


Abstract
Objectives: To assess the impact of changes in sinus aeration on dose variation in nasopharyngeal cases using a single beam with various field sizes and real patient computed tomography (CT) images.
Methods: The calculations were carried out on a computer equipped with an Intel Xeon (R) Gold 5118 processor operating at 2.30 GHz in 2022 at Taibah University, Al Madinah Al Munawwarah for a retrospective nasopharyngeal case. At the patient level, the impact on dose distribution was examined for different field sizes by comparing the percentage depth dose. The dose discrepancy was evaluated by comparing the dose delivered without considering the anatomical changes observed in the initial fraction to the dose adjusted to account for these changes using a 2D gamma analysis. With a criterion of 1% dose difference and 1 mm distance to agreement, the gamma level for analysis was set at 95%.
Results: The study findings indicated that the observed effect diminished by approximately 50% for both 5 cm x 5 cm and 10 cm x 10 cm field sizes compared to the 3 cm x 3 cm size, where there was an overlap between the planning target volume and sinusitis.
Conclusion: The study concluded that the impact of dose discrepancy was more pronounced in smaller field sizes.
The human head is composed of diverse tissues and cavities, making it a heterogeneous region. From a radiation dosimetry standpoint, this heterogeneity contributes to uncertainties and has an impact on dose distribution.1 Any alteration in tissue composition, such as sinusitis where the sinuses are filled with fluid instead of air, can result in incorrect target coverage and introduce significant uncertainties in dose calculation. This is due to the distinct physical and radiologic properties of each tissue.2 It is essential to recognize the influence of tissue property changes caused by sinusitis and, if necessary, consider the option of replanning the radiotherapy treatment. By doing so, we can enhance the therapeutic benefits of radiotherapy.
Radiotherapy is widely utilized in cancer treatment, it is included in the treatment plans of nearly half of individuals diagnosed with cancer. Intensity-modulated radiation therapy (IMRT), an advanced type of radiation therapy, has significantly improved long-term outcomes for head and neck patients, leading to a notable enhancement in their post-treatment quality of life. This achievement has placed IMRT in the spotlight.3 Despite these positive advancements, radiation treatment can induce localized changes and side effects that may impact dose distribution and ultimately affect treatment success.4 One such side effect caused by radiation is sinus inflammation, medically referred to as sinusitis. In this condition, the sinuses are filled with fluid instead of air.5 This alteration can have dosimetric implications.
To address this issue, dosimetry based on electronic portal imaging devices (EPIDs) can be employed to monitor the dose and detect any deviations between the planned dose and the delivered dose.6 However, the presence of heterogeneity errors and anatomical changes presents a challenging obstacle for pre-treatment verification.7 Consequently, it is highly recommended to perform patient-specific verification during the course of treatment to ensure accurate dose delivery.
This study aims to assess the impact of changes in sinus aeration on dose variation in nasopharyngeal cases using a single beam with various field sizes and real patient computed tomography (CT) images. The researchers utilized the latest version of EGSnrc (Electron Gamma Shower developed by the National Research Council) user codes in this study. This software serves as a toolkit for conducting Monte Carlo (MC) simulations, specifically designed for simulating the transport of ionizing radiation through matter.
Methods
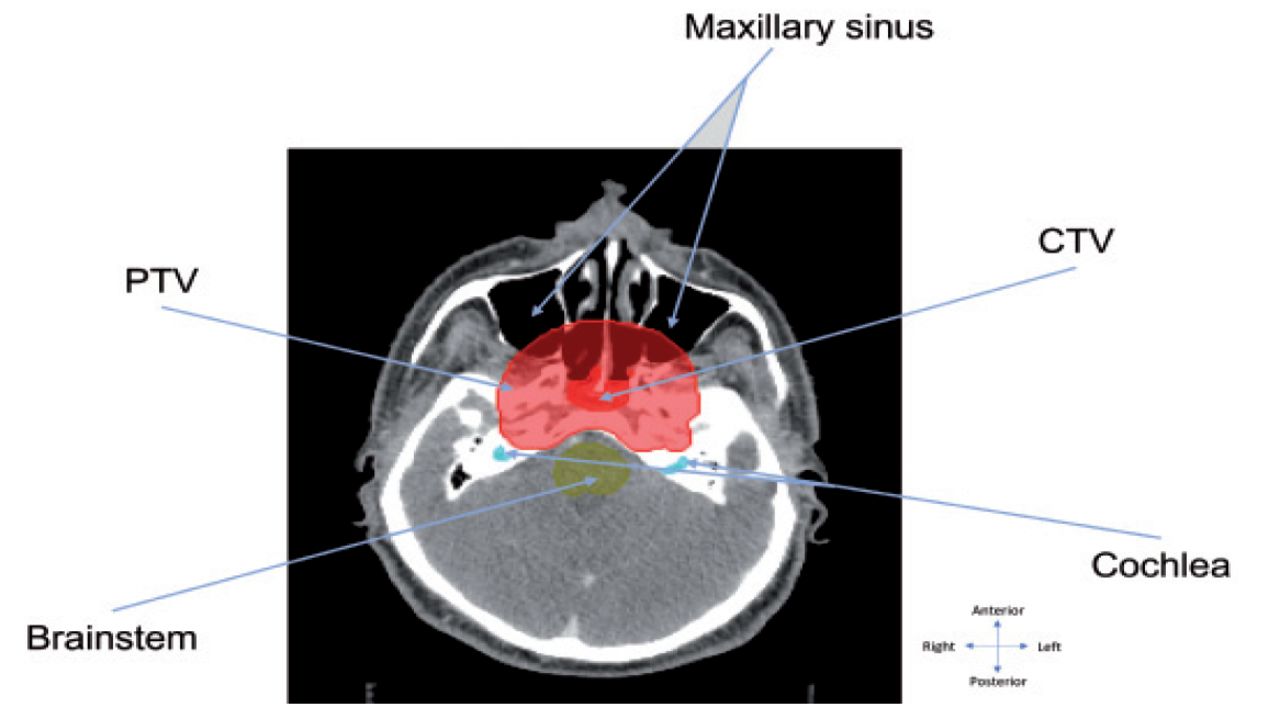
In this study, a case of IMRT Nasopharyngeal was chosen to investigate the impact of sinusitis on dose distribution by replacing the air within the sinus cavity with fluid. To achieve this, the anterior beam was specifically selected to ensure that the radiation beam passed through the maxillary sinuses (Figure 1). The process involved reading the digital imaging and communications in medicine (DICOM) files using MATLAB® and identifying the slices that contained the maxillary sinus. Subsequently, the pixel values corresponding to the air within the sinus were modified to represent fluid. This process was repeated for all relevant slices in the CT images. No ethical approval was required for this study.

- The positioning of the maxillary sinus in relation to planning target volume (PTV), clinical target volume (CTV) and organs at risk.
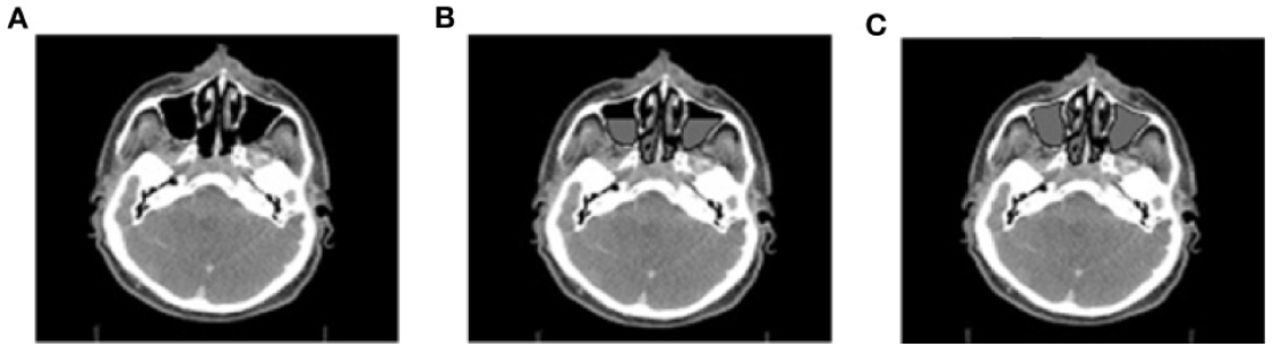
In the final stage of the study, several scenarios of real patient-based phantoms were generated to conduct the experiment. The focus was on 2 specific scenarios: scenario (b) and scenario (c), which involved deformed phantoms b and c, as illustrated in Figure 2. Scenario (b) represented a half-filled sinusitis condition, while scenario (c) represented a fully filled sinusitis condition. These scenarios were compared against a reference model, referred to as scenario (a), which corresponded to the original phantom without sinusitis. To ensure compatibility with the BEAMnrc user code, the phantoms were converted to a specific format using the CTCREATE tool distributed with the EGSnrc software. The voxel dimensions of the phantoms were set to 0.25 cm x 0.25 cm x 0.25 cm. This voxel size selection aimed to strike a balance between resolution, simulation speed, and statistical uncertainty.
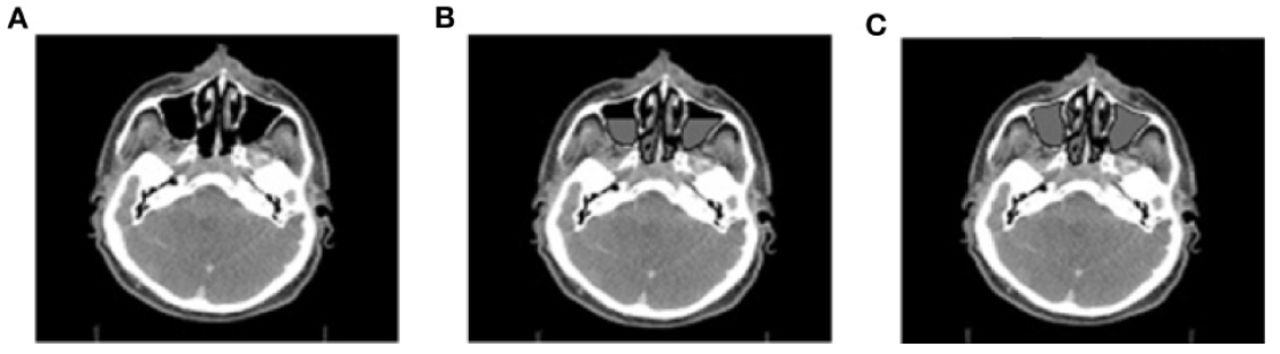
- Different scenarios of sinusitis A) the original CT, B) modified phantom for experiment 1 (half water-filled sinuses) referred to as scenario b, C) the scenario c for experiment 2 (fully water-filled sinuses).
To define the boundaries of the patient, including the location of the planning target volume (PTV) and the maxillary sinuses on the new phantom, Equation (1) was utilized.
 (1)
(1)Psim represents the new pixel position in centimeters (cm), while PCT denotes the pixel position on the y-axis in cm on the CT image. LengthCT refers to the length of the y-axis in the CT image, and lengthsim corresponds to the length of the y-axis in the new image.
Calculating the position on the y-axis is crucial because the percentage depth dose (PDD) was extracted from the y-axis of the axial CT image. It is important to note that the same equation can also be used to determine the new pixel position on the x-axis.
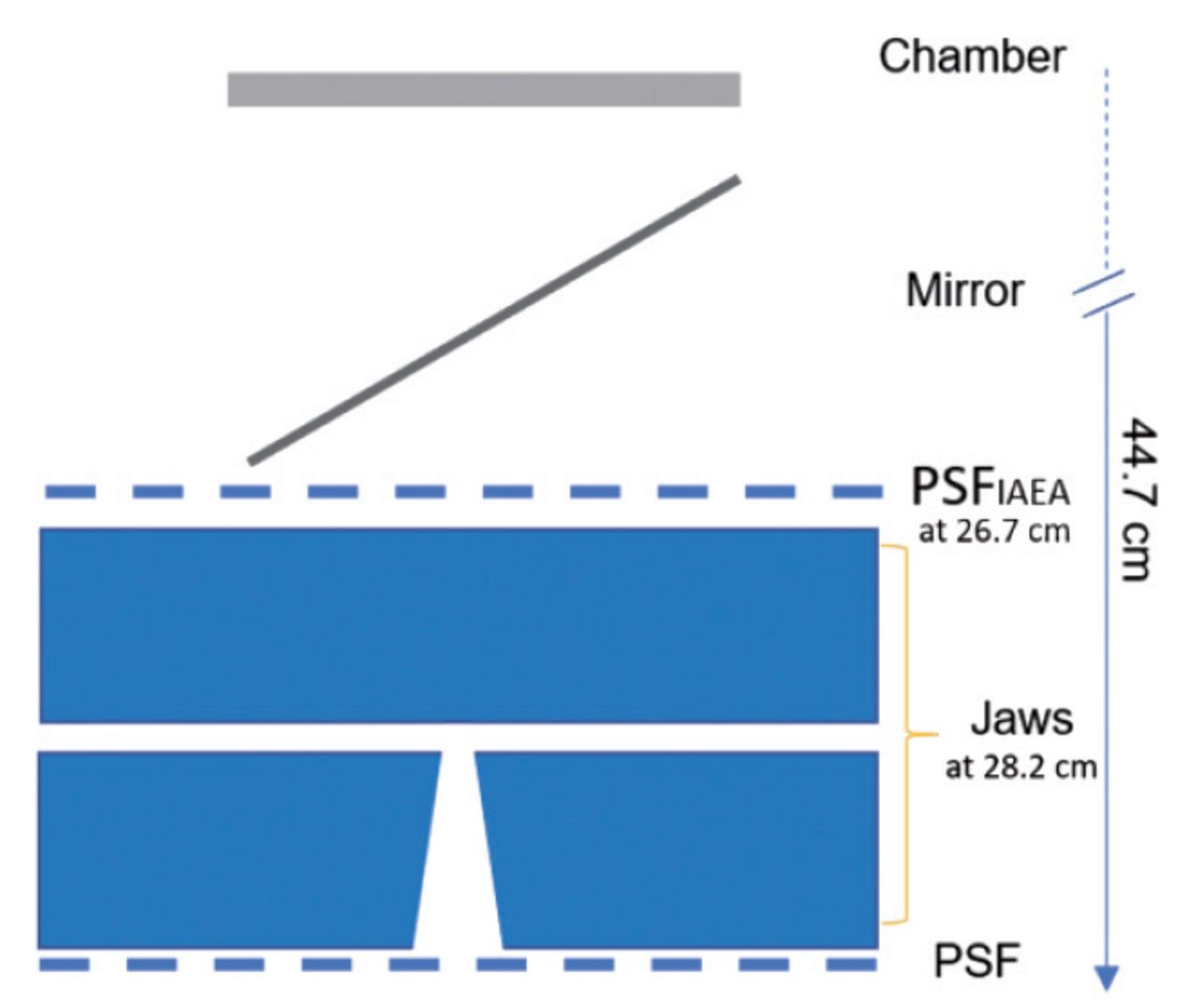
The treatment head for 6 MV was simulated using the international atomic energy agency (IAEA) phase-space files (PSFs) specifically designed for the TrueBeam Varian linac. This simulation was performed using BEAMnrc, which is one of the EGSnrc user codes. The treatment head includes various components, such as an ion chamber, mirror, jaws, and dynamic multi-leaf collimators (MLC), as depicted in Figure 3. The geometry of each component was approximately defined in the simulation.

- The linear accelerator treatment head.
The dose calculation was performed using DOSXYZnrc, an EGSnrc user code, on voxelized phantoms. To ensure compatibility, the coordinate system of the DICOM files was converted to the coordinate system of DOSXYZnrc by redefining the gantry, couch, and collimator angles. Several variance reduction techniques were implemented to reduce the simulation time while maintaining efficiency. Energy cutoffs were applied to electrons and photons, with a cutoff of 0.7 MV for electrons and 0.01 MV for photons. This choice was made to account for the long-distance travel and interaction of low-energy photons.6,7 The dose simulation involved scoring the 4D PSFIAEA at the particle exit from the phantom. The calculations were executed on a computer equipped with an Intel Xeon (R) Gold 5118 processor operating at 2.30 GHz.
The evaluation method used in this study was the gamma index with a specified gamma angle. This method is widely regarded as the gold standard for comparison in radiotherapy. The main parameters of the gamma index are the dose percentage and the distance to agreement (DTA) in millimeters. The gamma angle helps determine which parameter has a greater influence on the gamma result.8 To assess the impact of the changes made to the phantom, the dose of the modified phantom was compared to the dose of the original phantom at the patient level. This comparison was evaluated using gamma analysis with a criterion of 1% dose difference and 1 mm distance to agreement. A gamma level of 95% was used to determine the acceptability of the results.
Results
This study focuses on examining the impact of sinusitis on dose distribution in radiotherapy using real patient phantoms and considering different field sizes. The PDD is used as an indicator to detect dose discrepancies resulting from tissue inhomogeneity. In this study, a threshold of 95% has been defined as the reference level for acceptable error. Errors within the range of ±5% are considered minimal and inconsequential. This range has been established to strike a balance between avoiding undesirable outcomes associated with radiation treatment and ensuring that radiotherapy is administered with a reasonably high level of accuracy. It aims to maintain a level of precision without being excessively lenient or stringent.9
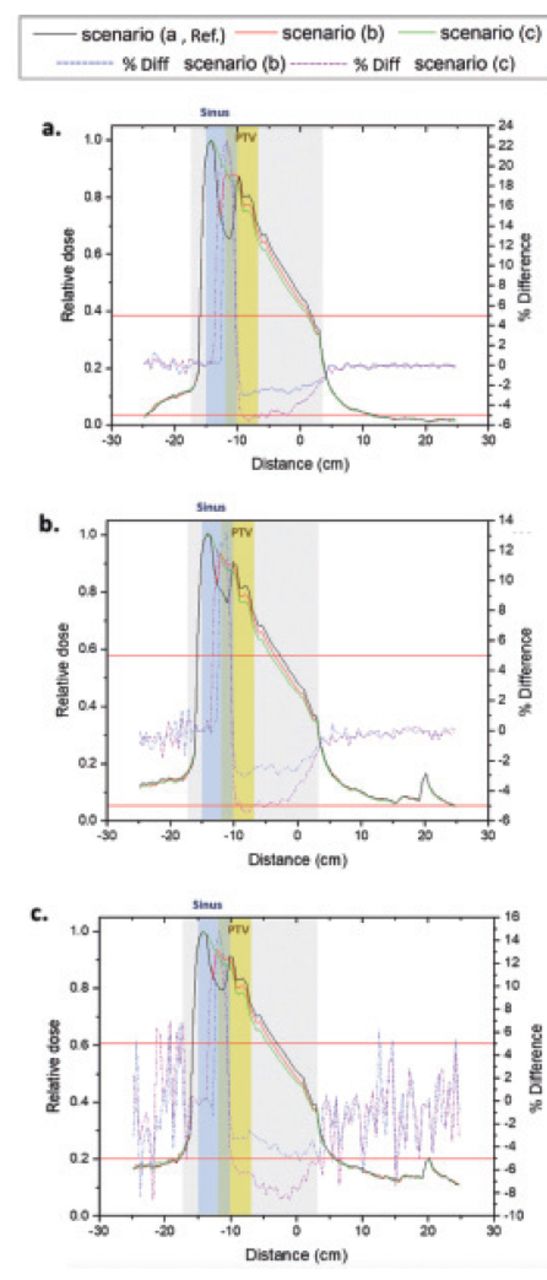
Table 1 presents numerical values obtained from Figure 4, which demonstrate the dose differences between the normal and deformed phantoms in terms of percentile change. It is important to note that in this specific patient, the planning target volume (PTV) overlaps with the maxillary sinus. As a result, the PTV dose difference is categorized into 2 regions: the dose difference during sinusitis and the dose difference after sinusitis.
- The averaged dose difference and 2D evaluating GPRs percentages for various field sizes within PTV.
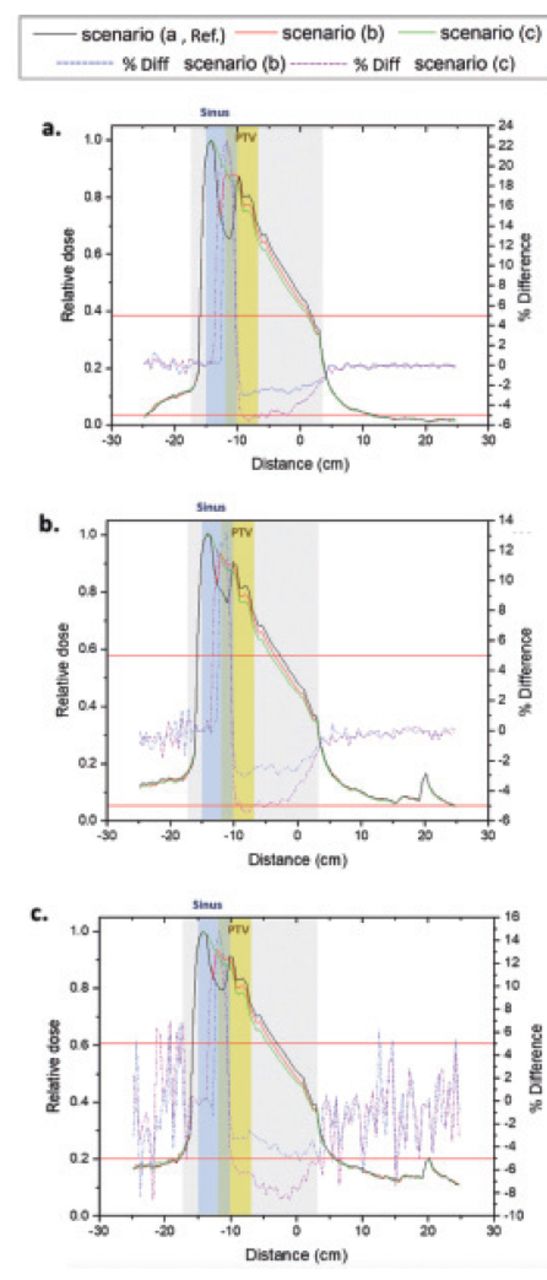
- The percentage depth dose in the phantom, ranging from -17 cm to 3 cm, are displayed in different scenarios: a) using a 3 cm x 3 cm field size, b) a 5 cm x 5 cm field size, and c) a 10 cm x 10 cm field size. The grey shaded area represents this range within the patient. The blue shaded area, spanning from -15 cm to -10 cm, corresponds to the sinuses, while the yellow shaded area, ranging from -12.5 cm to -7 cm, represents planning target volume.
In the region where the planning target volume (PTV) overlaps with sinusitis, the average dose difference decreases by nearly 50% when comparing the 5 cm x 5 cm and 10 cm x 10 cm scenarios to the 3 cm x 3 cm scenario. The impact of dose difference becomes more pronounced when the sinuses are completely filled with fluid. However, this effect diminishes as the field size increases. For example, in scenario (c) compared to scenario (b) at field sizes of 3 cm x 3 cm, 5 cm x 5 cm, and 10 cm x 10 cm, the dose differences are +3%/-2.46%, +0.40%/-2.32%, and +0.45%/-2.92%, respectively, in the areas corresponding to sinusitis/after sinusitis. The larger dose difference in the 10 cm x 10 cm field size compared to the 5 cm x 5 cm field size is attributed to increased scatter contribution and the larger coverage of both maxillary sinuses located on either side of the nose. As a result, sinusitis can potentially impact the distribution of radiation doses during radiotherapy. The presence of sinusitis during the course of radiotherapy may introduce challenges in the accurate delivery of radiation to the intended target areas, especially when the sinuses are fully filled with fluid or when the PTV is overlapped with sinusitis, as shown in Table 1 and Figure 4.
In all field sizes and scenarios, the dose difference within the planning target volume exceeded the predefined percentage difference threshold of ±5% in the sinusitis area. However, for scenario (b) and the after sinusitis area across all field sizes, the dose difference remained below the threshold, as indicated in Table 1. This implies that sinusitis that is half-filled has a lesser impact on dose distribution than sinusitis that is fully filled.
When evaluating gamma passing rates (GPRs), it is common to set the tolerance level at or above 95%. However, no discernible difference between the 2 scenarios is observed within the planning target volume.
Discussion
The impact of inhomogeneity on dose distribution has been previously investigated using various methods such as water phantoms or animal models like dogs, as shown in previous studies.10-12 The presence of inhomogeneities is a concern because x-rays interact differently with different materials, leading to variations in image contrast.13 In the case of sinuses, the air-filled spaces cause a reduction in dose due to the lower density of air compared to other tissues in the head. This underdosing effect is expected to decrease when the sinuses are filled with fluid.12
In the region where the planning target volume overlaps with sinusitis, the average dose difference decreases by approximately 50% when comparing field sizes of 5 cm x 5 cm and 10 cm x 10 cm to a 3 cm x 3 cm field size. The difference in dose is more significant in the 10 cm x 10 cm field size compared to the 5 cm x 5 cm field size. This can be attributed to the increased scatter contribution in the larger field size. Additionally, the 10 cm x 10 cm field size covers both maxillary sinuses on both sides of the nose, which results in a larger area being affected (such as, 2 maxillary sinuses). A research study carried out by Daly et al14 investigated the clinical outcomes of patients who underwent intensity-modulated radiation therapy (IMRT) for nasal cavity and paranasal sinus malignancies. The long-term results of the study revealed suboptimal outcomes, as patients experienced late complications. It is possible that these complications could be attributed to a failure to account for anatomical changes that occurred in the treated area during the course of treatment, leading to inadequate disease control.
In the context of volumetric-modulated arc therapy (VMAT), studies have reported that changes in the maxillary sinuses have minimal impact on the distribution of radiation dose within the tumor volume and do not result in significant dose differences in volumes of organs at risk (OARs).15 However, it is important to note that these changes can have a significant impact on the dose distribution when proton therapy beams are used.15
Table 1 reveals that the 10 cm x 10 cm field size exhibits the lowest gamma passing rates compared to the other two field sizes. This can be attributed to the fact that the 10 cm x 10 cm field size covers both sinuses, whereas the other two field sizes do not. However, to enhance the robustness of this study, it is imperative to increase the sample size.
In conclusion, by comparing the percentage depth dose in a phantom, the study revealed a correlation between sinusitis and the impact of field size. The findings indicated that the effect of sinusitis decreased slightly as the field size increased. Specifically, when examining the region where the planning target volume overlaps with sinusitis, the average difference decreased by nearly 50% for both scenarios when using a 5 cm x 5 cm or 10 cm x 10 cm field size compared to a 3 cm x 3 cm field size. These observations support the assertion that variations in volume, such as those caused by sinusitis, may have a more significant impact on smaller field sizes commonly used in intensity-modulated radiation therapy (IMRT) plans.
Acknowledgment
The authors would like to acknowledge ContentConcepts (www.contentconcepts.com) for the English language editing.
Footnotes
Disclosure. Author have no conflict of interests, and the work was not supported or funded by any drug company.
- Received July 19, 2023.
- Accepted January 7, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.