


Abstract
Objectives: To determine the incidence of Clostridioides difficile infection (CDI) and the frequency of known risk factors.
Methods: A prospective hospital-based surveillance for CDI, according to the Centers for Disease Control and Prevention criteria, was carried out from July 2019 to March 2022 for all inpatients aged more than one year in Prince Sultan Military Medical City, Riyadh, Saudi Arabia.
Results: A total of 139 cases of CDI were identified during the survey among 130 patients admitted in the hospital. Most cases were incident (n=130; 93.5%), and almost three-quarters (n=102; 73.4%) were hospital-onset (HO) CDI, with an incidence rate of 1.62 per 10,000 patient days (PD). The highest rates were noted in intensive care units with an incidence rate of 3 per 10,000 PD and wards for immunocompromised patients with an incidence rate of 2.72 per 10,000 PD. The most prevalent risk factor for CDI was acid-reducing drugs (72.6%). Vancomycin (48%) and ciprofloxacin (25%) were the most frequently prescribed antibiotics for patients with CDI. Clostridioides difficile infection complications were identified in 5.7% of the cases, with a reported 28-day mortality rate of 3.8%.
Conclusion: In our hospital, HO-CDI incidence rate is lower than that in high-income countries. National multicenter surveillance is needed to evaluate the actual burden of CDI in Saudi Arabia.
Clostridioides difficile (C. difficile) is a gram-positive, spore-forming, anaerobic bacillus that produces 2 large toxins, A and B, which cause diarrhea and colitis in patients whose normal colonic microbiota is compromised by prior antimicrobial treatment or other factors. Over the past 2 decades, the incidence and severity of C. difficile infection (CDI) have significantly increased worldwide.1 In the United States, CDI is a major health threat; in 2017, CDI caused 223,900 hospitalized cases and 12,800 deaths.2 A review of specific cases of CDI identified during surveillance revealed that 65.8% of the cases were healthcare-associated, but only 24.2% had the onset during hospitalization. Most patients diagnosed with community-associated CDI report exposure to outpatient healthcare settings.3 In addition, the incidence was higher in patients who were aged ≥65 years, women, and Caucasians. More than 40 risk factors are involved in the development of CDI, and host-related characteristics, including age, gender, race, and comorbidities, are well-described risk factors.4 Comorbidities, such as diabetes mellitus, malignancies, and inflammatory bowel disease, may also contribute to the pathogenesis of CDI.4 Since the use of gastric acid-suppressing drugs, such as proton pump inhibitors (PPIs) and histamine-2-receptor antagonists, is prevalent, their association with C. difficile has been thoroughly evaluated.5 In 2012, a meta-analysis revealed that PPI use increased the risk of CDI 2-fold.6 In addition, excessive use of broad-spectrum antibiotics can increase the risk of CDI by disrupting normal flora, thereby facilitating the proliferation of C. difficile.7,8 A systematic review and meta-analysis that aimed to confirm the association between antibiotic use and CDI indicated that the use of clindamycin and third-generation cephalosporins was strongly linked to healthcare facility-associated CDI.9 Since limited data on the risk factors and disease epidemiology of CDI is available in Saudi Arabia, further studies are required to identify patients at high risk for CDI in our community.10 Therefore, this study was carried out to estimate the incidence of hospital-onset CDI (HO-CDI) in our institution (a tertiary medical center) in Saudi Arabia and to determine the frequency of known risk factors that influence the development of CDI. We also assessed the outcomes and mortality rates of patients with CDI in the study group.
Methods
A prospective surveillance study was carried out among all patients who tested positive for C. difficile between July 2019 and March 2022 at the Microbiology Laboratory of Prince Sultan Military Medical City in Riyadh, Saudi Arabia. It is a tertiary medico-surgical teaching hospital, with 1350 bed capacity, including intensive care units (ICUs) (adult, pediatric, and neonates), oncology, organ transplant units, and all types of surgeries.
All unformed stool samples were tested for C. difficile toxin A or B and confirmed by GeneXpert polymerase chain reaction (Cepheid’s GeneXpert® System, California, USA). We excluded CDI-positive tests for outpatients, those aged less than one year, and duplicated cases, defined as C. difficile toxin-positive laboratory results from the same patient within 2 weeks of the most recent (previous) positive stool sample.
The institutional review board of Prince Sultan Military Medical City, Riyadh, Saudi Arabia, approved this study (approval no.: E-2059). All procedures were carried out based on the Helsinki declaration.
All definitions and related patient information, including known risk factors, were recorded by trained infection control practitioners based on patient medical electronic files, following the Centers for Disease Control and Prevention’s National Healthcare Safety Network (NHSN) criteria.11 Thus, we considered the following definitions: I) incident case CDI: cases with a C. difficile-positive stool specimen obtained greater than 8 weeks after the most recent (previous) positive stool sample for that patient or the first time; II) recurrent CDI: CDI cases with positive C. difficile stool specimens between 2-8 weeks after the last positive specimen; III) healthcare facility-onset (HO): specimen collection (event) date after the first 3 days of admission; IV) community onset (CO): specimen collection (event) date is in the first 3 d of admission; V) community onset healthcare facility-associated (CO-HA): specimen collection (event) date is in the first 3 days of admission but within 4 weeks of the last discharge; and VI) HO-CDI incidence rate: number of hospital-onset C. difficile infections noted in the location (if monitored by inpatient location) or facility (if monitored by overall facility-wide inpatient) / number of patient days for the location or facility × 10,000
Statistical analysis
Data entry and analysis were carried out using Excel 2016. We determined means and frequencies (%) for quantitative and qualitative variables. Incidence rates were calculated as mentioned above.
Results
During the surveillance period, 631,991 patient days (PD) were recorded in our hospital, and 139 cases of CDI were diagnosed among the 130 inpatients. The age of our population ranged from 1.4-99 years, with a mean age of 49.6 years; males constituted 51.5%. Patients aged 65 years or greater represented 37.7% among infected cases whereas 17.6% (n=23) were pediatric cases (Table 1).
- Characteristics of inpatients with Clostridioides difficile infection (n=130).
Most cases were incident (n=130; 93.5%), and almost three-quarters (n=102; 73.4%) were HO-CDI cases, with a mean incidence rate of 1.62 per 10,000 PD (Table 1).
The mean CDI incidence rate for the hospital over the study period was 1.62 cases/10,000 PD, with a minimum of 1.34 in 2020, and a maximum of 1.97 during the last 6 months of 2019. When we analyzed this incidence rate by location, we found that the highest rates were observed in ICUs during the last 6 months of 2019 with 4.73 per 10,000 PD and 2021 with 3.87 per 10,000 PD. However, oncology, solid organ transplant units, and hematopoietic stem cell transplantation recorded the highest mean incidence rates in 2020 and in the first quarter of 2022 (Figure 1).

- Hospital onset-Clostridioides difficile infection incidence rate from July 2019 to March 2022 in Prince Sultan Military Medical City, Riyadh, Saudi Arabia. ICU: intensive care unit, SOT: solid organ transplant, HSCT: hematopoietic stem cell transplant
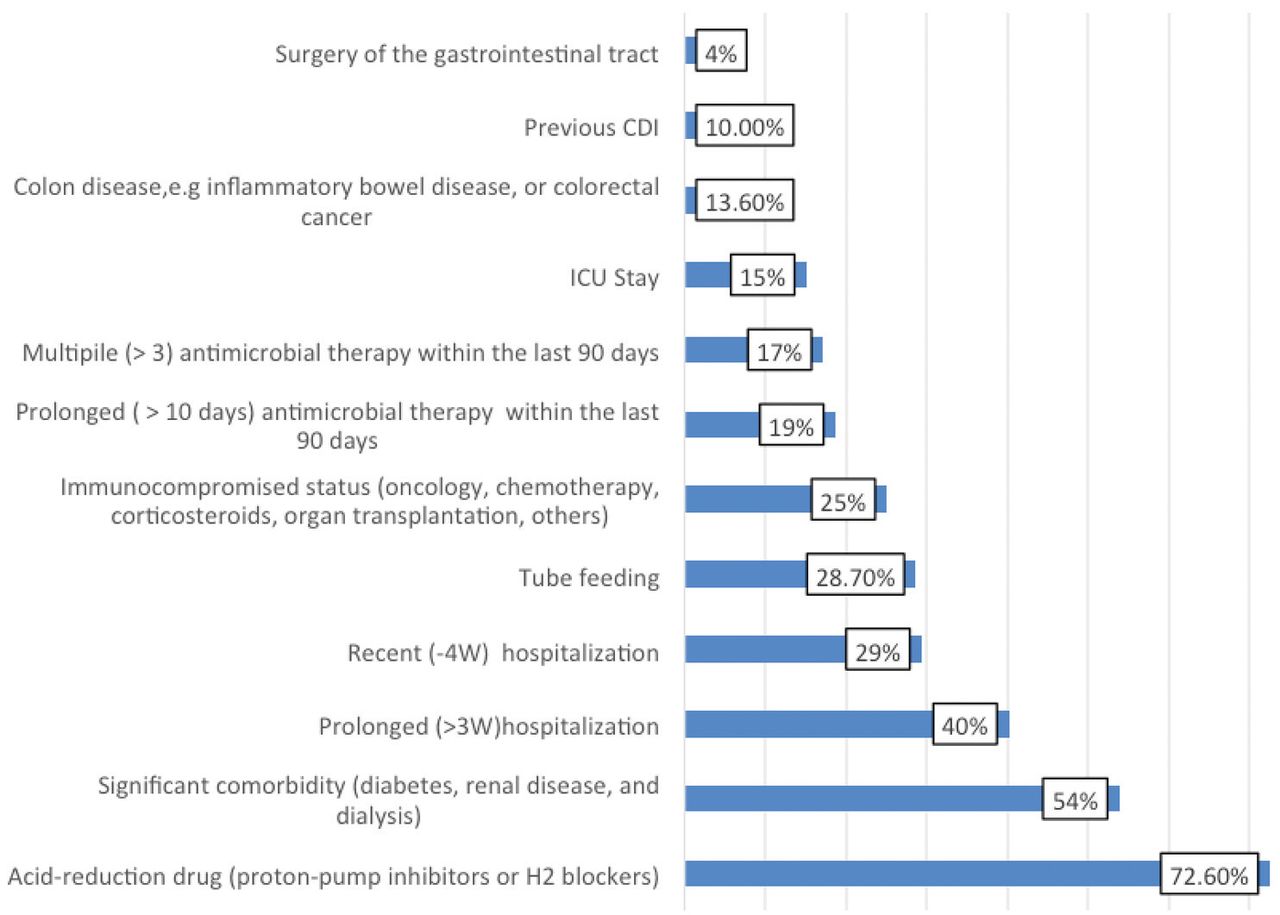
Approximately one-third (33%) of the patients exhibited more than 3 risk factors associated with CDI. Figure 2 shows that the use of acid reduction drugs (72.6%), existing significant comorbidities (54%), and prolonged hospitalization for more than 3 weeks (40%) were the most prevalent risk factors identified in our patients.

- Prevalence of known Clostridioides difficile infection (CDI) risk factors noted in our study. ICU: intensive care unit, W: week
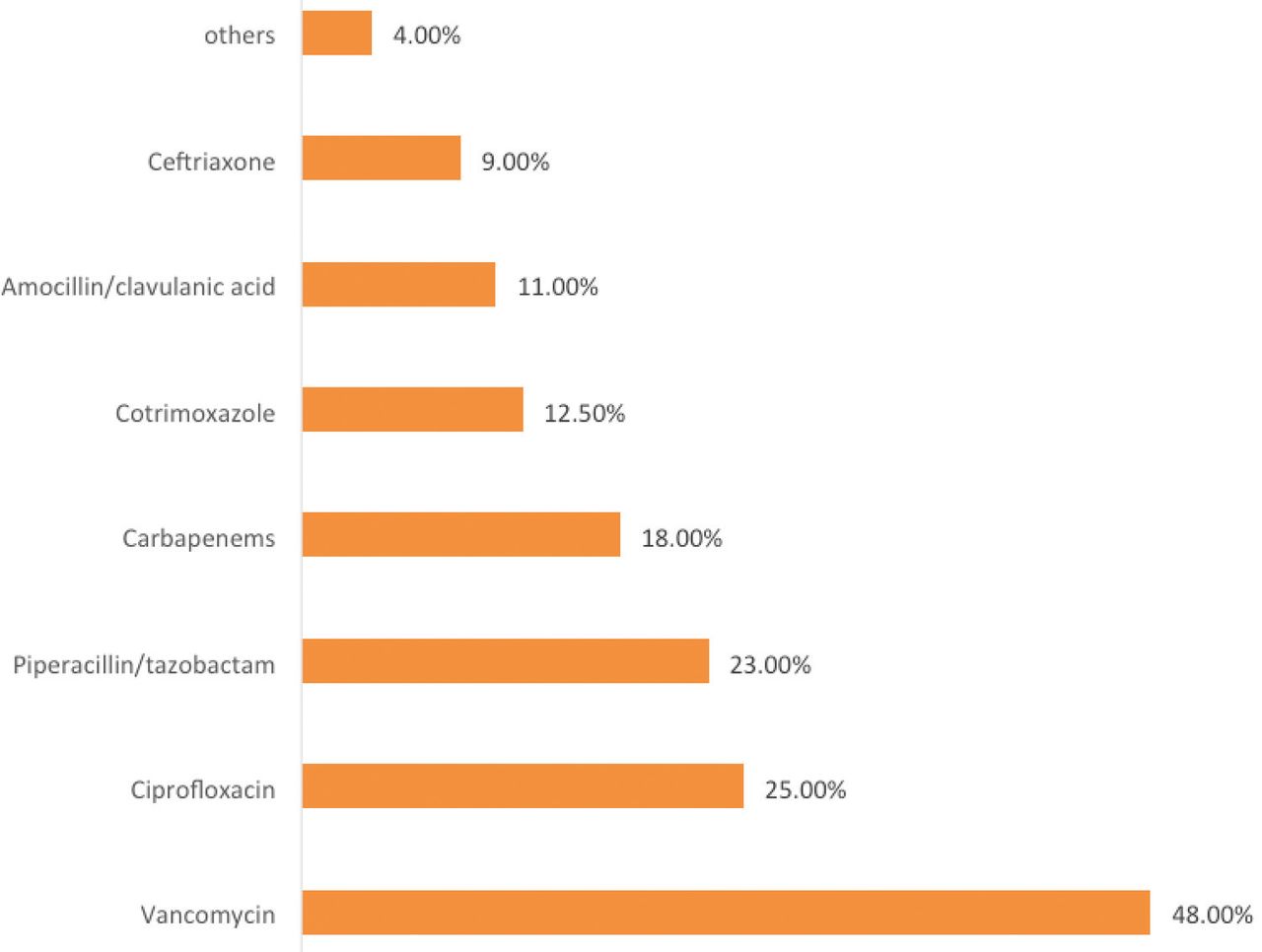
At the time of CDI diagnosis, 40% of the patients were administered one or more antibiotics. The most commonly prescribed drugs were vancomycin (48%), ciprofloxacin (25%), and piperacillin/tazobactam (23%, Figure 3).
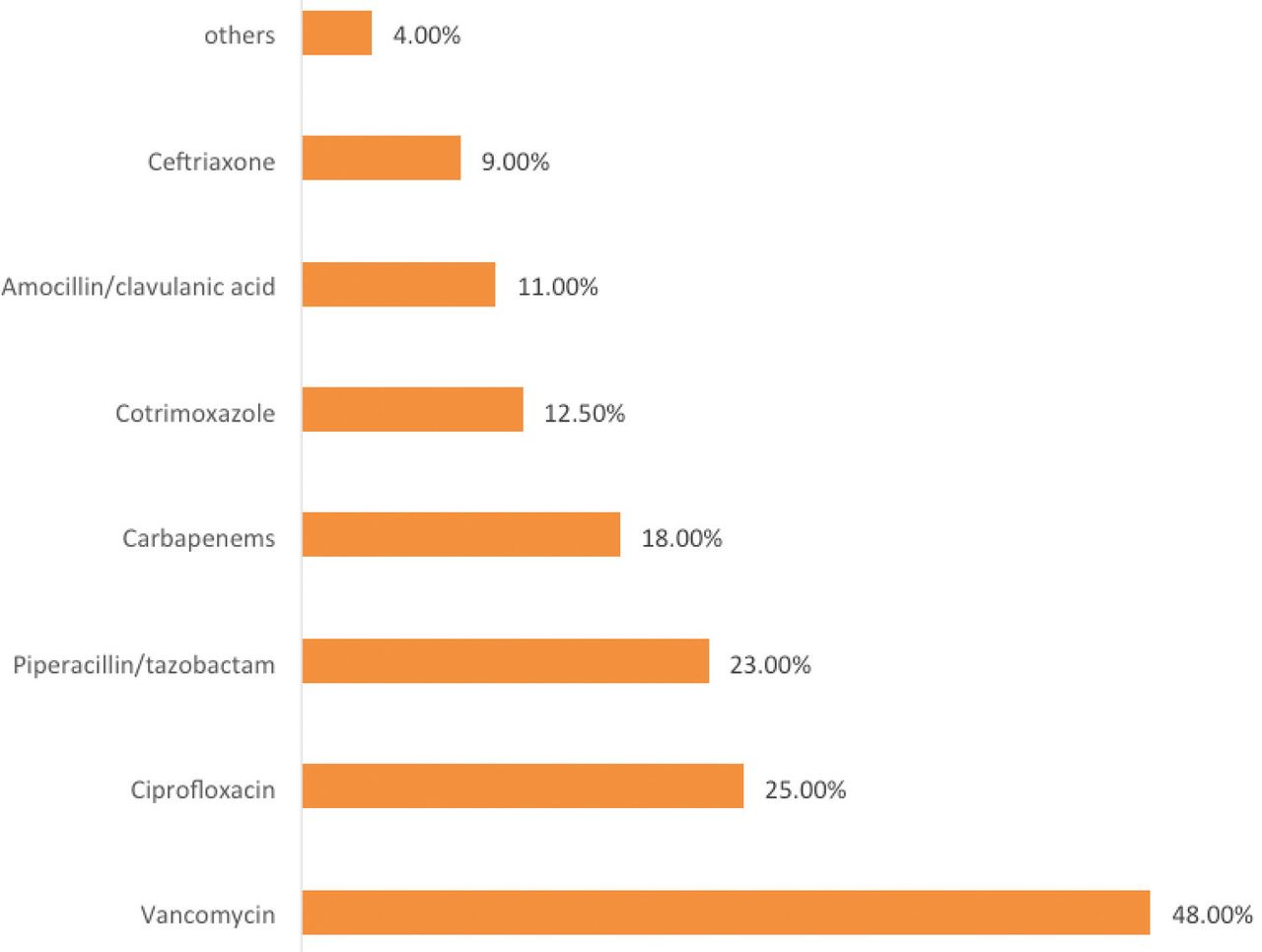
- Antibiotics prescribed during Clostridioides difficile infection diagnosis.
Most patients recovered completely without complications (94.3%). However, 2 patients developed toxic mega colon and refractory colitis occurred in one case.
The reported mortality rate at a 28-day post infection was 3.8%, with no evidence of a direct effect of CDI on death.
Discussion
In the last several years, published studies carried out in different Saudi Arabian hospitals have shown a low cumulative prevalence or incidence of CDI. However, most of these results were based on monocentric or retrospective surveillance and were carried out without the use of NHSN definitions.12,13 In the current survey, we calculated HO-CDI incidence rate based on the NHSN classification, which enables comparison with international data and our incidence rate was found to be much lower (1.62 cases/10,000 PD) compared to the NHSN rate of 7.2 per 10,000 PD.14 In a previous surveillance carried out in our institution from June to November 2015, although the authors added CO-HA CDI to their population, the CDI incidence rate was 3.5/10,000 PD.15 The same finding of low HO-CDI incidence rate was noted in an old study carried out in 2007 and 2008 at a single hospital in Dhahran, Saudi Arabia, showed an incidence rate of 1.7-2.4/10,000 PD.16 In addition, in a recently published report of a retrospective CDI surveillance in tertiary general hospitals, Al Tawfeek et al17 noted that the rate of HO-CDI per 10,000 PD increased from 0.09 to 2.2 from 2001 to 2018. Although studies in Saudi Arabia are rare and retrospective, the reported low rates of CDI can be explained by multiple factors such as the absence of active surveillance in a majority of Saudi Arabian hospitals and the absence of diagnostic tools to confirm the presence of CDI in some facilities. Moreover, compared to western countries, emphasizing personal hygiene in Islamic culture, in connection with the importance of ablution and the use of water for cleaning after defecation, seems to contribute to reducing the risk of CDI transmission in our country.
This study aimed to determine the frequency of risk factors for CDI. Therefore, almost one-third of patients had at least 3 risk factors associated with CDI. The most prevalent risk factor noted among our study population was the use of acid-reducing drugs (PPIs and histamine-2-receptor antagonists; 75%), and its association with an increased risk of CDI has been established in previous studies.15,18 Therefore, having significant comorbidities (uncontrolled diabetes, ischemic heart disease, and others) and being exposed to tube feeding are known to be significantly associated with CDI and they were frequently reported among our population, with rates of 54% and 28.7%.15,19 A combination of these factors can act as an early predictor of preventive measures in high-risk groups. In addition, a history of antibiotic use is known to increase the risk of developing CDI by 7- to 10-fold during treatment and up to one month after treatment, and approximately 3-fold for 2 months thereafter.20,21 However, obtaining accurate information from the patient history over the last 3 months was difficult. Therefore, we included only patients who were receiving antimicrobial therapy (40%) at the time of CDI. Many antibiotics are associated with an increase in CDI, most of which are fluoroquinolones, clindamycin, penicillin, broad-spectrum combinations (broad spectrum), cephalosporins, and carbapenems.22,23 A reduction in fluoroquinolone use across the United Kingdom population has resulted in decreased CDI incidence across the country.24 These findings indicate the need for controlled use of antimicrobials and reinforcement of antimicrobial stewardship programs as important measures for the prevention of CDI. During our survey, although the highest incidence rate of HO-CDI was noted in ICUs; a large proportion of patients were diagnosed in medical surgical wards. This is consistent with the findings of a 6-year retrospective study carried out in an Italian hospital, which CDI cases were more frequent in the medical ward than in the ICU.25 According to another prospective surveillance study carried out in Eastern Europe, patients were more likely to acquire CDI in a medical ward than in other wards.26 However, this was expected as patients admitted to a medical ward tended to stay longer in the facility. Several CDI-associated risk factors should also be considered, including hospital infrastructure (multi-bedded rooms), scarcity of handwashing facilities, patient-to-nurse ratio, patient placement, availability of supplies such as personal protective equipment and their correct utilization, antimicrobial stewardship programs, adherence to environmental hygiene measures (namely, use of sodium hypochlorite), and patient visitors/caregivers. Further studies on the significance of these risk factors in reducing the CDI rates in clinical settings are required. This surveillance data analysis illustrates CDI incidence in the largest military hospital in Saudi Arabia, which can be used as a foundation for future studies on the importance of prevention and control measures to lower CDI incidence.
Study limitations
This was a monocentric study, carried out over a few years, and involved only inpatients with CDI; therefore, the results should be interpreted with caution. National CDI surveillance (CO and HO), following the NHSN criteria, should be carried out to evaluate the actual burden of CDI in Saudi Arabia. Although the risk factors were similar to those reported in international studies, further studies are required to determine the effectiveness of infection control measures for CDI incidence.
In conclusion, our study showed a high CDI incidence rate in some critical areas such as ICUs and immunocompromised wards. Therefore, specific infection control precautions should be reinforced in these areas by extending the period of contact isolation precautions until patient discharge and enhancing environmental cleaning and medical equipment disinfection.
Acknowledgment
The authors gratefully acknowledge Editage (www.editage.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received October 30, 2023.
- Accepted January 4, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.