al13 1999 68 F No Hx Fall Fever, dyspnea, cyanosis, bradycardia Unknown 0 19. Sandooram et al9 2000 78 M Warfarin Fall Dyspnea, dysphonia, dysphagia, tachypneic, stridor, salivation Unknown 0 20. Vakees et al46 2000 88 F No Hx Fall dyspnea, hoarseness, neck swelling 6 hrs. 0 21. Kette et al47 2000 67 M No Hx Fall AMS, neck pain, dyspnea, hoarseness Unknown 0 22. El Kettaniet al48 2002 37 M No Hx MVA Dyspnea, dysphagia, neck pain, stridor 10 hrs. Clavicle fracture, C6 fracture 23. Van Velde et al49 2002 84 F No Hx Fall Dyspnea, stridor, sore throat, neck swelling 5 hrs. 0 24. Shiratori et al50 2003 40 M No Hx Skiing accident neck pain, dyspnea Immediately Tracheal displacement 25. Kochilas et al51 2004 53 M No Hx Fall stridor, dysphonia, neck swelling, dysphagia 4 hrs. 0 26. Suzuki et al33 2004 67 M No Hx MVA dyspnea, neck pain, cervical pain, cyanosis, AMS Immediately C5 fracture 27. Anagnostara et al52 2005 58 M No Hx MVA Dyspnea, dysphagia, sore throat, hoarseness, cyanosis Unknown 0 28 Chiti-Batelli et al53 2005 54 F Warfarin Fall Dysphagia, hoarseness, dyspnea 20-21 hrs. 0 29. Duvillard et al54 2005 40 M No Hx of anti Struck by metallic lump Dyspnea, dysphagia Unknown 0 30. 2005 94 M No Hx of anti Fall Dysphagia Unknown 0 31. Freeman et al55 2005 31 M No Hx Motorcycle accident Cervical pain Unknown 0 32. Lin et al32 2006 50 M No Hx Fall Dyspnea, hoarseness, neck swelling Unknown 0 33. Sheah et al56 2006 90 M No Hx Fall Stridor, neck swelling Unknown Tracheal dislocation and compression 34. Wyngaert et al57 2006 27 M No Hx MVA Neck pain, dyspnea, stridor Unknown Occipital condyles fracture, anterior arcus of the atlas fracture 35. Takeuchi et al58 2007 31 M No Hx Motorcycle accident Neck pain, dyspnea, hoarseness Unknown Atlantooccipital dislocation, cervical subdural hematoma, traumatic subarachnoid hemorrhage, mandibular fracture. 36. Lazott et al59 2007 50 M No Hx Fall Neck pain, dyspnea, hoarseness Unknown Brachial plexus injury, C1 fracture 37. Srivastava et al60 2008 85 F Warfarin Fall Stridor Unknown 0 38. Tsai et al30 2008 40 M No Hx Fall Dyspnea, dysphonia, throat pain, neck pain Unknown 0 39. Birkholz et al61 2010 77 M No Hx MVA Dyspnea and hypoxic cardiac arrest. Unknown Leg fracture, C2 fracture, partial tetraparesis, larynx dislocation 40. Morita et al62 2010 92 M No Hx Fall Sore throat, dyspnea and neck pain 6 hrs. Ligament injury, minor vascular injury around the injured ligament 41. Wronka et al63 2011 89 M No Hx Fall Dysphagia, dysarthria, dyspnea, stridor, hoarseness 168 hrs. C2 fracture and displacement 42. Pfeiffer et al64 2011 92 F No Hx Fall Dyspnea, dysphagia, odynophagia 10 hrs. All cervical spine injury 43. Lin et al65 2011 84 F Warfarin Fall Capp’s triad, dyspnea, neck swelling Unknown Tracheal dislocation and compression 44. Ottaviani et al66 2011 77 F Heparin Iatrogenic Hoarseness, sore throat, dysphagia 48 hrs. 0 45. Senel et al38 2012 86 F No Hx Fall Dyspnea, cyanosis, neck swelling Unknown 0 46. Jakanani et al67 2012 65 F No Hx Fall Dyspnea, cardiac arrest Unknown C5 fracture, prevertebral hematoma 47. Nurata et al68 2012 4 M No Hx Somersault Neck stiffness, neck pain Unknown 0 48. Iizuka et al69 2012 30 F No Hx MVA Dyspnea, neck swelling, AMS Unknown C4-7 fracture, Intracranial hemorrhage 49. Paul et al70 2015 75 M No Hx Fall Neck pain, dysphagia, dyspnea, AMS, stridor, hoarseness, and cyanosis. Unknown 0 50. Thamamongood et al71 2015 77 F No Hx Fall Neck swelling, odynophagia Unknown 0 51. Park et al72 2015 51 M No Hx Fall Neck pain, dyspnea. Unknown 0 52. 2015 78 M No Hx Fall Neck swelling, dyspnea 4 hrs. 0 53. Calogero et al73 2015 80 M No Hx Fall Dysphagia, hoarseness, neck swelling, Unknown 0 54. Kudo et al74 2017 83 F No Hx MVA AMS, dyspnea, hemorrhagic shock, neck swelling Unknown Subarachnoid hemorrhage, C4, 5 dislocations 55. Lowe et al75 2017 60 F No Hx Fall hoarseness, dysphagia, neck pain, neck swelling Unknown Upper aerodigestive tract distortion, loss of normal cervical lordosis 56. Betten et al76 2018 81 F No Hx Fall Stridor, Dyspnea, AMS 10 hrs. 0 57. Ren et al77 2019 55 M No Hx Iatrogenic Cervical swelling, dysphagia 33 hrs. 0 58. Devarakonda et al78 2019 22 M No Hx of anti Fall ------ Unknown Fracture angle (left) Parasymphysis (right) of mandible +trauma in the oropharynx. 59. Chang et al79 2019 93 M No Hx Fall Neck swelling Unknown Incomplete quadriplegia 60. 2019 53 M No Hx MVA Neck pain Unknown 0 61. Arai et al80 2020 75 M No Hx Fall Dyspnea, AMS Unknown Cervical cord injury 62. Yu et al81 2020 55 M No Hx Bicycle accident Dyspnea, neck swelling Unknown 0 63. Iida et al82 2020 79 M Warfarin Fall Neck pain, back pain, dyspnea 4 hrs. Cervical spine at the C3 level, as well as a fracture in the spinous process of the cervical spine. 64. Baek et al83 2020 49 M No Hx MVA Dyspnea, neck swelling Unknown 0 65. Kitai et al84 2021 75 M No Hx Fall Dysphagia, neck swelling 6 hrs. Left scapula fracture, left fifth metacarpal fracture 66. Patel et al85 2021 83 M No Hx Blunt force trauma by the closing doors Neck pain, dysphagia, stridor 1-1.5 hrs. 0 M: male, F: female, Hx: history, C: cervical spine, MVA: motor vehicle accidents, AMS: altered mental status.
Authors Modality Findings Smith et al27 CT Large homogeneous mass gradually occluding the airway at the level of hypopharynx. Biby et al29 CT A severe prevertebral soft tissue swelling. Kuhn et al31 CT I) 4 weeks later, soft tissue swelling occluding airway.
II) Cervical spine revealed a C5 and C6 pedice fracture with subluxation and mild widening of the prevertebral soft tissue. Three days later, retropharyngeal soft-tissue swelling and prominent degenerative osteophytes anteriorly theat contribute to airway obstruction.
III) Breakage from C1’s transverse process to C2’s lamina, a dens fracture, and a fracture of the transverse process of C3, with moderate prevertebral soft-tissue swelling.
IV) Not stated.
V) Not stated.
VI) Complete fracture dislocation of C4 on C5 and extensive prevertebral soft-tissue swelling.
VII) Significant degenerative alterations in the cervical spine and a 4-mm posterior displacement of C5 on C6.
VIII) Widespread soft-tissue edema before vertebrae.Daniello et al33 CT There is a large mass located in the retropharyngeal area that extends from the base of the skull to the top of the lungs. Shaw et al34 CT The imaging showed a fluid-filled cavity in the retropharyngeal space that extended from the second to the sixth cervical vertebrae. The cavity was also found to be enhancing. Mitchell et al35 CT Retropharyngeal hematoma with the trachea outlined only by the endotracheal tube. Mazzon et al37 CT The imaging revealed a large hematoma that extended from the second cervical vertebra to the upper mediastinum. The hematoma occupied the entire pharyngeal and parapharyngeal space, and it caused compression of the upper larynx. Cox et al38 CT The imaging showed that there was an occipital skull fracture that was not displaced, significant swelling of the soft tissue in front of the vertebrae, and compression of the airway from outside. Senthuran et al39 CT The imaging revealed a significant mass in the retropharyngeal region on the left side, measuring 4 × 5 cm. The mass extended from the level of the hyoid bone to the left atrium, and it caused an indentation and anterior displacement of the trachea. Additionally, it blocks the left lower lobe bronchus. Vakees et al41 CT The imaging showed a significant swelling of the soft tissue behind the trachea, which was consistent with a large hematoma that extended from the retropharyngeal and tracheal regions into the posterior mediastinum and base of the skull. Kette et al42 CT/MRI CT: neck edema and hemorrhagic infarction of the peripharyngeal and perilaryngeal tissue, deformed upper airway, perivertebral muscular structures were no more recognizable, and vascular nervous fascia included within the mass without compressed, a discrete amount of air war documented at the level of perithyroidal. MRI: cervical spine contusion at c3-c4 and c5-c6 levels in pre-existing vertebral spondylotic stenosis, the vertebral channel was stenotic, hemorrhagic infarction attributed to hematoma was documented at the same level prevertebral space. Kettani et al43 CT According to the imaging, there was a hematoma that stretched from the fourth cervical vertebra to the upper mediastinum and filled the pharyngeal space, and the sixth cervical vertebra had a fracture. Velde et al44 CT From the base of the skull to the superior mediastinum and the carina, there is a hematoma in the retropharyngeal area. Goiter is indicated by calcifications and nodules on the thyroid gland. Shiratori et al45 CT The trachea is severely narrowed due to a large hematoma that extends from the pharynx to the point where the trachea splits into 2 branches. The narrowing is most severe at the level of the sternoclavicular joint, and the trachea has been pushed forward from its normal position. Kochilas et al46 CT After 12 hours with intravenous contrast, it was suggested that the swelling was caused by a hematoma rather than soft tissue edema. Suzuki et al47 CT The CT scan of the neck with 5 mm slices revealed that the retropharyngeal space is widened, and there is an obstruction in the upper airway. Anagnostara et al48 CT/MRI CT: revealed a retropharyngeal collection that was hypoattenuating and located in the midline, anterior to the swollen prevertebral musculature. It extended from C1-C6 level. Additionally, there was an anterior displacement and compression of the parapharyngeal space, as well as lateral displacement of the carotid space, which were demonstrated bilaterally.The arytenoid cartilages were likewise somewhat shifted anteriorly, more caudally MRI: following the absorption of the prevertebral edema, axial T1 and T2 weighted MRI scans at the level of the tongue base show that the airway has been cleansed. Retropharyngeal collection, which is T2 hyperintense and T1 hypointense, is barely discernible. Chiti-Batelli et al49 CT A mass was identified in the mediastinum that is consistent with a hematoma extending to the carina. Duvillard et al50 CT I) A retropharyngeal hematoma that is massive and extends from the second to the seventh cervical vertebra is present.
II) A retropharyngeal hematoma is present between C3 and C7, which is causing a mass effect on the larynx, trachea, and pharynx without any vertebral fracture.Freeman et al51 CT Imaging of the head was unremarkable. However, type I bilateral occipital condylar fractures with little displacement were found from C0-C2. Lin et al52 CT Demonstrate the presence of a retropharyngeal hematoma that is obstructing the airway and causing breathing difficulties. Sheah et al53 CT A massive low-density retropharyngeal hematoma that stretched from the base of the skull to the mediastinum was visible on the CT image. The suspicion was of extravagance. Wyngaert et al54 CT/MRI The CT scan showed a fracture of the anterior arcus of the atlas and a bilateral fracture of the occipital condyles. Both bone fragments were displaced inferomedially towards the medulla. A type III OCF, according to the classification of Anderson and Montesano, was also detected. MRI: the cervical epidural hematoma with obliteration of the anterior perimedullary space (curtain-sign) was discovered on the MRI, which also verified the OCFs. On the other hand, medullary pathology was not evident. Lazott et al56 CT/MRI The CT scan showed bilateral fractures of the anterior arch of C1 and a fracture of the right C4 spinous process. Mild prominence of prevertebral soft tissues was noted without significant encroachment on the pharynx. MRI: an expanding hematoma was the cause of the noticeable increase in the prevertebral soft tissue prominence seen on the sagittal T2-weighted MRI with fat saturation techniques. Srivastava et al57 CT The CT scan revealed a fracture of the right C4 spinous process in addition to bilateral fractures of the C1 anterior arch. There was a slight prevertebral soft tissue prominence without a noticeable pharyngeal encroachment. Tsai et al58 CT There was a massive hematoma visible on the CT scan that stretched from the base of the skull to the thoracic inlet. Both of the carotid arteries had extravasated contrast material inside of them as well as lateral displacement. Birkholz et al59 CT Fracture of C2, extended retropharyngeal and mediastinal hematoma. The pharynx, the larynx, and the trachea were obstructed by the hematoma, suggestive for partial bilateral basal ganglia infarction. Morita et al60 CT/MRI CT: a large hematoma that stretched from the superior mediastinal space to the retropharyngeal was visible on the CT scan. MRI: at the C4-5 levels, a sagittal MRI (T2-weighted) showed anterior longitudinal ligament tearing. Wronka et al61 CT The CT scan showed a type 2 fracture through the junction of the odontoid peg and body of C2. The body of C2 was displaced anteriorly by approximately 11 mm. There was an associated surrounding hematoma and soft tissue edema. Pfeiffer et al62 CT confirmed that a large retropharyngeal haematoma narrowed the pharyngeal lumen. Lin et al63 CT A large retropharyngeal hematoma that extended between the C2 and T4 vertebral body levels was visible on the CT scan. The trachea was compressed and moved as a result of the hematoma. Ottaviani et al64 CT The CT scan showed a retropharyngeal hematoma measuring 7 cm by 3 cm on the right side. The hematoma caused a mass effect on the pharynx and larynx. Additionally, severe cervical spondylosis was present. Senel et al65 CT A hypodense 3 x 1.5 cm region at the level of C2 and the left anterior border of the trachea was visible on the CT scan. There was a cannula inside the trachea, which was twisted to the right. Jakanani et al66 CT The CT scan revealed a small retrolisthesis of C5 on C6, as well as a reduction in the C5/C6 disc interspace. A C5 lamina fracture that was consistent with a hyperextension injury was also discovered by CT scanning. Nurata et al67 CT/MRI CT: the prevertebral spaces were wider, and the CT scan revealed an X-mm soft tissue mass compressing the trachea between C1 and C4. MRI: on T2-weighted sagittal and axial MRI images, diffuse edema completely obscured the left retropharyngeal space. A retropharyngeal hematoma is consistent with the significant pharyngeal airway narrowing that resulted from this. Iizuka et al68 CT/MRI The CT scan showed a brain contusion in the right frontal lobe, C4-7 right transverse process fracture, no visualization of the right vertebral artery, and extravasation of the contrast agent around the right transverse process fracture. The MRI revealed a massive retropharyngeal hematoma located anteriorly, extending from the C1-T3 vertebrae. This was responsible for the sudden asphyxia. The same MRI also detected avulsion of the right lower cervical roots. Paul et al69 CT Evidence of large retropharyngeal hematoma, measuring approximately 11 cm by 2.4 cm by 4 cm in size and causing severe compression of the adjacent airway Thamamongood et al70 CT A soft tissue mass in the posterior mediastinum, retropharyngeal space, and bilateral carotid space was visible on the CT scan. It appeared isodense to hypodense. The mass compressed the upper esophagus posteriorly and extended caudally to the level of the eighth thoracic vertebra. Park et al71 CT/MRI I) The CT scan showed no definite fracture or vessel injury. However, in the second CT, it revealed a prevertebral hematoma and a dark air density region at the C6-7 disc. There was no fracture or vascular injury on CT angiography. MRI: the same patient’s T2-weighted sagittal MRI revealed a longitudinal mass in the retropharyngeal space from the C3 to T2 levels with heterogeneous signal intensity. The signal intensity was high for the C4 and C5 bodies. The same patient’s T1-weighted sagittal MRI revealed a low signal intensity mass in the retropharyngeal space. While the signal intensity at the upper C4 body was low, it was slightly higher at the lower C4 and C5 bodies. II) Not possible due to poor compliance. Calogero et al72 CT A sizable hematoma, measuring 6.7 cm transversely and 3.2 cm anteroposteriorly, is located in the retropharyngeal space. The hematoma is believed to have originated from the thyrocervical trunk and is situated posterior to the thyroid gland level. It measures 25 centimeters in length and begins at the level of the lower nasopharynx. It continues down the neck into the retropharyngeal space and into the mediastinum posterior to the esophagus. The hematoma causes esophageal compression in addition to anterior deviation of the larynx. Prevertebral soft tissue swelling is seen in the cervical spine, which causes the endotracheal tube to move anteriorly. Unintentionally, the abdomen revealed a 4.8 cm abdominal aortic aneurysm. Kudo et al73 CT/MRI A retropharyngeal hematoma and C4/C5 dislocation were visible on the CT scan. Bilateral occipital watershed infarctions were seen on the MRI; they did not seem to be causing any symptoms. Lowe et al74 CT Retropharyngeal hematoma Betten et al75 CT The CT scan was normal, but a large retropharyngeal hematoma measuring 3.6 cm by 5.3 cm by 20 cm was detected. Ren et al76 MRI A significant C4/5 and C5/6 disc herniation with severe spinal cord compression is visible on the sagittal cervical spine MRI. On T2-weighted images, there is an abnormally hyperintense signal in the spinal cord at the C5/6 level. A massive retropharyngeal hematoma that extends from the base of the skull to T1 is visible on the sagittal T2-weighted MRI 35 hours after surgery. This hematoma severely compresses the laryngopharynx and oropharynx posteriorly. A massive incisional hematoma between the trachea and carotid sheath is visible on the axial T2-weighted MRI. Chang et al78 CT/MRI CT: I) a type II dens fracture (Anderson-D’Alonzo classification) and the Wackenheim line running behind the dens, indicating posterior AOD, were both visible on the CT scan. II) The CT scan additionally revealed a posterior AOD-indicating type II dens fracture with comminution (Anderson-D’Alonzo classification) and a running of the Wackenheim line behind the dens. A combined horizontal and sagittal split fracture of the C1 anterior arch and a type II dens fracture with comminution were identified on the coronal and axial reconstructed CT scans. Furthermore, a type II TAL injury was suggested by an avulsion fragment from the lateral mass of C1 and a widened right atlantodental interval seen on an axial CT scan. MRI: increased anterior soft tissue swelling as a result of intramedullary hemorrhage and retropharyngeal hematoma was seen on the MRI. The axial MRI showed a type II TAL injury in accordance with Dickman’s classification and a midline sagittal split fracture of the C1 anterior arch. Arai et al79 CT Massive retropharyngeal hematoma Yu et al80 CT In the retropharyngeal space, a sizable hematoma that stretched from the base of the skull to the posterior mediastinum was discovered. Additionally, there was evidence of contrast leakage at the C6-7 vertebral level. Iida et al81 CT There is a sizable hematoma measuring 53 × 145 × 25 mm in the retropharyngeal space. The patient also has a cervical spine spinous process fracture and a cervical fracture (C3). At the C7 vertebral body level, contrast agent extravasation was observed in the hematoma, which is compressing the hypopharynx and larynx. Baek et al82 CT/MRI CT: no definite fracture or vessel injury was detected. However, an intense retropharyngeal hematoma was found. MRI: a heterogeneous signal intensity mass in the retropharyngeal space is visible on the T2-weighted sagittal MRI. A mass with low signal intensity is visible in the retropharyngeal space on the T1-weighted sagittal MRI. Kitai et al83 CT There was no evidence of a retropharyngeal space anomaly or spinal fracture. Nonetheless, fractures on the left fifth metacarpal and scapula were discovered. Patel et al84 CT The nasopharynx and supraglottic larynx are effaced anteriorly due to opacification of the entire retropharyngeal (danger) tissue space (mean 65 HU), which stretches from the base of the skull to the mediastinum. This is caused by a noticeable mass effect. RPH: retropharyngeal hematoma, CT: computed tomography, MRI: magnetic resonance imaging, OCF: occipital condylar fracture, AOD: atlantooccipital dislocation, TAL: transverse atlantal ligament, HU: hounsfield units
Case No. Author Year of publication Method of airway management Treatment modalities Acute complications Cause of mortality ICU 1 Smith et al39 1988 Tracheostomy Observe None No No 2 Myssiorek et al10 1989 Endotracheal intubation Percutaneous aspiration None No No 3 Biby et al40 1990 Endotracheal intubation Observe None No No 4 Kuhn et al29 1991 First tried endotracheal intubation, then cricothyroidotomy Observe Anoxic brain damage No No 5 First tried endotracheal intubation, then cricothyroidotomy Observe None No No 6 Endotracheal intubation Observe None No No 7 Tracheostomy Observe Difficulty swallowing solid foods for months No No 8 First tried endotracheal intubation, then cricothyroidotomy Observe Respiratory arrest No No 9 Tracheostomy Observe Fatal pneumonia and multiple organ failure No No 10 Endotracheal intubation Observe Respiratory arrest No No 11 First tried endotracheal intubation, then tracheostomy Observe Cardiopulmonary arrest No No 12 Daniello et al41 1994 First tried endotracheal intubation, then cricothyroidotomy Observe Non No No 13 Shaw et al42 1995 Tracheostomy Observe None No No 14 Mitchell et al11 1995 Endotracheal intubation Percutaneous aspiration None No No 15 O’Donnell et al43 1997 First tried endotracheal intubation, then tracheostomy Observe None Multisystem organ failure Yes 16 Mazzon et al44 1998 First tried endotracheal intubation, then tracheostomy Observe None No Yes 17 Cox et al45 1998 Endotracheal intubation Observe None No Yes 18 Senthuran et al13 1999 First tried endotracheal intubation, then tracheostomy Observe Pneumonia, left arm swelling, subclavian and internal jugular vein thrombus No Yes 19 Sandooram et al9 2000 First tried endotracheal intubation, then tracheostomy Observe None No No 20 Vakees et al46 2000 Endotracheal intubation Percutaneous aspiration None No No 21 Kette et al47 2000 Not mentioned Observe None No Yes 22 El Kettani et al48 2002 Not mentioned Observe None No Yes 23 Van Velde et al49 2002 Endotracheal intubation Observe None No No 24 Shiratori et al50 2003 Endotracheal intubation Observe None No No 25 Kochilas et al51 2004 Endotracheal intubation Transcutaneous arterial embolization None No Yes 26 Suzuki et al33 2004 First tried endotracheal intubation, then tracheostomy Observe None Hemodynamically unstable Yes 27 Anagnostara et al52 2005 Endotracheal intubation Observe None No No 28 Chiti-Batelli et al53 2005 Endotracheal intubation Observe None No No 29 Duvillard et al54 2005 Tracheostomy Observe None No No 30 2005 Endotracheal intubation Percutaneous aspiration None No No 31 Freeman et al55 2005 Tracheostomy Percutaneous aspiration None No No 32 Lin et al32 2006 Not mentioned Observe None No Yes 33 Sheah et al56 2006 Endotracheal intubation Observe None No No 34 Wyngaert et al57 2006 First tried endotracheal intubation, then tracheostomy Observe None No No 35 Takeuchi et al58 2007 Endotracheal intubation Transcutaneous arterial embolization None No No 36 Lazott et al59 2007 Not mentioned Observe None No Yes 37 Srivastava et al60 2008 Endotracheal intubation Surgery Pulmonary oedema, type 2 respiratory failure No Yes 38 Tsai et al30 2008 Endotracheal intubation Surgery None No No 39 Birkholz et al61 2010 Endotracheal intubation Observe None No No 40 Morita et al62 2010 Tracheostomy Observe None No No 41 Wronka et al63 2011 First tried endotracheal intubation, then tracheostomy Surgery None No No 42 Pfeiffer et al64 2011 Endotracheal intubation Observe None No No 43 Lin et al65 2011 First tried endotracheal intubation, then tracheostomy Observe None No No 44 Ottaviani et al66 2011 Endotracheal intubation Percutaneous aspiration None No No 45 Can Senel et al38 2012 Endotracheal intubation Observe None Multiple organ failure Yes 46 Jakanani et al67 2012 Endotracheal intubation Percutaneous aspiration None No No 47 Nurata et al68 2012 First tried endotracheal intubation, then tracheostomy Observe None No No 48 Iizuka et al69 2012 Endotracheal intubation Transcutaneous arterial embolization None No Yes 49 Paul et al70 2015 Not mentioned Observe None Multiple organ failure Yes 50 Thamamongood et al71 2015 Endotracheal intubation Observe None No Yes 51 Park et al72 2015 Tracheostomy Surgery None No No 52 2015 Not mentioned Observe None No No 53 Calogero et al73 2015 Endotracheal intubation Surgery haemorrhage from the branches of the internal thoracic artery No No 55 Lowe et al75 2017 Endotracheal intubation Transcutaneous arterial embolization None No No 56 Betten et al76 2018 Endotracheal intubation Transcutaneous arterial embolization None Multiple organ failure No 57 Ren et al77 2019 Tracheostomy Surgery None No No 58 Devarakonda et al78 2019 First tried endotracheal intubation, then tracheostomy Surgery Submucosal swelling in the posterior wall of the pharynx, at the naso-oro junction, approximating the outline of the endotracheal tube No Yes 59 Chang et al79 2019 Endotracheal intubation Surgery None No No 60 2019 Not mentioned Surgery None No No 61 Arai et al80 2020 Not mentioned Observe None No No 62 Yu et al81 2020 Endotracheal intubation Observe None No No 63 Iida et al82 2020 Endotracheal intubation Observe None No No 64 Baek et al83 2020 First tried endotracheal intubation, then tracheostomy Surgery None No No 65 Kitai et al84 2021 Endotracheal intubation Observe None No No 66 Patel et al85 2021 Endotracheal intubation Surgery Diffuse mucosal oedema and copious secretions No No 66 2021 Endotracheal intubation Surgery Diffuse mucosal oedema and copious secretions No No
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.