


Abstract
Objectives: To evaluate the role of sonography in revealing and characterizing liver transplant complications based on gray scale and color Doppler, describe the normal Doppler findings, and discuss the significance of distinguishing normal transient changes in the spectral waveform from findings that may suggests ominous complications.
Methods: We carried out a retrospective cross-sectional study at Prince Sultan Military Medical City, Riyadh, Saudi Arabia. The medical records and imaging studies of a total of 122 candidates who underwent transplantation between January 2016 to February 2022 were reviewed.
Results: Our results showed that most patients were males with the most frequent age group being those between 54-71 years. Hepatitis B virus and hepatic cellular carcinoma were the most common indications for transplants. A total of 95 patients received a graft from a living related donor. Regarding complications, biliary issues (including leaks and ducts dilation) were the second most frequent complication after collections. Vascular complications represented 7.4% of all complications and was the leading cause of death in 4.8% of cases. Among all vascular issues encountered during liver transplant, portal vein thrombosis was the most predominant. In respect to Doppler findings, portal vein velocities and resistive index of hepatic artery had re-averaged within 7-10 post-operative days in most patients.
Conclusion: Ultrasound plays crucial role in the post-operative management of compilations, facilitating early detection, which is substantial for the graft survival.
Unprecedented organ transplantation was once considered an insurmountable challenge and the theory did not hold water. However, it has become a leading therapeutic branch of surgery.1 Globally, the liver is the second most commonly transplanted organ.2 Liver transplantation has emerged as recognized and successful therapy for acute and chronic liver failure in just 60 years.3 Due to advancements in the surgical technique, immunosuppression, and imaging, the morbidity and mortality continues to decline. Imaging, in particular, is essential because it makes identifying intra and post-operative (early and delayed complications) issues easier and allows instant management. Intra and post-operative complications are categorized as vascular, biliary, parenchymal, and malignant. Although imaging is not typically used to diagnose the rejection of an allograft, it is crucial in ruling out mechanical causes of graft dysfunction that could mimic rejection. Complementary investigations such as computed tomography cholangiopancreatography and magnetic resonance cholangiopancreatography are used to detect complications.4 Intra-operative ultrasound, allows for the real-time and quantitative evaluation of the graft vasculature, and is considered as an integral component of the recipient surgery.5
Priority for liver transplantation is based on the model for end-stage liver disease (MELD) score, which measures the severity of end stage liver disease including bilirubin, creatinine, and international normalized ratio (INR).6 The Child-Pugh score works along with the MELD to assess the prognosis of chronic liver disease. A total of 5 clinical features are considered, which includes total bilirubin level, serum albumin, prothrombin time now measures as INR, the degree of ascites, and grade of hepatic encephalopathy.6-8 Additional different model for hepatic cellular carcinoma (HCC) candidates is the Milan criteria which includes a single tumor less than 5 cm in length or 3 tumors, each 3 cm or less, with no macro-vascular infiltration or metastasis. However, other studies state “a single nodule measuring less than 6.5 cm in diameter or up to 3 nodules, each measuring less than or equal 4.5 cm with a total tumor diameter of 8 cm or less”.9,10 The immune response to a transplanted organ comprises of cellular (lymphocyte-mediated specially T lymphocytes) and humoral (antibody-mediated) mechanisms.11 A major complication of liver transplantation that affects up to 40% of patients is acute cellular rejection (ACR). Usually, this problem appears within the first 3 months post-operatively. The majority of ACR bouts are asymptomatic, suspected only when liver enzyme increases.12
Immunosuppression aims to reach a modifiable standard therapy with a delicate balance between optimal immunosuppression and minimal side effects, using a combination of less used corticosteroids, particularly a calcineurin inhibitor (cyclosporine or tacrolimus) and an antiproliferative agent in 2 phases: intensive and maintenance.13-15 Liver allograft has the advantage of demonstrating lower rates of acute and chronic rejection, a resistance to antibody-mediated rejection as well as a higher likelihood of developing spontaneous tolerance.14
This study focused on living donor liver transplantation (LDLT) because it represents the majority of cases (91.3%). Due to the complex nature of the vascular anastomoses on LDLT the incidence of vascular complications (VCs) is greater than that in deceased donor liver transplantation (DDLT).15-17 The motive of the study is to detect the presence of significant post liver transplant complications which has a great impact on patients and graft survival. The main objective of the study is to evaluate the detection of intra and post-operative complications in liver transplant recipients using ultrasound.
Methods
This is a retrospective cross-sectional study carried out in the Department of Diagnostic Medical Imaging, Ultrasound Section at Prince Sultan Military Medical city, Riyadh, Saudi Arabia. The study duration was from January 2016 to February 2022 and the data were collected from December 2021 to February 2022. A total of 122 patients who underwent liver transplantation and its sequential follow up scans, from January 2016 to February 2022 were included. The range of follow up period is between 6 months to 6 years.
The inclusion criteria were adult patients above the age of 14 years and pediatric patients less than 14 years old who received a liver graft. The study was limited to patients who needed and underwent liver transplant surgery. The exclusion criteria were patients under consistent medical management and patients unfortunate to procced with transplantation. The following data were collected: patient’s age, gender, pathological history of the patients, and graft type. Assessments of the liver graft were established based on the gray scale appearance, color Doppler flow of the hepatic veins, inferior vena cava (IVC), portal vein, and hepatic artery. Furthermore, spectral waveform of hepatic veins, IVC, portal vein (velocity), and hepatic artery resistive index (RI).
The retrospective analysis of the transplant database was approved by the institutional review board, which granted permission to carry out the study (approval number: 1493). Permission to carry out ultrasound under the Radio Diagnostic Department was granted.
Following the research-based protocol, all patients were examined intra-operatively and, on the 1st, 2nd, and 3rd days post-operatively. Most patients were continuously assessed until September 2022, based on clinician’s requirements and the patients’ clinical condition. Patients were scanned using a curved linear and linear transducer with a center frequency ranging from 2.8-9 MHz. Linear-array transducers are often used for pediatric, thin patients, and scanning the liver surface in adults. Patients were examined in the supine position and in the left lateral decubitus if needed. The anterior subxiphoid, subcostal, and intercostal approaches are used to access the optimum window. Assessment of the liver parenchyma, biliary tree, and any fluid collection was obtained in grayscale, while the Doppler mode was used for hepatic vasculatures evaluation. Equipment used included: ultrasound machines with a transducer frequency of 2.8-5 MHz (curve linear) and 8.4-9 MHz (linear), ultrasound machines (GE LOGIQ E9), ultrasound portable (Philips CX50, Philips IU22, and Philips EPIC 6G), and ultrasound medical gel.
Statistical analysis
The data were analyzed using the Statistical Package for the Social Sciences, software statistics for Windows, version 25.0 (IBM Corp., Armonk, NY, USA) and Excel computer programs. Categorical nominal data are summarized as frequencies and percentages, whereas numerical data are represented in maximum, minimum, means and standard deviation (SD). The correlation between categorical variables was assessed using Pearson’s chi-squared test. A p-value less than 0.05 is typically considered to be statistically significant, in which the null hypothesis should be rejected. A p-value greater than 0.05 means that deviation from the null hypothesis is not statistically significant, and the null hypothesis is not rejected.
Results
Table 1 shows the demographic data of the patients. A total of 122 liver transplant recipients, between the age of 5 month to 72 years old were included. Both genders, adults, and pediatrics (pediatrics less than 14 years) were included. Patients were categorized into 5 age groups (0.5-14 years, 15-35 years, 36-53 years, 54-71 years, and 72-89 years). Graft appearance and graft donation types were demonstrated. Frequency distribution of general complications, incident of VCs, causes of death, and early mortality rates per year are also documented.
- Demographic data, complications, cause of death, and mortality/year.
Table 2 shows the descriptive statistics of Doppler parameters of portal vein velocity and hepatic artery RI during the follow up periods.
- Descriptive statistics of Doppler parameters.
Discussion
The study included 122 liver transplant recipients, between the age of 5 month to 72 years old; 59% were male and 41% were female, and 66.4% were adults and 33.6% were pediatrics. Patients have been categorized into 5 age groups (0.5-14 years, 15-35 years, 36-53 years, 54-71 years, and 72-89 years). Patients between the age of 54-71 years comprised the highest percentage, which was 39.9% of all candidates. A total of 112 individuals received a graft from a living donor, while only 10 candidates received a cadaveric graft.
Results showed the frequency distribution of primary diseases that led to the transplantation among the 101 living patients. Hepatic cellular carcinoma was the most common indication for transplantation in 19 (18.8%) patients, followed by progressive familial intrahepatic cholestasis (PIFIC) in 15 (14.9%) patients. Similarly, in 21 deceased patients, HCC and hepatitis B virus cirrhosis had the same percentage of 14.3%.
One of the post-operative routines includes an ultrasonic examination that evaluates the changes in the echotexture of the liver parenchyma. The scan demonstrates medium level echogenicity in 82 (67.2%) patients,15 (12.3%) heterogenous, and 25 (20.5%) hyperechoic.
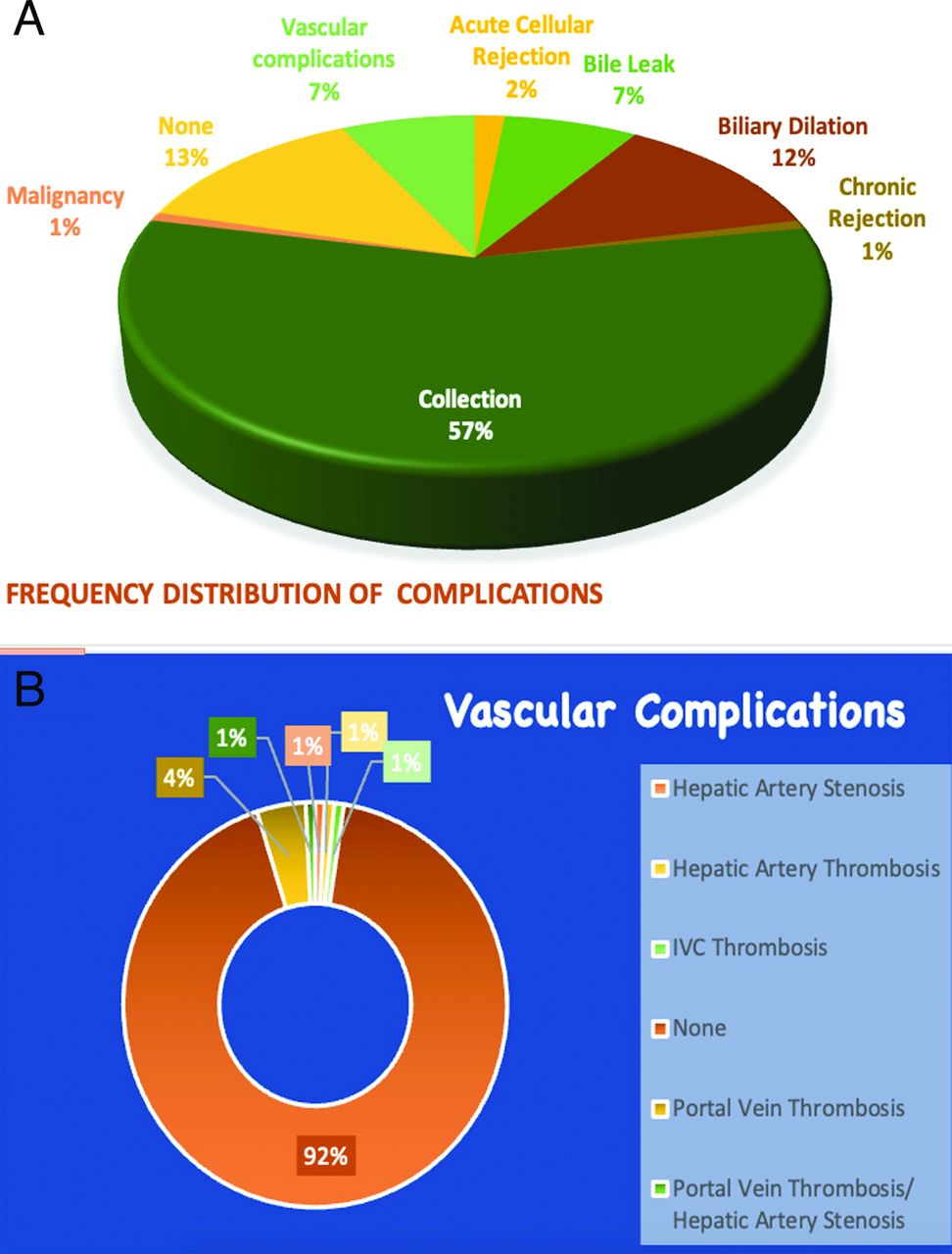
Regarding complications, 69 (56.6%) presented with variant types of fluid collections including hematomas, bilomas, abscesses, and ascites. Majority of the collections are clinically insignificant. They predominantly have simple imaging characteristics and resolve or decrease in size on follow-ups. A total of 16 (13.1%) patients experienced no complications, 15 (12.3%) patients suffered from biliary ducts dilation (Figure 1), 9 (7.4%) patients had bile leak, VCs were noticed in 9 (7.4%) patients, 2 (1.6%) patients faced ACR, chronic rejection occurred in one (0.8%) patient (Figure 2A), and recurrency of primary liver malignancy HCC documented in one (0.8%) case. The latter case had an underlaying cryptogenic liver cirrhosis with HCC, which remanifested after 2 years of transplantation.

- Dilated intrahepatic bile ducts seen 6 months after transplantation in a 17-month female who received a (left lobe) living related donor liver graft. Note the usage of color and power Doppler to differentiate between bile ducts and vasculatures.

- Frequency distributions. A) Frequency distribution of the overall complications. B) Frequency distribution of vascular complications.
Filgueira18 published a research article, which infers that, in spite of employing morphologic Milan or other criteria to nominate patients with HCC for liver transplant (LT), the chance of relapsed hepatic neoplasms is averagely 17.5% of the total cases accompanied with low chance of recovery. What is more, the study illustrates that in the neighborhood of 75% of the remanifesting tumor recurrent (TR) took place within the immediate 2 years post LT, in which is abreast with the current research findings. Notwithstanding, later than 4 years, the percentage plummets to 10% (Figure 3).18

- Hepatic cellular carcinoma representing a primary disease recurrency 2 years after liver transplantation. A) Gray scale sonogram revealing a hypoechoic lesion seen within the liver graft. B) Correlative magnetic resonance imaging abdomen demonstrating multiple hepatic lesions (blue arrows).
There are 2 major categories of post-liver transplant complications, non-vascular and vascular, which jeopardized the survival of graft and patient.19 Meticulously medical education emphasis particularly on VCs as it is considered the second cause of graft failure and mortality in orthotopic liver transplantation after rejection.19
A total of 113 (92.6%) patient suffered no complications of vascular nature. A total of 9 (7.4%) patients exhibit different types of VCs and 5 (4.1%) patients with portal vein thrombosis (PVT).
We found only one (0.8%) patient for each of the following complication: hepatic artery thrombosis (HAT), IVC thrombosis, and PVT combined with hepatic artery stenosis (Figure 2B).
Although the most frequent early VC following liver donation is HAT.20 The results show that PVT counts the majority of VC in contrary to literature. Also, a previous study by Kamal et al,21 was not in lining with the results and reveled that HAT counts the largest percentage of VC.21 With advanced medical technology, innovations, new microvascular anastomotic techniques, and a customized anticoagulation protocol might play substantial role to reduce the incidence of HAT, which might give the superiority to PVT over HAT in this study.
Furthermore, a brief questionnaire was provided to the liver transplant team surgeons with an agreement of the prementioned privileges. In this study, one patient suffered from PVT and HAT intra-operatively, which might be representing hyperacute rejection, after multiple attempts the surgeons managed to revascularize the vessels. Shortly after operation, the patient again developed PVT and HAT. Eleven days later, the patient underwent his second cadaveric retransplanting. Fifteen days after, the patient became deceased due to sepsis. A study carried out by Khalaf22 concluded that incidence of VC was significantly higher among the LDLT group compared with the DDLT group. The results of this study is abreast of the current finding, 7 out of 9 patients who suffered from VC received a graft from a living donor, 6 related doners and one non related.22
A total of 21 (17.2%) patients died during the research period time; deaths associated with cardiopulmonary causes (19.0%), infection (14.3%), sepsis (19.0%), primary nonfunctioning graft (4.8%), septic shock (4.8%), VCs (4.8%), renal impairment (4.8%), and other different cause comprise 28.6%. All deceased died within the first 6 months, the highest mortality rate recorded in 2017, then had hovered at roughly 13% from 2018-2022.
Cross tabulation of primary diseases shows no statistically significant association between neither gender (p=0.00) nor age (p=1.34). Additionally, correlating mortality with both graft type and primary disease depicts the same.
The Chi-square test was used to find the correlation between complications and age group among the living patients. The results illustrated that there is a statically significant correlation with a p-value of 0.039. In contrast, there is no association between the graft type and complications for both living (p=0.053) and deceased (p=0.706) patients.
In Table 2, the highest velocity of the portal vein was detected between days 1-7 measuring 146 cm/sec with a mean of 63.65±29.170 cm/sec. The velocities had been reduced gradually in the next scan between days 20-30, the maximum velocity detected had dropped to 100 cm/sec and mean of 38.05±17.885. Normally in post liver transplant, the average velocity at the anastomosis vicinity of portal veins is 58 cm/sec.23
Maximum values of the hepatic artery RI were recorded between days 1-3 (0.90), with a mean of 0.6907±0.10352. Evaluation on days 20-30 showed reduced numbers with a mean of 0.66±0.13714. The resistive index of hepatic artery at initial period of post-operative surgery normally stands at high reading. The flowing progressive days of the surgery, the velocity, and resistive index readings gradually normalized to the average level. Multifactorial contributes to the latter changes such as hepatic arterial spasm, tissue edema, increased cold ischemia time, greater age of liver donor, the surge of portal flow velocity, and the restrain of natural vasopressin hormone to dilate the hepatic artery due to the pre-operative liver disease (Table2).23
The results of the portal vein velocities and hepatic artery RI was within normal values and matched with previous studies that showed high readings in immediate evaluation, which reduced to normal within the following days (Figure 4).24

- Spectral wave measurement of hepatic artery resistive index in day 1 and 5. A) High RI of hepatic artery (0.84) one day after the transplantation. B) Normalization of the HA RI (0.65) by day 5. HA: hepatic artery, RI: resistive index
Study limitations
The limitations of the study include the legible patients in one major medical city. Additionally, patients are given priority and nomination to undergo the transplant based on medical polices, urgency, patients’ condition, capacity, and capability of the hospital. There was reduction in the number of cases during the COVID pandemic, which resulted in a low number of candidates in the research. The study can be carried on larger scale of patient numbers, years, hospitals, cities, and possible countries to get a wider scope of results. The most challenging complication that can hinder the success of intra and post-liver transplant surgery is the vascular.
In conclusion, ultrasound assessment for any medical complications during intraoperative and postoperative liver transplantation is a golden tool. This retrospective cross-sectional study of 95 living donors aims to evaluate these complications. Data are collected from patients who are scanned in intraoperative, 1st, 2nd, 3rd, and followed scans as needed. All data were obtained and statically processed. Hepatitis B virus and liver neoplasms are the most common indication for LT. Although post-operative collection and biliary issues are the most common complications in LT, VCs have highest rate of deaths. Previous studies indicate that HAT is the highest incidents of VCs, which is refuted in this study with PVT. Ultrasound has shown great implication not only to diagnose and predict complications, but also serves as a baseline study for further comparison. However, it can be technically challenging and sometimes difficult to interpret.
Acknowledgment
The authors gratefully acknowledge Dr. Al-Bahili, Director of Multi-organ Transplant Center Consultant Surgeon, Prince Sultan Military Medical city, Riyadh, Saudi Arabia, for giving his valuable time enlightening us with his tremendous experience and knowledge. Extending a heartfelt thanks to the whole team of the Organ Transplant Center in Prince Sultan Military Medical city, Riyadh, Saudi Arabia, for facilitating the access to patients’ data. The authors also would like to extend their gratitude to Dr. Mohammed A. Safhi (radiologist) for his great review of the images and correction. The authors also would like to thank Prabh Grewal at Editage (https://www.editage.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 15, 2024.
- Accepted August 30, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.