


ABSTRACT
Objectives: To compare the effectiveness of providing telepharmacy anticoagulation to on-site clinics in achieving optimal outcomes for patients newly starting warfarin.
Methods: This single-center retrospective cohort study included adult patients who started warfarin for the first time and were monitored by clinical pharmacists either on-site or via telepharmacy anticoagulation clinics between January 2017 and March 2024. The primary outcome is to compare the time in therapeutic range (TTR) between the 2 groups. The secondary outcome is the occurrence of anticoagulation therapy–related complications.
Results: We included 191 patients, with 77 in the telepharmacy group and 114 in the on-site group. The baseline characteristics were similar for both groups. The primary outcome— time in therapeutic range (TTR)—was not significantly different between thetelepharmacy and the on-site groups (50% versus 53.8%, p=0.455) and remained so after univariable and multivariable adjustments (OR [odd ratio]= 0.63, p=0.14 and OR=0.58, p=0.102). Additionally, there were no significant differences in secondary outcomes, including thromboembolism and bleeding (p=1 for both).
Conclusion: This study demonstrates that patients who receive warfarin for the first time at an anticoagulation clinic can use the telepharmacy method without the fear undesirable outcomes. Results of this study support the continued use and expansion of telepharmacy services in Saudi Arabia. However, further research larger sample sizes and multiple centers is needed to confirm these findings.
For the past century, warfarin has been the cornerstone of oral anticoagulant therapy, despite its restricted safety profile and small therapeutic window. (1,2).Warfarin remains essential for the treatment of individuals with antiphospholipid syndrome, valve disease, and chronic kidney disease even with the introduction of new direct-acting anticoagulants.1
Warfarin’s effectiveness depends on the careful management of its anticoagulation effects by maintaining an international normalized ratio (INR) of 2.0–3.0 or 2.5–3.5, depending on the indication.2 The percentage of time during which a patient’s INR values remain within the target range is known as the time in therapeutic range (TTR). The Rosendaal method categorizes TTR as either good (>70%), intermediate (50–70%), or inadequate (<50%).3 Due to its significant ability to predict undesirable outcomes such as bleeding and thrombosis, TTR has been found in previous research to be widely accepted as an intermediate outcome to assess anticoagulation treatment.4 Several factors were thought to influence TTR, including patient-related factors, such as age, gender, socioeconomic status, indications, comorbidities, genetic predisposition, and medications that interact with warfarin, as well as factors specific to the healthcare center and country.5 Additionally, time on anticoagulation therapy was recently found to be a predictor of good TTR, indicating that patients who have used warfarin for a long time are more likely to have better TTR regardless of other factors.5
In order to properly manage a patient’s warfarin dosage, professional anticoagulation services from qualified healthcare practitioners must be used to closely monitor INR. Pharmacist-managed anticoagulation clinics are widely accepted due to better anticoagulation control, decreased adverse events, and possibly decreased healthcare costs.6-8
Before the COVID19 pandemic, telepharmacy anticoagulation clinics weren’t common;nevertheless, their usage during the pandemic and afterwards has shown benefits for patients, healthcare providers, and healthcare organizations. These advantages include convenience, improved patient experience, reduced exposure to infectious disease, reduced healthcare burden, rapid access to care, and the ability to optimize the duration of visits.9,10 However, individuals who have previously taken warfarin—also referred to as “warfarin-experienced patients”have been a majority of the participants in research comparing telepharmacy anticoagulation services to in-person treatments. The results of these studies showed a comparable efficacy in TTR between telepharmacy clinics and on-site clinic.11-14 This is not surprising since patients who have used warfarin for a long time are knowledgeable and experienced in dealing with warfarin. During the post-pandemic period, a massive shift toward using telehealth occurred, including the provision of telehealth services for patients starting to use warfarin for the first time.
In Saudi Arabia, several studies have evaluated the effect of shifting warfarin patients from on-site, in-person clinics to a telehealth model during the COVID-19 pandemic, and they showed comparable TTR.15,16
While previous studies have demonstrated the safety and efficacy of telepharmacy anticoagulation services in warfarin-experienced patients, little is known on the efficacy of initiating new warfarin patients via telepharmacy clinics. Therefore, the aim of this study is to compare the effectiveness of providing telepharmacy services to providing on-site services in achieving optimal outcomes for patients newly initiated on warfarin.
Methods
This is a retrospective cohort study that was carried out at the anticoagulation clinics at Security Forces Hospital in Riyadh, Saudi Arabia. It is a tertiary care facility that mostly serves military personnel and their families from all over Saudi Arabia. The pharmacist-lead clinic was first implemented in the late 1990s as an on-site clinic. However, it shifted to providing telepharmacy services during the COVID-19 pandemic in 2020 and, after the pandemic, continued to deliver services mostly through telepharmacy, except when patients requested that they be followed on-site, which is rare.
The INR results for all followed patients were determined using blood samples obtained via venipuncture in hospital laboratories. Additionally, the clinic uses a point-of-care coagulation testing device called CoaguChek to measure INR using blood samples obtained via finger-stick for on-site patients only as a backup for patients who did not undergo the test earlier in the laboratory. Fortelepharmacy clinic patients, the first 2 visits were on-site,and then all patients were followed up via telephone. The clinical pharmacist contacted the patients by telephone after the blood test results were obtained (whether through a laboratory test or the patient’s own CoaguChek test) to manage their anticoagulation therapy. Subsequently, the data were tracked and documented using electronic medical records. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) were adhered to.17
In 2020, the clinic switched from providing on-site to providing telepharmacy services. Consecutive patients were included in the study before and after implementing telepharmacy to obtain the desired sample (both chronologically and bi-directionally). The resulting date range for the study period was January 2017 to March 2024.
We included all adult patients who were followed in the anticoagulation clinic and received warfarin for the first time, which ensured mutually exclusive groups. Patients were excluded if they had hepatic impairment, were followed up in person more than twice within the first three months or more than three times during the first 6-month period, died during the first 6 months, were no longer on warfarin within the first 3 months, or were followed up for less than 3 months. Patient consent was not required because this was a retrospective study.
The intervention group consisted of patients who were monitored via telepharmacy between 2020 and 2024. The control group consisted of patients who started warfarin and attended the on-site clinic between 2017 and 2020. Both groups received warfarin for conditions such as deep vein thrombosis (DVT), pulmonary embolism (PE), atrial fibrillation (AF), or stroke. All INR readings obtained during the first 6 months that patients took warfarin were obtained and compared.
To guarantee the accuracy and consistency of the data we collected, we adhered to a systematic procedure for data collection. Initially, we took a list of every patient that was seen at the clinic over the specified time frame. Three investigators then gathered and entered all of the data into the Research Electronic Data Capture (REDCap) online platform. A random 10% sample of the data were checked by other investigators and data were cross-referenced with the hospital medical records of the patients to ensure the accuracy of the data.
The data extracted from the medical records of each patient included demographic characteristics, indications for starting warfarin therapy, mode of clinic follow-up, comorbidities, concurrent use of antithrombotic medications, concurrent use of non-steroidal anti-inflammatory Drugs (NSAID)thatcould increase risk of bleeding, target INR, planned duration of anticoagulation therapy, and all INR readings during the first 6 months.
The primary outcome was theTTR percentage in all patients who were followed-up in person on-site and via telepharmacy. All available INR readings for the first 6 months of warfarin treatment were used to estimate TTR using the Rosendaal method (the percentage of time that INR was therapeutic). The secondary outcome was the occurrence of anticoagulation therapy–related thromboembolic or bleeding complications, the frequency of extreme INRs, and the percentage of patients with TTR≥ 60%. Thromboembolic complications include deep vein thrombosis (DVT), pulmonary embolism (PE), and stroke. Bleeding complications includes both major and minor bleeding. The International Society on Thrombosis and Hemostasis defines major bleeding as i) fatal bleeding; ii) symptomatic bleeding in a critical area or organ (such as intracranial, intraspinal, intraocular, retroperitoneal, intraarticular, pericardial, or intramuscular with compartment syndrome); or iii) bleeding causing a fall in hemoglobin level of 2 g/dL (1.24 mmol/L) or more, leading to transfusion of 2 or more units of whole blood or red cells. Minor bleeding is as any sign or symptom of hemorrhage that does not fit the definition of a major bleed but require medical attention from a trained specialist; necessities hospitalization or higher care; or demands an in-person assessment.18 Extreme INR is defined as INR <1.5 or >4.6.19
The study was carried out according to principles of Helsinki Declaration and was reviewed and approved by the Investigational Review Board of the Security Forces Hospitalin Riyadh, Saudi Arabia.
Statistical analysis
Statistical analysis was performed using SPSS, version 27 (IBM, Armonk, NY, USA). Continuous variables were reported as mean and standard deviation if they followed a normal distribution and as median and interquartile range (IQR) if they did not follow a normal distribution. Categorical variables were presented as frequency and percentage. To compare continuous variables between the 2 independent groups, either a t-test or Mann–Whitney U test was used, depending on the distribution of the data. For categorical variables, the chi-squared test or Fisher’s exact test were used as appropriate. Whenever multiple comparisons were conducted, the Bonferroni–Holm method was used to control the family-wise error rate. To examine the association between study variables and the outcome of achieving TTR ≥60%, we conducted univariate logistic regression analysis. All variables with a p-value <0.2 in the univariate analysis were included in the multivariate analysis model. A one-sided p-value <0.05 was considered statistically significant for all tests.
Results
We reviewed the records of 289 patients who either attended the on-site coagulation clinic or received telepharmacy services between February 2017 and March 2024. Approximately 98 patients were excluded for various reasons, the most common of which was that they were followed for less than three months (Figure 1). A total of 191 patients were included in the study: 77 (40.3%) in the telepharmacy group and 114 (59.7%) in the on-site group. We had no missing data. Around 99% of the included patients were Saudis, with 92% from Riyadh Region; this profile was similar in the 2 groups (p>0.05). Baseline characteristics were analyzed, and no statistically significant differences were found between the 2 groups (Table 1). In this cohort, the most common indication of using warfarin was DVT (30.4%), and around 73% of patients intended to continue warfarin indefinitely.

- Study participants enrollment process.
- Baseline characteristics of the study participants (N=191).
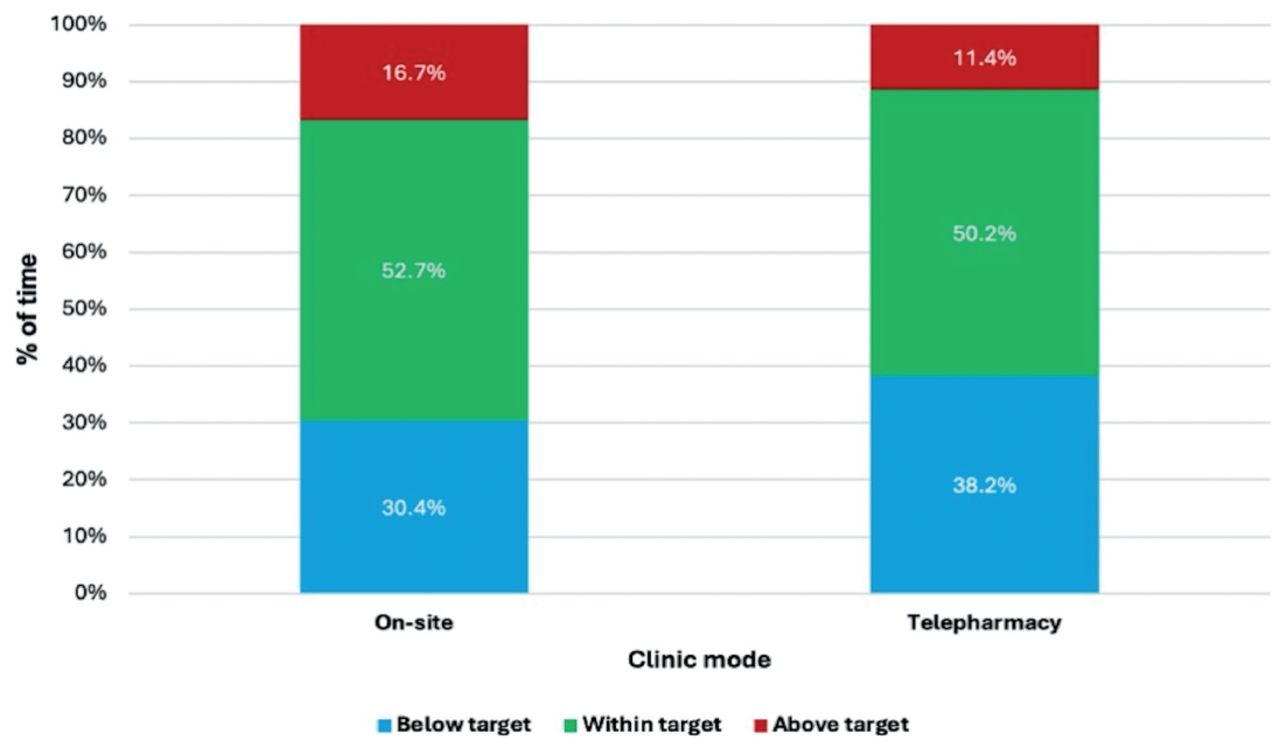
The TTR for the on-site clinic and the telepharmacy clinic was comparable (53.8% and 50%, p=0.455). Overall, the time above, below, and within the therapeutic range was comparable between the on-site and the telepharmacy clinic (Figure 2). The secondary outcomes of bleeding, thromboembolic events, extreme INRs, and TTR>60% were comparable between the 2 groups (Table 2).

- Time in therapeutic range during the on-siteand telepharmacyanticoagulation clinics (p=0.455). TELE: telepharmacy
- Outcome measure comparison between on-site and telepharmacy in newly initiated warfarin patients.
Secondary analysis (adjusting for confounders)
To further investigate the validity of the results, we assessed the predictors of TTR. We chose a dichotomous outcome of TTR ≥60 as a point of analysis using univariate and multivariate analysis. Univariate analysis indicated that males were more likely to achieve TTR>60%. However, after adjusting for multivariate analysis, none of the measured baseline characteristics affected the achievement of TTR ≥60% (Table 3).
- Comparing telepharmacy and standard clinic follow-up for warfarin-naive patients.
Discussion
To the best of our knowledge, this is the first study to compare the outcomes of patients starting warfarin treatment who are followed by a telepharmacy anticoagulation clinic with those who are followed at an on-site clinic. The results showed no statistically significant differences in TTR between the 2 groups (TTR of 50% and 53.8%, p=0.445). This result remained the same even after adjusting for confounders.5 Previous studies (5,11,13,14)have shown that being on warfarin for a long time is predictive of better TTR.5 Therefore, comparing telepharmacy to face-to-face clinic in warfarin-naïve patients is important to estimate the true effectiveness of telepharmacy and assess the appropriateness of switching to a full telepharmacy mode.
Results from this study add to the existing literature, that following warfarin-naïve patients via a telepharmacy anticoagulation clinic is comparable in efficacy to services they receive at an on-site clinic. Our findings are in general agreement with 2 previous Saudi studies. A study by Al Ammari et al16 investigated the switch to telehealth anticoagulation monitoring during the COVID-19 pandemic in a single center and found the average TTR to be 57.81%± 32.08.Another study by Alanzi et al15 evaluated the provision of telepharmacy services in a single center. Using a crossover design, they compared the TTR of the same patients before and after switching totelepharmacy during the pandemic. They found that TTR was 54.6% while the patients were followed by the on-site clinic and 50% when they switched to the telepharmacy clinic, with no statistically significant difference between the 2 types of services.15
Our results agree with several studies that compared telepharmacy services to on-site anticoagulation management. A meta-analysis by Sakunrag et al12 included the pooled estimate of seven US studies and showed no difference in TTR among patients who received telephone services compared with those who received the usual care. A meta-analysis by Ferreira et al14 included the pooled estimate of 25 randomized control trials (RCTs) and found that TRR was comparable between the 2 groups. A systematic review and meta-analysis by Tran et al13 included a pooled analysis of 9 studies and found that the TTR of in-person and telepharmacy patients was comparable.
While the Rosendaal method is the most common and most reliable method for calculating TTR, the categorization of TTR and the reported international average varies in the literature. The clinical guidelines of Thrombosis Canada (2017) arbitrarily define a good INR as TTR >60%.20 In our study, the average TTR was in the range of 50%, which is consistent with several real-world studies from various regions indicating an average TTR of around 50%.21–24
In our study, the secondary outcomes of thromboembolic and bleeding events, extreme INRs, and TTR ≥60% were not significantly different between the 2 groups. Our results are in agreement with Sakunrag et al,12 who found that patients receiving telehealth services had similar incidents of extreme INR, major bleeding, thromboembolic events, and hospitalization as those receiving in-person services. Additionally, the meta-analysis of RCTs by Ferreira et al14 showed a comparable rate of bleeding and mortality, and a trend of reduction in thromboembolic events in telepharmacy group. However, another meta-analysis by Tran et al13 favored telepharmacy in the reduction of bleeding and hospitalization but not thromboembolic events. It is important to note that our study was retrospective which might limit the accurate capture of these adverse effects. Lastly, the low number of included patients in our study might lead to underestimation of the adverse events reported. Therefore, a prospective study might be needed to validate these secondary outcomes.
Our study is subject to the inherent limitations of a retrospective study conducted in a single-center tertiary care institution. The quality of some data is not optimal. Several factors that may affect TTR were not measured, such as socioeconomic factors. Additionally, patients’ compliance was not measured due to the retrospective nature of the study. Therefore, a prospective multi-center study with a larger sample size is needed to confirm these findings. Moreover, long-term follow-up studies should be conducted to assess the sustainability and durability of outcomes achieved by telepharmacy anticoagulation clinics.
In conclusion, this study demonstrates that patients who are starting warfarin treatment for the first time can confidently use telepharmacy services without fear of undesirable outcomes. This conclusion is supported by the absence of significant differences in the outcomes of the patients who received telepharmacy care and those who attended the anticoagulation clinic, and in the absence of any significant differences between the 2 groups in terms of secondary outcomes, such as thromboembolism and bleeding events. This study adds to the research that supports thetelepharmacy management of warfarin treatment, specifically for patients starting warfarin for the first time. Our findings provide promising evidence that telepharmacy services can be a safe and effective alternative to on-site care for patients newly started on warfarin. This approach offers potential benefits in terms of healthcare resource utilization, such as reducing the need for hospital visits and potentially lowering healthcare costs, yet further research in this domain is needed.
Acknowledgment
We greatly appreciate the support of Princess Nourah bint Abdulrahman University in funding this research through: Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2024R167), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
We would like to acknowledge Scribendi (www.sceibendi.com) for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received August 9, 2024.
- Accepted November 4, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.