


Abstract
Lung cancer is a complicated and challenging disease and is one of the most common causes of cancer-related mortality worldwide. Within the lung microenvironment, specific cytokines, including the B cell activation factor (BAFF) and the A proliferation-inducing ligand (APRIL), are produce by various cells, notably airway epithelial cells, in response allergic inflammation or pulmonary infection. These cytokines play a critical role in maintaining local immune responses and fostering the survival of immune cells. The BAFF and APRIL system have been connected in a range of malignancies and have shown their potential in inducing drug resistance and promoting cancer progression. This review highlights recent studies on the involvement of BAFF and APRIL in various cancers, focusing mainly on their role in lung cancer, and discusses the possibility of these molecules in contributing to drug resistance and cancer progression following pulmonary infection. We suggest consideration the targeting BAFF and APRIL or their respective receptors as promising novel therapies for effective treatment of lung cancer, especially post pulmonary infection. However, it remains important to conduct further investigations to fully elucidate the precise mechanisms underlying how the BAFF and APRIL systems enhance cancer survival and drug resistance subsequent pulmonary infections.
Despite advancements in diagnosis and treatment, patients with lung cancer still have a poor prognosis, making it one of the leading cause of cancer-related mortality globally.1 According to the global burden of disease study, lung cancer is the second most common cancer worldwide, with over 2.2 million new cases and approximately 1.8 million deaths by 2020.2 Lung cancer develops once cells in the lungs proliferate abnormally, which can be caused by a variety of factors, such as smoking, breathing contaminated air, and genetic abnormalities.3 The lung cancer is divided into 2 major types, including small cell lung cancer (SCLC) and non-small cell lung cancer (NSCLC).4 Non-small cell lung cancer is the most frequent kind of lung cancer, causing almost (85%) of all occurrences, whereas SCLC has a low incidence, reaching 15% of all cases.4 The possibilities for lung cancer therapy are determined by the stage and type of cancer along with the patient’s overall health.4 Non-small cell lung cancer is commonly treated with surgery, radiation therapy, and chemotherapy, whereas SCLC is typically treated with radiation therapy and chemotherapy.4 The pulmonary microenvironment plays a crucial role in the onset and progression of cancer, in addition to the emergence of resistance to therapies. The tumor microenvironment consists of a complex network of tumor cells that have interactions with stromal and immune cells.5 This interaction has the potential to influence the behavior of cancer cells, such as their viability and resistance to chemotherapy.5 Recently, targeted treatments and immunotherapies for lung cancer have shown promising results clinical trials, emphasizing the critical need to identify novel strategies for treating the lung cancer.6 Higher levels of both B cell activation factor (BAFF) and the A proliferation-inducing ligand (APRIL), in addition to their corresponding receptors, have been documented in several types of malignancies. These elevated levels have been observed to have a positive association with the severity both the disease and the response to medical treatments.7 However, a few studies have examined the involvement of BAFF and APRIL, along with their corresponding receptors in lung cancer. In addition, we and others have reported that BAFF and APRIL were expressed following viral or bacterial pulmonary infection.8-11 Ultimately, this review summarizes the fundamental roles of BAFF/APRIL in cancer, especially lung cancer, and discusses the potential of targeting of BAFF/APRIL or their correspondence receptors in lung cancer following pulmonary infection to prevent cancer survival and drug resistance.
Modulation of host immune response by lung cancer
A key hallmark of lung cancer is its ability to escape from the immune system, which is important for tumor progression and treatment resistance.12 The lung cancer microenvironment, which interacts with tumour cells and affect their behavior, include 4 major aspects, including inflammation, angiogenesis, immune response, and extracellular matrix proteins. Furthermore, chronic lung inflammation can promote lung cancer initiation and progression through DNA damage, oxidative stress, angiogenesis, and immune evasion, and inflammatory cells such as macrophages, neutrophils, mast cells can produce cytokines, chemokines, growth factors, reactive oxygen, which may result in enhancing tumor growth and expansion.13 In addition, angiogenesis, or the formation of new blood vessels, is necessary for tumor survival and metastasis. Lung cancer cells can secrete pro-angiogenic factors, such as vascular endothelial growth factor (VEGF), fibroblast growth factor (FGF), and platelet-derived growth factor (PDGF) that trigger new angiogenesis from existing angiogenesis.13,14 Angiogenesis can also promote tumor cell proliferation in the circulation.13 In addition, the microenvironment can increase cancer survival by modulating the immune system which can then evade immune surveillance by suppression molecules immune responses that inhibit the expression of immune cell function.14 The immune system can recognize and eliminate malignant cells through mechanisms involved antigen presentation, T cell activation, cytotoxicity induction, and cytokine generation. It has been shown that lung cancer cells are capable of altering the expression and function of several immune system components, such as the major histocompatibility complex (MHC), the interferon (IFN) pathway, immunological checkpoints, and microRNAs (miRNAs).15 These alterations improve cancer cells to avoid immune surveillance and initiate attacks. The suppression of T cell activation takes place when PD-1 receptors on the surfaces of T lymphocytes engage with lung carcinoma cells that exhibit an excessive expression of PD-L1.12 Moreover, lung cancer cells can modify extracellular matrix (ECM) proteins, by inducing matrix metalloproteinases (MMPs), cathepsins, and heparinases. This degrades ECM components and remodels the ECM, creating spaces and affecting pathways, adhesion molecules, and mechanical properties of tumour cells.14
Furthermore, cytokines play an important role in the tumour microenvironment, where they can have pro- or anti-tumour effects depending on the context.16 Some cytokines, such as interlukin (IL)-2, IL-12, and interferon gamma, may enhance the immune response against tumors by stimulating the activation and proliferation of T cells, NK cells, and macrophages. Other cytokines such as IL-6, IL-10, TGF-β, and VEGF, can induce tumour growth, angiogenesis, invasion, metastasis by inhibiting immune cell function or inducing immunosuppressive cells.16 Also, cytokines can also impact the responsiveness of lung cancer cells to various drugs by regulating their expression of drug transporters, drug-metabolizing enzymes, or drug targets.17 Thus, a deeper understanding of cytokines derived from the airway epithelial cells can provide survival signals to lung cancer cells is warranted to understand factors that support survival and drug resistance of lung cancer cells, especially following pulmonary infection.
The BAFF/APRIL system
B cell activation factor and APRIL cytokines belong to the tumour necrosis factor (TNF) family and both have vital and functional immunological roles in B-cell survival, proliferation, antibody production, and response to infection.18-20 The BAFF and APRIL system have been implicated in various diseases, as reviewed in previous studies.7,20-22 These molecules become functionally active through interactions with their receptors, including BAFF receptor (BAFF-r), B cells maturation antigen (BCMA) and, transmembrane activator and CAML interactor (TACI), which are expressed on B cells and other cell types.23 In addition, the expression of these cytokines is controlled by a range of stimuli including cytokines, growth hormones, and microbial products.24 B cell activation factor-receptor is unique receptor for BAFF, while BAFF shares 2 receptors: TACI and BCMA, and APRIL can bind strongly with BCMA and TACI but not with BAFF-r.21 These 2 molecules can trigger signalling pathways, including nuclear factor kappa-light-enhancer of activated B cells (NF-kB) and the mitogen-activated protein kinase pathway (MAPK), which regulate the balance and expression of apoptotic genes in B cells. This can lead to the prevention of cell death and promotion of cell division; therefore, they can promote B cell survival and growth.18
Expression of BAFF/APRIL in cancers
B cell activation factor and APRIL have recently emerged as potential contributors to both of hematological and non-hematological cancer development and resistance to treatment.7 Consequently, increased understanding to the role of these cytokines and their associated receptors in cancer is critical. Notably, BAFF and APRIL have been involved in the progression of B cell malignancies, including their role in the expansion of primary central nervous system lymphoma (CNS).25,26 In addition, it has been shown that APRIL has an essential functional role in supporting chronic lymphoblastic leukaemia (CLL) survival and interfering with APRIL and TACI can be used as promising approach to treat CLL disease.27 Additionally, BAFF and APRIL have been found to induce pluripotency genes like KLF4 and NANOG, thereby enhancing breast cancer cell stemness and migration.28
Furthermore, higher BAFF, APRIL levels, and their respective receptors have been observed in various malignancies, including CLL, brain cancer, hepatocellular carcinoma, skin cancer, colorectal cancer, breast cancer, and multiple myeloma (MM). These increased levels are liked with disease progression and therapy efficacy, as they augment the viability, proliferation, and invasiveness of cancer cells.7,28 Notably, local androgens in breast cancer amplify APRIL expression, fostering the transformation cells into stem cells and potentially leading to resistance to aromatase inhibitors.28 Additionally, increased levels of APRIL have been observed in breast cancer cells and patients, particularly in response to androgens, which promote APRIL transcription and tumour cell stemness, potently leading to therapeutic resistance in patients receiving aromatase inhibitors.29 Furthermore, BAFF and APRIL, along with their receptor genes, have been found to be expressed in MM cell lines, and elevated levels of these cytokines are correlated with poor outcomes and disease progression, promoting MM cells proliferation and survival.30
In addition, it has been shown that leukaemia cells cultivated in vitro exhibited higher viability and survival when exposed to the cytokines BAFF and APRIL.31 Moreover, it has been observed that CCL cells resist apoptosis through self-stimulating and external signalling pathways, including BAFF and APRIL, which can activate both the standard and alternative NF-kB pathways.23,32 Blocking of BAFF and APRIL or their receptors, as well as a decrease in their cleavage, have been shown to enhance CLL apoptosis, suggesting their potential as therapeutic targets.23,33
The triggering of the conventional and non-canonical NF-B pathways by BAFF and APRIL has been linked to treatment resistance and reduced apoptosis in CLL cells.34,35 Additionally, the serum samples from patients with CLL exhibited the presence of BAFF and APRIL proteins, whereas both of these molecules were not found in the serum of healthy individuals.23 The persistence of the microenvironment of CLL cells has been attributed to stromal cells that exhibit the cytokines APRIL, BAFF, and CD40L; this phenomenon contributes to resistance to treatment and enhanced survival.36
These findings underscore the potential of targeting the BAFF and APRIL signalling pathways to improve CLL treatment outcomes and facilitate precision medicine. B cell activation factor and APRIL have also been linked with drug resistance in cancer cells. For instance, acute myeloid leukemic (AML) blasts treated with BAFF and APRIL showed enhanced survival rates and reduced sensitivity to apoptotic inducers.37
Implications of BAFF/APRIL System in lung drug resistance post pulmonary infection
Earlier studies have demonstrated that both BAFF and APRIL cytokines promote normal and malignant B cell development.23 However, the specific immunological functions of BAFF and APRIL, along with their signalling receptors in lung cancer, remains poorly understood. Limited studies have been conducted on the role of these molecules in lung cancer. For instance, it has been observed that lung cancer cell lines, such as A549 and H2030, expresses BAFF, APRIL, as well as their correspondence receptors, including BAFF-r and TACI, but not BCMA. Notably, the addition of BAFF or APRIL did not appear to influence cancer progression and invasiveness.38
Furthermore, previous studies have shown that increased APRIL activity leads to the co-expression of APRIL and its receptors, which in turn increases self-stimulated tumour cell growth. Specifically, in A549 cells, increased APRIL activity induces extracellular signal-regulated kinase pathway (ERK1/2) phosphorylation, indicating the involvement of the ERK1/2 pathway, which stimulates the MAPKs pathway.
The upregulation of MAPKs in NSCLC plays a crucial role in promoting cancer cell survival and growth.39-41 Additionally, higher levels of APRIL and its respective, including BCMA, and TACI mRNA and proteins have been observed in NSCLC in comparison to normal tissues, and their presence were associated with lung cancer progression and poor outcomes in the clinical settings.42 Activation of APRIL pathway has been found to sustain MAPK signalling, potentially promoting tumour development. Inhibition of BCMA and TACI using siRNA has resulted in a reduction of APRIL-driven ERK1/2 activation in lung cancer cells, suggesting that they may enhance the cellular response to APRIL.42 The same group also discovered that APRIL and its receptors are highly expressed patient samples of NSCLC as well as in cell lines. April has the ability to increase tumour expansion, migration, and dissemination in A549 and H1299 cells via TACI and BCMA signalling. Furthermore, the activation of ERK1/2 was mediated by TACI not BCMA in A549 and H1299, underscoring the potential of APRIL as a prognostic biomarker and its associated signalling pathway as a therapeutic target in NSCLC.43 Additionally, one of the significant challenges in lung cancer treatment is the development of drug resistance.44 Various mechanisms of drug resistance have been identified as significant obstacles in the therapy of lung cancer.45 Inflammatory responses within the tumor microenvironment (TME) have been observed to play a significant role in facilitating the initiation, proliferation, and progression of tumors during their stages of development.46 Various mediators, which are either secreted by tumor cells or provided by cells infiltrating the TME, play a significant role in complex relationships that occur during inflammation. These interactions have various impacts on processes such as cellular differentiation, activation, performance, as well as cell survival and apoptosis.46 Therefore, the strategic approach of addressing tumor-associated inflammation holds promise as a viable strategy for combating cancer.47
Inhibiting BAFF and APRIL or their receptors has emerged as a promising therapeutic method for cancer and related diseases. B cell activation factor and APRIL have been linked to B-CLL cell resistance to apoptosis.23 Inhibiting BAFF and APRIL interactions with their receptors has been proposed as a treatment strategy for patients suffering from autoimmune rheumatoid diseases.48 Furthermore, neutralization of BAFF and APRIL by soluble decoy receptors such as TACI and BCMA may reduce the proliferation of malignant B cells in non-Hodgkin lymphoma (NHL) patient.49 Targeting BAFF and APRIL has also been investigated in the context of systemic lupus erythematosus (SLE) and other antibody-associated illnesses. In vitro investigations have demonstrated that TACI-Ig and BCMA-Ig can inhibit BAFF/APRIL heteromers, implying that dual inhibition of BAFF/APRIL by TACI-Ig may be an effective way to block these heteromers in autoimmune disorders.48 Furthermore, suppression of BAFF has been found in mouse lupus models to delay disease development, highlighting its potential therapeutic effectiveness in SLE.50 Overall, inhibiting BAFF and APRIL or their receptors offers promise as a cancer and associated disease therapy strategy. It may be possible to impair the survival and proliferation of B cells, which are frequently dysregulated in these situations, by targeting these substances. More study is needed to completely understand the processes underlying BAFF and APRIL’s roles in disease development and to produce clinically effective inhibitors.
Consequently, there is an urgent necessity to gain a deeper understanding of how cytokines derived from the airways or tumour microenvironment could enhance lung cancer survival and drug resistance. We recently reported that BAFF and APRIL cytokines are expressed in lung disorders in response to allergens, such as allergic asthma or respiratory infections.20
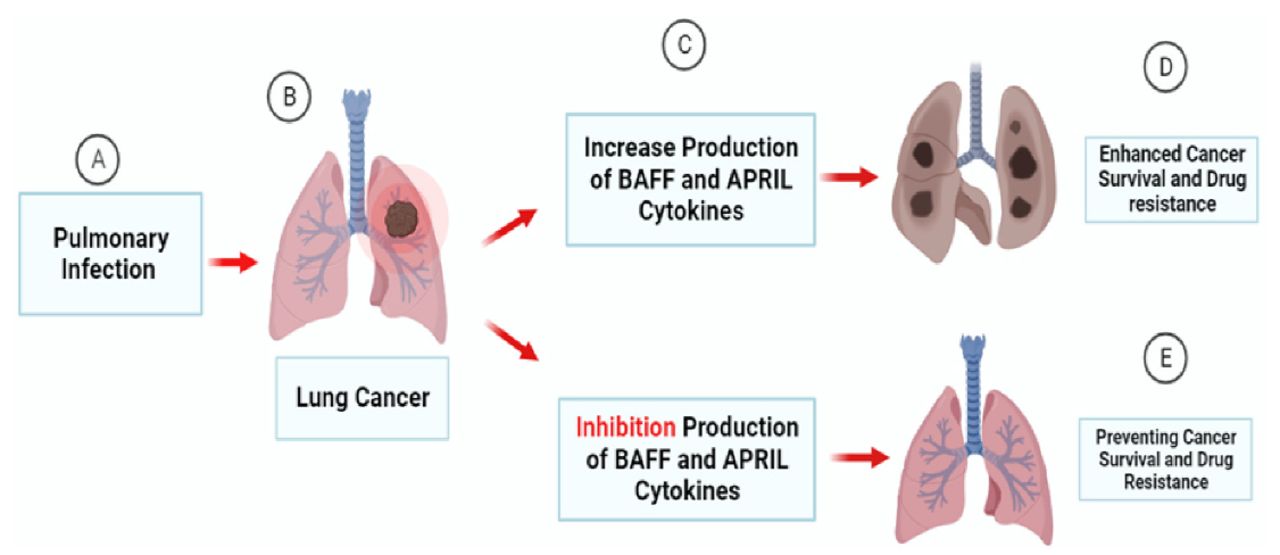
Moreover, we previously reported that BAFF and APRIL are expressed following respiratory syncytial virus (RSV) infection in both, in vivo and in vitro, studies in human and murine models and might enhance the adaptive immune response in the airways.8-10. These cytokines play a pivotal role in facilitating B-cell functions, including survival, differentiation, antibody production, and response to infection.51,52 Furthermore, bacterial infections, such mycobacterium tuberculosis (M. tuberculosis) infection have been reported to produce significant levels of BAFF and APRIL and have been linked to the severity of the infection.53 In addition, elevated levels of BAFF in both the lungs of individuals with cystic fibrosis and mice have been observed after Pseudomonas aeruginosa infection.11 Therefore, the BAFF/APRIL system is potentially significant in regulating the host reaction to microbial infection in the airways. Considering the increased expression of BAFF and APRIL in patients with lung cancer following pulmonary infection, it is possible that this may contribute to enhance cancer survival and drug resistance. Consequently, targeting the BAFF-APRIL signalling pathway could potentially improve lung cancer treatment and prevent the worsening of disease outcomes (Figure 1).

- The Role of BAFF and APRIL in Supporting Lung Cancer Survival and Drug Resistance: Respiratory infections such as viruses and bacteria can lead to an increase in local production of BAFF and APRIL cytokines to combat infections in lung cancer patients (A-B). The interaction of BAFF and APRIL cytokines with their unique receptors can lead to trigger signalling pathways, including NF-kB, ERK1/2, and the MAPKs pathways, which regulate the balance and expression of apoptotic genes. This can lead to the prevention of cell death and promotion of cell division; therefore, they can promote cells survival and growth. However, increased production of theses cytokines may also promote the survival of lung cancer cells (C), augment their drug resistance, inhibit apoptosis, and thus worsen the disease outcomes (D). Inhibiting the production of BAFF and APRIL may help prevent cancer survival and drug resistance (E).
Conclusion and future perspective
Lung cancer remains a critical international health challenge and is one of the common causes of death globally. It often responds poorly to treatment due to medication resistance and tumour heterogeneity. Thus, it is important to fully comprehend the mechanisms underlying medication resistance in lung cancer in order to design successful treatment strategies. Cytokines BAFF and APRIL play important roles in cancer development. These cytokines are produced by many cells, including airway epithelial cells, especially during infections, which can enhance tumour growth and metastasis and resist apoptosis and chemotherapy. In addition, over production of BAFF and APRIL cytokines have been linked in the progression of other diseases such as allergy and autoimmunity, and targeting these molecules or their receptors has improved outcomes in these conditions. Therefore, targeting BAFF, APRIL, and their receptor signalling pathways may be a potential strategy for lung cancer treatment especially following pulmonary infections. However, further researches are warranted to elucidate the molecular processes and signalling pathways of these cytokines in lung cancer cells, and their interplay with other factors and immune cells within the pulmonary microenvironment.
Acknowledgment
I would like to the thank the Deanship of Scientific Research at Majmaah University of supporting this study under project number (R-2024-973). I would like to thank Essay Doctor Academic Proofreading (www,academicproofreading.co.uk) for the English language editing.
Footnotes
Disclosure. This study was funded by the Deanship of Scientific Research at Majmaah University, Majmaah, Kingdom of Saudi Arabia. Project Number: R-2024-973
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.