


Abstract
Objectives: To investigate the relationship of the erythrocyte distribution width (RDW)/albumin ratio on hospital length of stay (LOS) and prognosis in patients hospitalized with chronic obstructive pulmonary disease (COPD) exacerbation.
Methods: Patients hospitalized in our clinic for COPD exacerbation were retrospectively analyzed. Demographic characteristics, comorbidities, pulmonary function tests, arterial blood gas, history of hospitalization due to exacerbation in the last year, LOS, C-reactive protein, RDW, albumin, platelet counts, and 30-day mortality status were recorded. Significant cut-off RDW/albumin ratio values that could predict hospitalization for 10 days or more were analyzed.
Results: A total of 58 patients were included in our study. With a significant cut-off value of ≥5.22 for the RDW/albumin ratio to predict a duration of hospitalization of more than 10 days, a sensitivity of 68.42% and specificity of 74.36% were obtained. No significant association was found between the RDW/albumin ratio and 30-day mortality (p=0.14). The RDW/albumin ratio (p=0.005) and mortality (p<0.001) were found to be higher in patients with an LOS of 10 days or more. The RDW/albumin ratio and mortality, which were statistically significant in patients hospitalized for 10 days or more, were analyzed using logistic regression, and no significant results were found.
Conclusion: In further analysis results of patients hospitalized due to COPD exacerbation, there was no significant relationship between length of hospital stay, mortality, and the RDW/albumin ratio.
Chronic obstructive pulmonary disease (COPD) is defined as a widespread, preventable, and treatable inflammatory disease characterized by persistent airflow limitation due to abnormalities in the airways or alveoli, often due to exposure to toxic gases and particles.1 It is the 3rd leading cause of death around the worldwide, especially in low- and middle-income nations.2
Chronic obstructive pulmonary disease exacerbation is defined as an acute worsening of the disease requiring additional treatment for respiratory symptoms and, if hospitalization is required, is described as a severe exacerbation.1 The 5-year mortality rate in a patient with COPD hospitalized for an exacerbation is approximately 50%.3
During COPD exacerbation, airway inflammation and oxidative stress increase. It has been shown that the neutrophil increase in the airways is correlated with a decline in forced expiratory volume in the first second (FEV1) and that this is independent of bacterial infection.4,5 Again, while expiratory airflow limitation and end-expiratory lung volume increase in exacerbation, inspiratory capacity decreases. As a result, inspiratory muscle dysfunction, impaired gas exchange, neuromechanical dissociation, and mucus hypersecretion lead to an escalation in symptoms such as dyspnea, cough, and sputum during exacerbation.6 In exacerbations, systemic inflammation increases in addition to airway inflammation. This leads to atherosclerotic plaque destabilization and increases the risk of acute coronary syndrome and stroke.7 Considering that hospitalization due to exacerbation increases the mortality rate in patients with COPD, there is a need for inexpensive biomarkers that can be used easily to predict the frequency of attacks, hospital length of stay (LOS), and mortality.
Erythrocyte distribution width (RDW) is an inexpensive and easily applicable parameter that reflects the degree of heterogeneity in erythrocyte volume and is used to define anemia but recent studies have shown that high RDW levels are associated with mortality in inflammatory diseases such as cardiovascular disease, community-acquired pneumonia, sepsis, and COPD.8-12
Albumin is a laboratory test that is routinely measured in the blood of hospitalized patients and is vital for modulating oncotic pressure. It also contributes to anti-inflammatory effects, reduces oxidative stress, and inhibits endothelial cell apoptosis.13 Hypoalbuminemia has been associated with increased mortality in COPD.14,15
The RDW/albumin ratio is a combination of RDW and albumin and is considered a new inflammatory risk marker calculated as the ratio of RDW to serum albumin (%/g/dL). In the literature, it has been associated with mortality in patients with diabetic ketoacidosis, heart failure, and acute respiratory distress syndrome.16-18 However, only a study have investigated the association of RDW/albumin ratio with mortality in COPD.19 Qiu et al19 found that a high RDW/albumin ratio was correlated with in-hospital mortality in a study carried out on patients with COPD admitted to the intensive care unit (ICU).
In our study, we pointed to investigate the relationship between the RDW/albumin ratio on mortality, frequency of attacks, and LOS in patients hospitalized for COPD exacerbation.
Methods
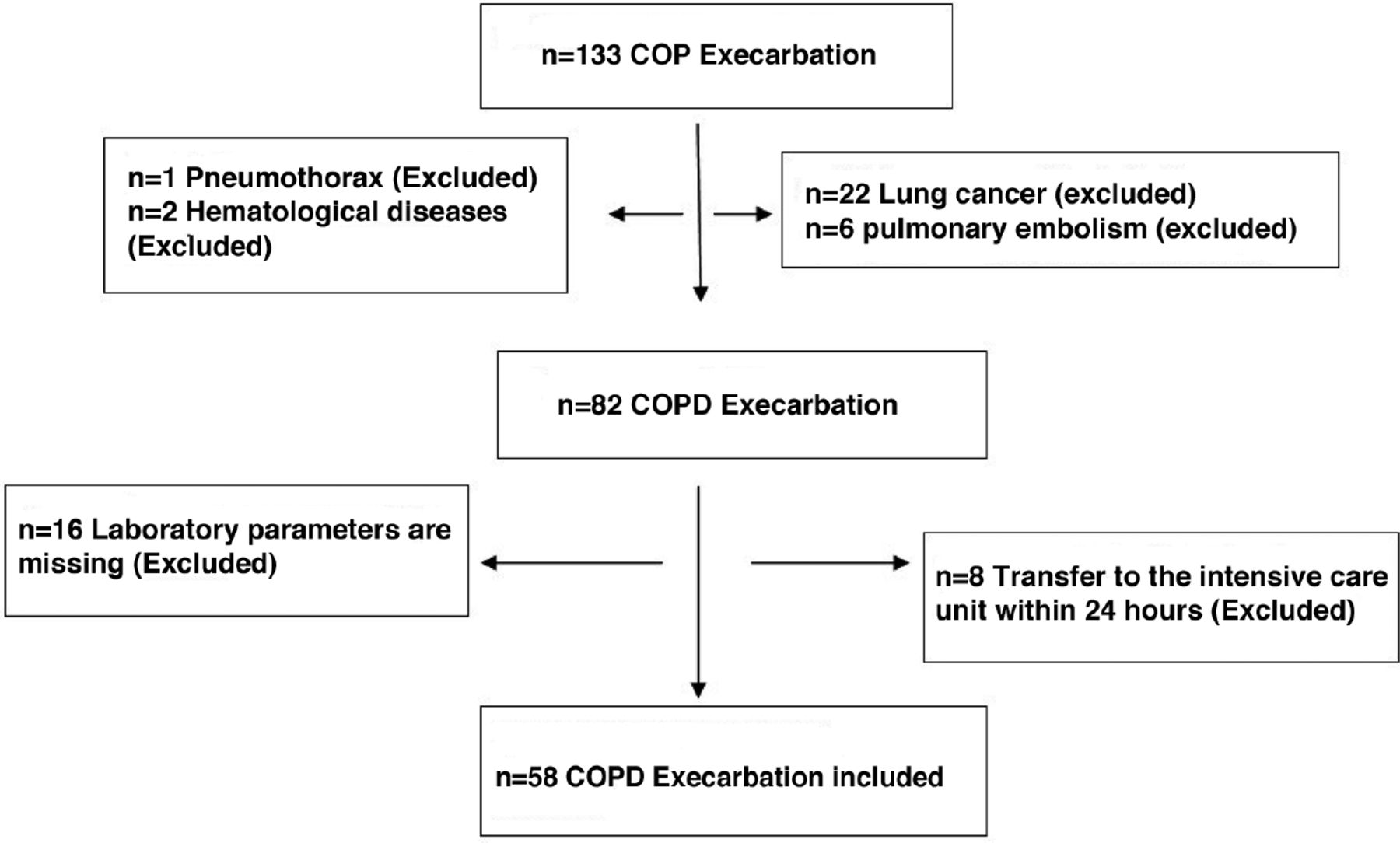
Patients who were admitted to the Chest Diseases Clinic of Dr. Lutfi Kirdar City Hospital, Istanbul, Turkey, between June 2019 and January 2020 with the diagnosis of COPD exacerbation were retrospectively examined. Patients with missing RDW and albumin data, concomitant pulmonary embolism with COPD, lung cancer, pneumothorax, hematologic diseases, those who were transferred to the ICU within 24 hours of being admitted to the hospital, and patients aged under 40 years were excluded from the study (Figure 1).
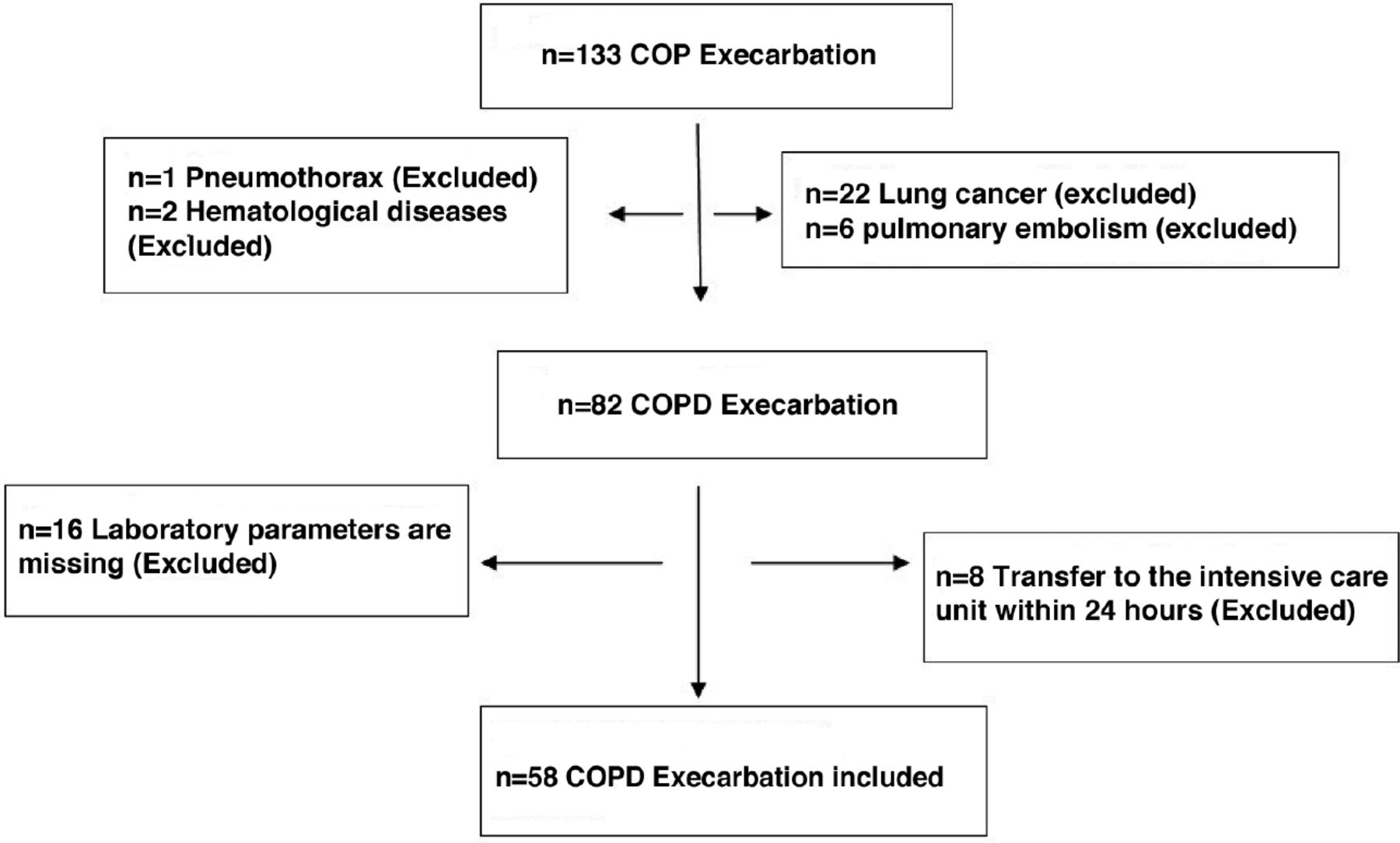
- Patient selection flowchart.
The study protocol was affirmed by the ethics committee of Dr. Lutfi Kirdar City Hospital, Istanbul, Turkey (Decision no.: 2023/514/250/21) and carried out in agreement with the Declaration of Helsinki.
Gender, age, body comorbidity (diabetes, cardiovascular diseases, hypertension, and renal dysfunction), body mass index (BMI), arterial blood gases during hospitalization, serum C-reactive protein (CRP), albumin level, RDW percentage, platelet counts, pulmonary function tests, history of hospitalization for an attack in the last year, LOS, discharge, and death status were recorded.
Significant cut-off values of the RDW/albumin ratio that could predict hospitalization for 10 days or more were analyzed.
The primary outcome of this study was the 30-day mortality, and the secondary outcome was the LOS.
Statistical analysis
Data were analyzed using the Statistical Package for the Social Sciences, version 25.0 software package (IBM, Armonk, NY, USA). The normality of variable distribution was examined using histogram graphs and the Kolmogorov-Smirnov test. Median, mean, standard deviation (SD), interquartile range (IQR), and minimum-maximum values are used to present descriptive analyses. Categorical variables were compared using the Chi-square test. The Mann-Whitney-U test was used to analyze non-normally distributed (nonparametric) variables between 2 groups. Spearman’s correlation test was used to analyze the measured data with each other. Factors affecting a length of stay of 10 days or more were examined using binary logistic regression analysis. Significant cut-off values were investigated using receiver operating curve (ROC) analysis. P-values of <0.05 were considered significant.
Results
The study included 58 patients hospitalized for COPD exacerbation. The mean age of the patients was 71 (48-91) years, and 40 (68.97%) patients were male. In pulmonary function tests, the mean FEV1 values were found as 42% (range: 19-93). The median value for albumin was found as 3.35 (2.4-4.2) g/dL, RDW a median value of 17% (10.4-19%) in RDW, and a median value of 5 (3.15-7.5) in RDW/albumin ratio, at admission (Table 1).
- General characteristics of the patients.
According to the hospitalization LOS, patients were divided into 2 groups: 10 days or more and less than 10 days. When the 2 groups were compared, no significant difference was detected between age, gender, comorbidity, BMI, FEV1, and arterial blood gases (p>0.05).
The RDW/albumin ratio (p=0.005) and mortality (p<0.001) were found to be significantly higher in the group with a hospital LOS of 10 days or more (Table 2).
- Clinical outcomes of patients with chronic obstructive pulmonary disease in the matched cohorts.
The RDW/albumin ratio and mortality, which were statistically significant in patients hospitalized for 10 days or more, were analyzed using logistic regression and no significant results were found (Table 3).
- Logistic regression analysis between mortality and erythrocyte distribution width/albumin.
Regarding 30-day mortality, it was determined that 7 (12.1%) patients died. No relationship was found between RDW/albumin ratio and 30-day mortality (p=0.14).
The RDW/albumin values were higher in the group with a history of hospitalization for COPD exacerbation in the last year compared with the group without hospitalization (p=0.002). The RDW/albumin ratio was found to be higher in patients with one or more comorbidities (p=0.024).
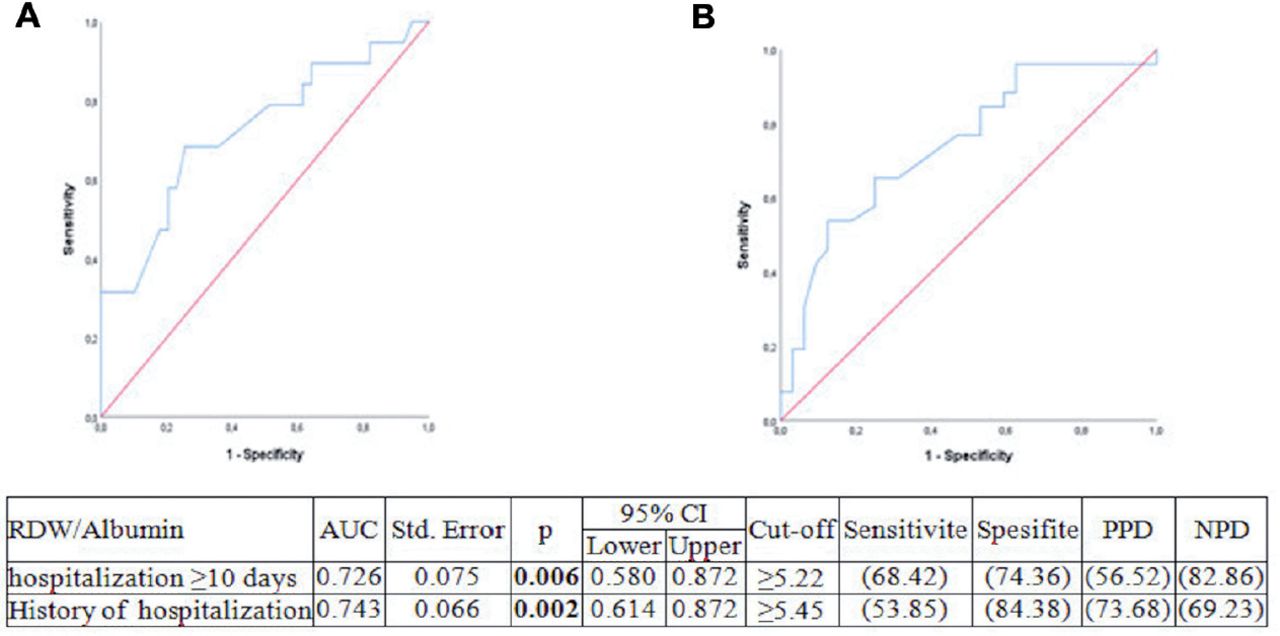
With a significant cut-off value of ≥5.22 for the RDW/albumin ratio to predict an LOS of 10 days or more, 68.42% sensitivity, 74.36% specificity, 56.52% positive predictive value (PPD), and 82.86% negative predictive value (NPD) were obtained (Figure 2a). With a significant cut-off value of ≥5.45 to predict hospitalization for COPD exacerbation in the last year, a sensitivity of 53.85%, specificity of 84.38%, PPD of 73.68%, and NPD of 69.23% were obtained (Figure 2b).
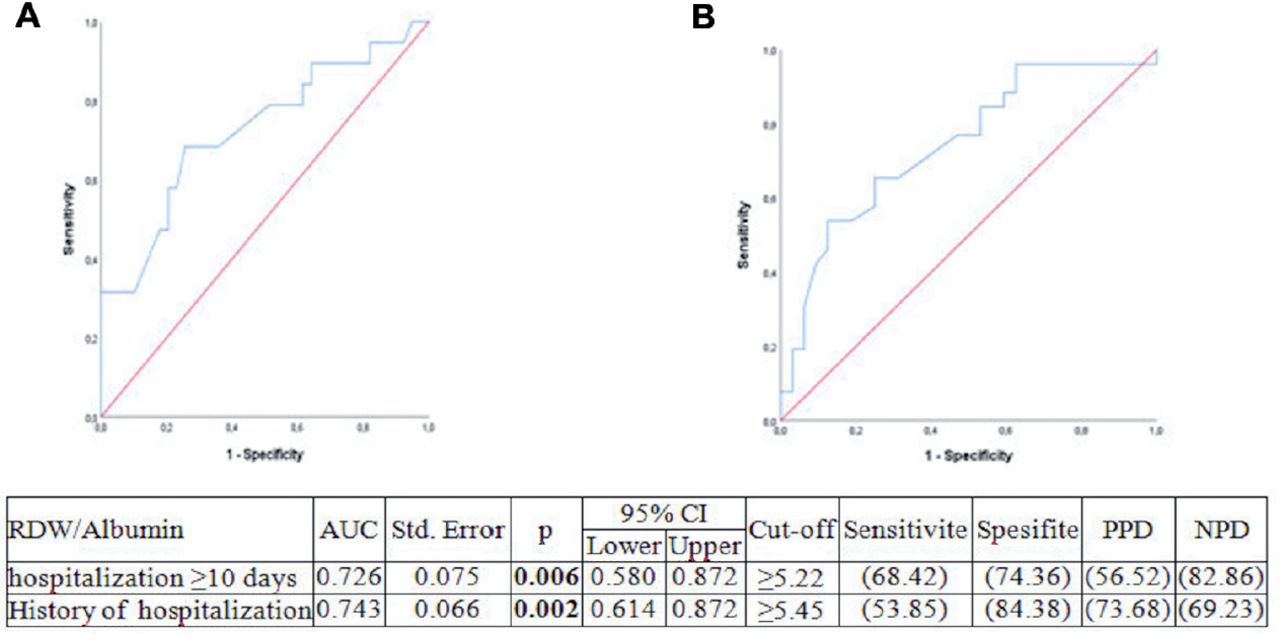
- Ratio of curve analysis. A) RDW/albumin ratio to predict a duration of hospitalization of more than 10 days. B) DRW/albumin to predict hospitalization for chronic obstructive pulmonary exacerbation in the last one year. PPD: positive predictive value, NPD: negative predictive value, RDW: erythrocyte distribution width
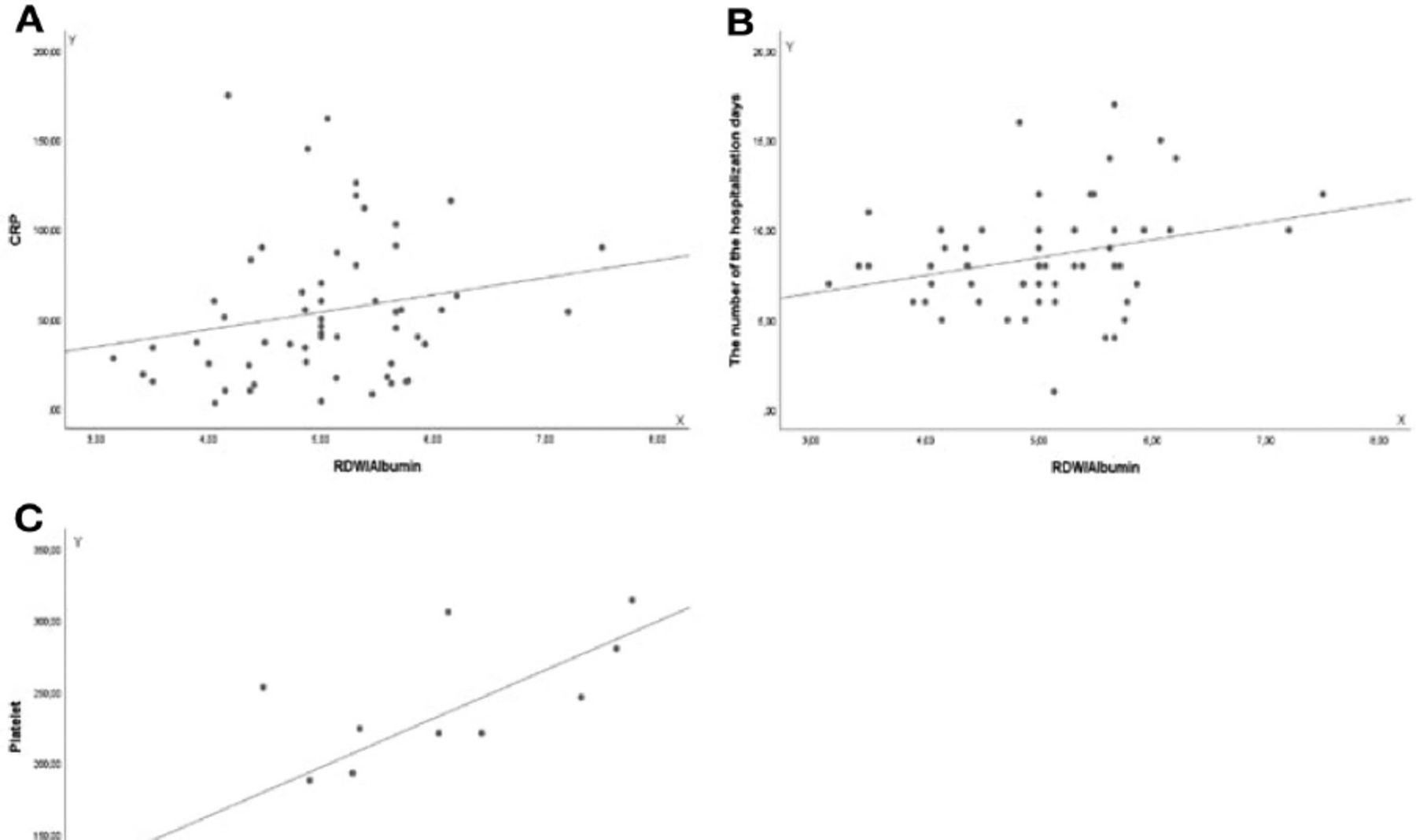
A similar correlation was found between RDW/albumin and CRP (r=0.265, p=0.046), LOS (r=0.266, p=0.043), and platelet count (r=0.732, p=0.004, Figures 3a-c).
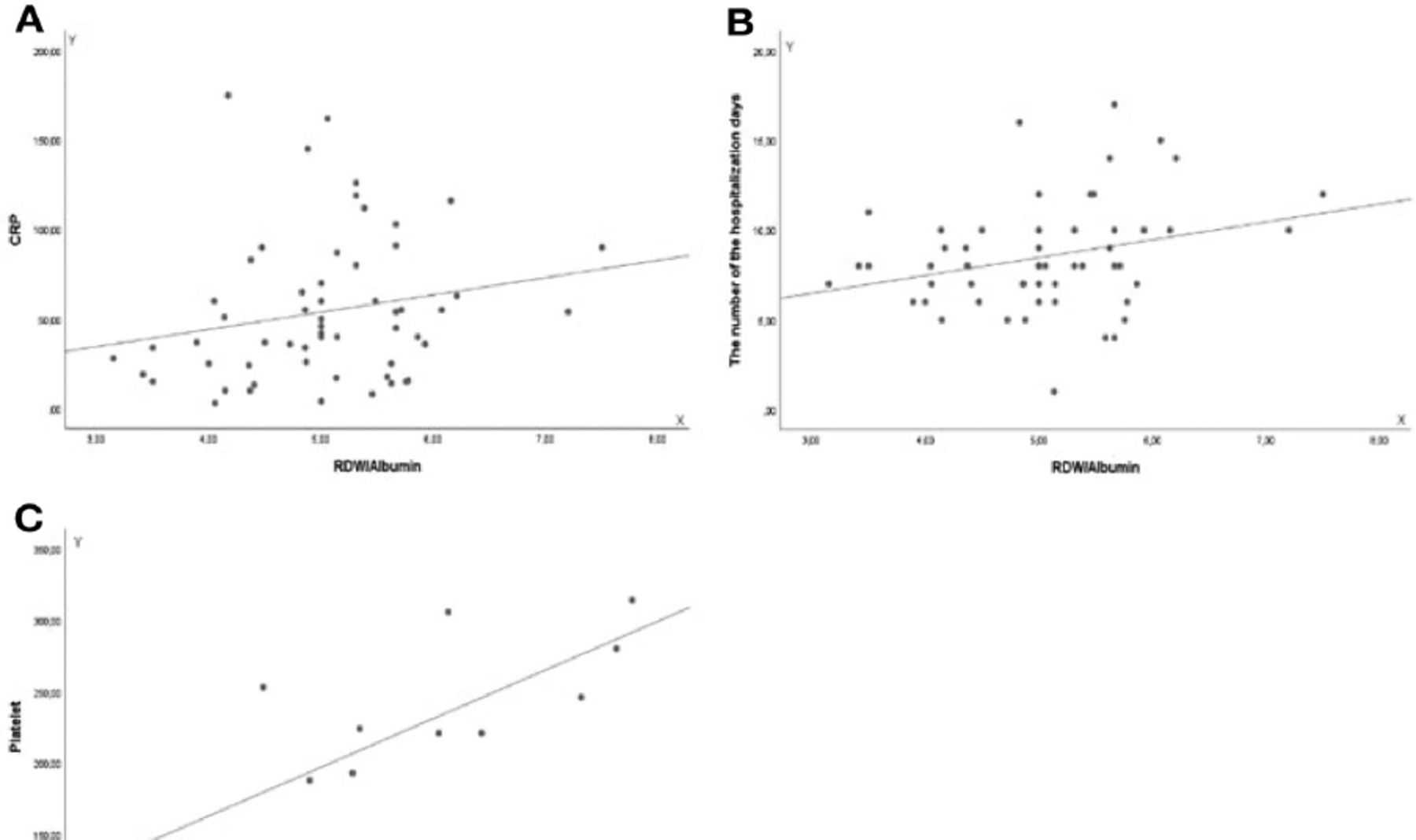
- Spearman correlation test. A) x=RDW/albumin, y=C-reactive protein (CRP). B) x=RDW/albumin, y=the number of hospitalization days (LOS). C) x=RDW/albumin, y=platelet counts. RDW: erythrocyte distribution width.
Discussion
No significant correlation was found between RDW/albumin ratio at admission and 30-day mortality in patients hospitalized for COPD exacerbation in this study. Although RDW/albumin ratio and mortality were found to be higher in patients hospitalized LOS for 10 days or more, no difference was found after further analyses.
The RDW is a routine component of the hemogram, which shows heterogeneity in erythrocyte size and is used as a laboratory value for anemia.20 The RDW is considered to be strongly correlated with inflammatory parameters such as CRP and erythrocyte sedimentation rate and therefore may be used as an inflammatory parameter.21 A similar correlation was found in our study between RDW/albumin and serum CRP (r=0.26, p=0.046) and platelet counts (r=0.73, p=0.004) among inflammation parameters.
Studies have shown that high RDW can be used as an indicator of worse prognosis in COPD.12,22 In a study carried out by Rahimirad et al12 on 330 patients, it was found that high RDW values at admission were associated with in-hospital mortality (p=0.002) in patients hospitalized for COPD exacerbation. The precise mechanism is unclear; however, it is thought that acute hypoxia causes a significant increase in serum erythropoietin levels, thus, being able to induce the formation of enlarged erythrocytes, which in turn causes an increase in RDW.23
Similarly, albumin levels as a marker of inflammation were shown to be associated with poor prognosis in COPD exacerbation. Connors Jr et al24 found that hypoalbuminemia was associated with poor prognosis in a prospective study of 101 patients hospitalized with severe COPD exacerbation. Low albumin levels play a pro-inflammatory role and are associated with increased oxidative stress, platelet activation, and platelet aggregation.25 The RDW/albumin ratio is a new inflammatory marker and elevated RDW and decreased albumin levels may predict severe inflammation. Therefore, the RDW/albumin ratio may reflect inflammation more accurately than either marker.
There is only one study in the literature investigating the association of RDW/albumin ratio with COPD mortality. Qiu et al19 retrospectively analyzed 1174 patients hospitalized in the ICU for COPD and showed that a high RDW/albumin ratio (>5.315%/g/dL) was associated with hospital mortality (p<0.001). By contrast, in our study, the RDW/albumin ratio was examined in patients with COPD hospitalized in the general ward, and the result was found to be unrelated to mortality (p=0.14). This may be primarily due to our small number of patients and the lower mortality expectation of patients in the ward compared with those in the ICU.
In our study, with a significant cut-off value of ≥5.22%/g/dL for the RDW/albumin ratio to predict an LOS of 10 days or more, a sensitivity of 68.42%, a specificity of 74.36%, PPD of 56.52%, and NPD of 82.86% were obtained. Based on these results, we think that the RDW/albumin ratio may predict LOS. The mechanism by which the RDW/albumin ratio predicts LOS may be explained by possible hypoxia and increased inflammation.
Comorbidities are common in patients with COPD and have a significant negative impact on the quality of life, exacerbation frequency, and survival of patients.26 In our study, approximately 63% of patients had at least one comorbidity, and the RDW/albumin ratio was higher in patients with comorbidities than in those without (p=0.024).
Severe exacerbations of COPD have been shown to be associated with poor prognosis. The mortality rate increases as the frequency of exacerbations necessity for hospitalization increases. Patients with the highest mortality risk are those with 3 or more acute COPD exacerbations.27 During COPD exacerbation, oxidative stress and inflammation increase. In our study, the RDW/albumin ratio was found to be higher in patients hospitalized due to exacerbation in the last year compared with those without hospitalization (p=0.002).
Study limitations
The first limitation of our study is that it was a single-center study, retrospective, and only a small number of patients were included. We also analyzed the measures of RDW and albumin at the time of admission. Therefore, the values of dynamic changes in RDW and albumin during hospitalization were not considered.
In conclusion, our study found no relationship between LOS (≥10 days), mortality, and the RDW/albumin ratio in patients hospitalized for COPD exacerbation. Well-designed, prospective, and multicentre studies are necessary to confirm our findings.
Acknowledgment
The authors gratefully acknowledge David F. Chapman from Pure Medical Editing for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received September 21, 2023.
- Accepted November 29, 2023.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.