


Abstract
Although, from a therapeutic standpoint, breast cancer (BC) is considerably well-characterized, it still leaves puzzling spots. The Her-2+/PR+/ER+ BC can benefit from the mainstays of anticancer therapy and immunotherapy and overall have a better prognosis. Triple-negative BC, due to the concomitant absence of Her-2/PR/ER receptors, is more challenging and necessitates different strategies. It has been learned that the mainstay anti-BC therapies were initially designed to demolish as many cancer cells as they possibly could. However, the number of reports on the adverse effects of these mainstay therapies has recently been increasing. It underpins efforts to reshape such therapies into much better and safer forms over time. Moreover, some current findings on the molecular markers, which are target-potential, have also shifted the paradigm from radical-to-local-yet-precise-approach to meet the need for a therapy platform that is less cytotoxic to normal cells yet efficiently kills cancer cells.
Breast cancer (BC) is the most common cancer in women and accounts for 25% of all cancers.1 In 2020 alone, there were a total of 2.26 million new patients with BC, and this is projected to reach 3.2 million cases by 2050.2 Although the death toll dramatically reduces (which is good news) the global battle against BC has yet to be close to an end. Moreover, the rising emergence of early onset, where patients are diagnosed with cancer at the age range of 20-50 years old, is another challenge that requires substantial focus.3
Breast cancer is genetically and clinically heterogeneous. The classification of BC is generally based on the expression of major hormone receptors, namely estrogen (ER), progesterone (PR) and human epidermal factor (Her-2) which results in 4 subtypes of BC: luminal A, luminal B, Her-2 positive and triple negative BC (TNBC) with the last mentioned is the least case which accounts for only 12-17% of total BC. Triple negative BC is characterized by weak cellular expressions of PR, ER, and Her-2.4 Due to these deficiencies, TNBC is insensitive to endocrine therapy or Her-2-based treatment. Until now, treatments for TNBC have been poorly standardized.5 Therefore, it urges novel strategies for which scientists across the globe have put their efforts to bring significant improvement.
It is broadly evident that family history augments the risk factor of somebody to develop BC in their lifetime. Approximately 5-10% of BC cases are related with family history.6 A 16-year-long observation by Breast Cancer Surveillance Consortium (BCSC) Registries in some regions in the United States showed that the first degree family history was associated with increased risk of invasive BC of older women regardless a relative’s age at diagnosis.7 This supported a finding of a 20-year-earlier study, with Sweden cohort, where women with any first degree relative were observed to have association with a higher risk of BC compared to those who did not have such a history. In addition, women with benign breast disease were related to BC risk even without family history.8 Despite consistency of these findings over the years across observational cohorts, family history remains underused which might contribute, to some extent, to the high prevalence of BC.9
From there, it is imperative to take family history into account to help stratify the propensity of people to develop BC somewhere within their lifetime. A comprehension of this variable might direct us toward a more efficient prevention strategy. But one must understand that family history is not a standalone variable. There are various variables whose interactions determine affected patients’ responses toward cancer development (whether it progresses into a more aggressive phenotype) and the treatment they are suggested to opt for. This review discusses the major contributors to BC development which renders their potential to be employed to enrich the existing platforms. It is learned that every anti-BC therapy is like a double-edged sword. The clinicians should take these 2-sided impacts into account, and the patients should be aware of them prior to providing a clear preference for specific treatments. The adverse effects of mainstay anti-BC therapies have been recorded all these years, which leads to the evolvement of the respective therapy. This evolvement is marked by more integrated aspects to be evaluated. We have seen revolutionized strategies from radical to conserving surgery and from whole high dose to fractionated radiotherapy. We also witness that immunotherapy has become more diverse following many more novel findings on molecular signatures, which are seen to be promising targets for the therapy. Many of which have been the Food and Drug Administration (FDA)-approved, suggesting that they have been through rigorous tiers of clinical trials to assure safety as well as efficacy. This review also alludes to some crucial genetic landscapes and molecular mechanisms with which the existing anti-BC therapy platforms can be improved to benefit a much broader range of patients.
Risk factor assessment
Cancer risk is the sum of various factors, including genetic architecture, lifestyle, behavior, and environmental exposure. However, it is difficult to measure the magnitude of each factor unless this is translated into an in vitro or in vivo setting. Both settings enable the identification of genes that are broadly known to drive cancer initiation as well as progression, for instance, retinoblastoma tumor suppressor-1 (RB1) and PIK3CA.10
Retinoblastoma tumor suppressor-1 protein is a regulator of cellular proliferation. Its status provides crucial information regarding BC prognosis and therapeutic interventions. Up to date, RB1 has been shown to be a pivotal player in many cancers.11 The RB1 regulates the G1/S-phase cell cycle and mediates antiproliferative signaling through binding to the transcription factor family E2F, which leads to the attenuation of many genes that are necessitated for cell cycle progression.11,12 As to the regulation of RB1, RB1-inducible coiled-coil 1 (RB1CC1), also known as the focal adhesion kinase family-interacting protein of 200 kDa, was identified as an RB1 regulator that hikes up RB1 transcription. Rearrangement in the genetic architecture of RB1CC1 is deemed to play a substantial role in the tumorigenesis of BC.12 The nuclear expression of RB1CC1 was shown to elevate RB1 expression in an in-vivo setting of human BCs, which added more volume to the prognostication value of RB1.13 The RB1 is encoded by the RB1 gene, which is situated in the long arm of chromosome 13q14. The gene consists of 27 exons, which scattered over 180 kb.14 A single-copy loss of chromosome 13q is frequently observed in diverse types of cancer and implicates poor outcomes. Microscopic deletions of 13q14 or monosomy 13 were observed in approximately 20% of RB tumors whereas trisomy 1q and i (6p) were reported in a high percentage of tumors.15
It was discovered that the frequency of reduced RB1 gene copy number was lower in those with metastatic lesions as compared to that seen for non-matched primary BC. This seemed paradoxical because deletion of a tumor suppressor gene should favor tumor progression. However, this feature contradicted observations in prostate carcinoma, where RB1 loss of heterozygosity (LOH) was detected at a higher frequency in metastatic sites compared to primary sites.16 Not only is RB1 a pivotal risk factor for BC development and progression, but it is also indicated as a strong predictor for sensitivity toward radiotherapy (RT) and chemotherapy.17,18 This suggests that an assessment of RB1 might provide a more accurate picture of one’s susceptibility to BC, upon which the preventive actions are accurately based.
The PI3K pathway is the most common mutated pathway in BC. The mutations are frequently detected in the gene coding for the PI3K subunits p110α (PIK3CA) and p110β (PIK3CB), the PI3K regulatory subunit p85α (PIK3R1), and receptor tyrosine kinases (RTKs), such as human epidermal growth factor receptor Her-2 (ERBB2) and fibroblast growth factor receptor (FGFR)-1.19 The PI3KCA alone encodes the catalytic α subunit of PI3K, referred to as PI3KCA. Its mutation occurs in 20-30% patients with BC.20 On the other hand, mutations of Akt serine/threonine kinase (AKT-1) are observed in up to 8% of BC. There have been mutational hotspots in the PI3KCA gene being in exon 20, exon 9, and exon 7, whereas mutational spots in Akt-1 lie in exon 1 and exon 2.21
The prognostic effect of these mutations differs among BC histological subtypes, but it can be highlighted that PI3KCA is a powerful predictor for hormone recep-tor-positive BC. Particularly in Her-2-positive BC, PI3KCA mutations might pose an adverse impact on patients’ survival.19 Like that seen for RB1, activation of the PI3K pathway induces anti-BC therapy resistance.22 Owing to that, PI3K pathway inhibitors, in combination with inhibitors of mitogen-activated extracellular signal-regulated kinase (MEK), Her-2, and ER, are currently under investigation. Randomized clinical trials are required to assess if the inhibition of PI3K is more beneficial compared to the standard targeted therapies alone.22
The ER and PR status are notable contributors to the clinical outlook of BC.23 In addition, Her-2 is integrated into ER and PR status, and jointly, ER, PR, and Her-2, determine the therapy platform for the affected patients. According to the presence of ER, PR, and Her-2, BC is categorized into 3 major types: I) ER+/PR+ but Her-2-negative; II) Her-2-positive; and III) TNBC, which concomitantly lacks of ER, PR and Her-2.5
The TNBC is prone to recur. Approximately 85% of patients with TNBC at stage I are likely to have a 5-year BC-specific-survival. But patients at the same stage but ER+/PR+/Her-2+ are reported to have a 99% chance of having a 5-year BC-specific-survival.24 With negative receptor status, one might question what is the best bet for patients with TNBC would be. Since TNBC does not have hormone receptors, hormonal therapy or trastuzumab-based targeted therapies are not preferred. Some patients indeed respond greatly to chemotherapeutic agents such as taxanes and anthracyclines that do not improve their prognosis. There have been targeted therapy platforms under investigation. Lovastatin and simvastatin, both are 3-hydroxy-3-methylglutaryl-coenzyme A reductase (HMG-CoAR) inhibitor (statin), which is more often used as antihyperlipidemic drugs as they display antiproliferative properties, have been demonstrated to target TNBC compared with that non-TNBC, suggesting that both are promising for TNBC management.25 However, this needs more investigation in clinical trials to acquire approval for use against TNBC.26 Chemotherapy is so far the treatment TNBC patients could benefit from but we have seen a significant move in constructing immunotherapy for TNBC, which we will discuss more in the subsection future direction in anti-BC therapy in this review.27,28
Common anticancer modalities
Surgery is one of the mainstay treatments in BC.29 Surgery options can be in the form of mastectomy or lumpectomy, where a decision is carried out by considering comorbidities, age, stage, grade, and size of the tumors.30 Mastectomy is opted for when RT is not possible due to physical disabilities and contraindications such as systemic lupus erythematous, and pregnancy. When multiple primary tumors are present, tumor-free margins are arduous to mark, but the proportion of tumor size in the breast is considerably large, mastectomy is deemed to be the most appropriate option.31
The surgical procedure has evolved rapidly in the last 2 decades. It is perceived as a gradual shift from total and radical removal of the breast toward partial or conserving surgery. The National Surgical Adjuvant Breast and Bowel Project (NSABP) B-04 trial reported that there was no difference in relapse-free survival, disease-free survival, distant-disease-free survival, as well as overall survival of those who have undergone mastectomy, lumpectomy (breast conserving surgery, BCS), or lumpectomy with radiation which suggests that lumpectomy may be a better procedure for surgery, particularly for patients with early-stage invasive BC.32 However, one should consider that BCS procedure might result in an unsatisfactory aesthetic due to the big excision. Therefore, the concept of oncoplastic breast surgery (OBS) emerged. In OBS, BC with negative histologic margins is resected, but at the same time, the contour of the breast is preserved.33 The procedure incorporates the principles of oncologic and reconstructive surgery by employing aesthetic-enhancing techniques to surmount tissue defects and optimize cosmesis from BC surgery.34
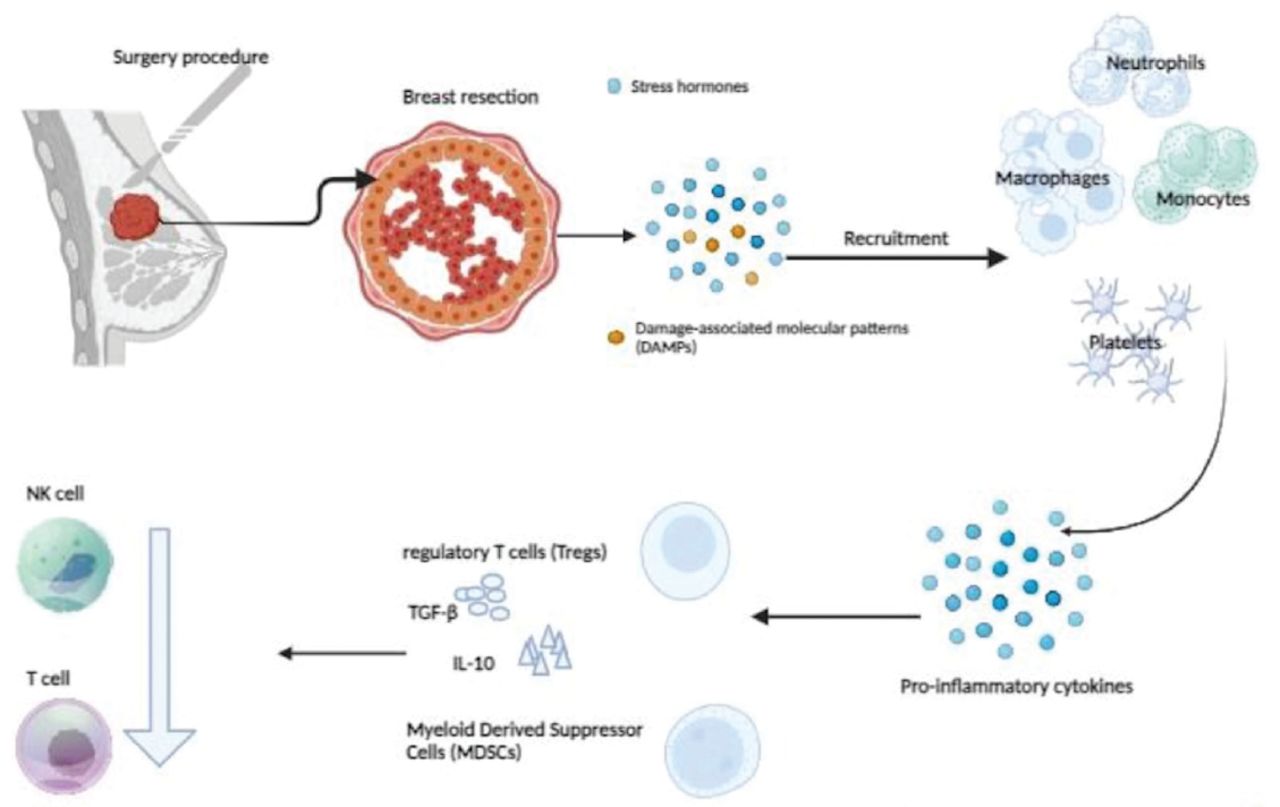
Despite being one of the mainstay anti-BC treatments, surgery is also reported to favor the expansion of immunosuppressive cell subsets, namely myeloid-derived suppressor cells (MDSCs). Surgery causes cellular stress, which is a recruitment and differentiation signal for MDSCs. The MDSCs carry tumor-promotive properties as they suppress natural killer (NK) cells and T-cells and expand regulatory T-cells (Tregs). The cytotoxicity of NK cells is, as well, largely attenuated through the release of catecholamine, glucocorticoid, and prostaglandin (hormones that are produced as a physiological response to stressful condition). Dysfunctional NK cells increase the chances of BC recurrence and metastases.35 The immunosuppressive mechanism of RT is shown in Figure 1.

- Surgery-mediated immunesupressive mechanisms.
As breast tissue is resected according to standard breast surgery procedures, danger-associated molecular patterns (DAMPs) and stress hormones such as catecholamine, glucocorticoid, and prostaglandin are released. Both signal for the recruitment of neutrophils, macrophages, monocytes, as well as platelets to the tumor microenvironment (TME). The TME, triggered by the surgery, remodels into an inflammatory state where pro-inflammatory cytokines such as IL-6, IL-8, and some chemokines such as CCL2 and CCL18 are markedly produced. These productions activate and direct the movement of 2 major immunosuppressive cell subsets being Tregs and MDSCs. Both secrete TGF-β and IL-10 which simultaneously downregulate NK cells and T-cells.35
Having grasped that surgery potentiates immunosuppression, one might question if the suppressive effect is long-lasting. An intriguing study by Ananth et al36 showed that tumor-associated antigen (TAA)-specific CD8+ T-cell (cytotoxic T-cells, CTLs)-immunity was profoundly suppressed after major surgery. They transplanted adoptive T-cells from surgically stressed vaccinated mice into naïve recipient mice, followed by a flank tumor challenge. It was observed that all mice that received T-cells from surgically stressed T-cell donors developed progressive flank tumors and died off. In contrast, those that were treated with adoptive T-cells from no-surgery-vaccinated mice showed 90% protection. Phenotypically, the TAA-specific CD8+ T-cells after major surgery produce less IFN-γ, TNF-α, and Granzyme B. This effect, however, was transient. Administration of IFN-γ recovered this defect.36 Since this study was carried out using animal models, more studies are required to clarify the involved immune cell subsets and validate this process in humans.
Radiation therapy (RT) is an integral part of the multidisciplinary management of BC. Nevertheless, it remains challenging. It changes rapidly following reports on the adverse effects it causes in some patients.37-41 The most commonly used RT to treat cancer is x-ray, which belongs to low-linear energy transfer (LET) radiation. Radiation induces a string of biological events, including ionization, free radical production, and chemical and biological reactions.42
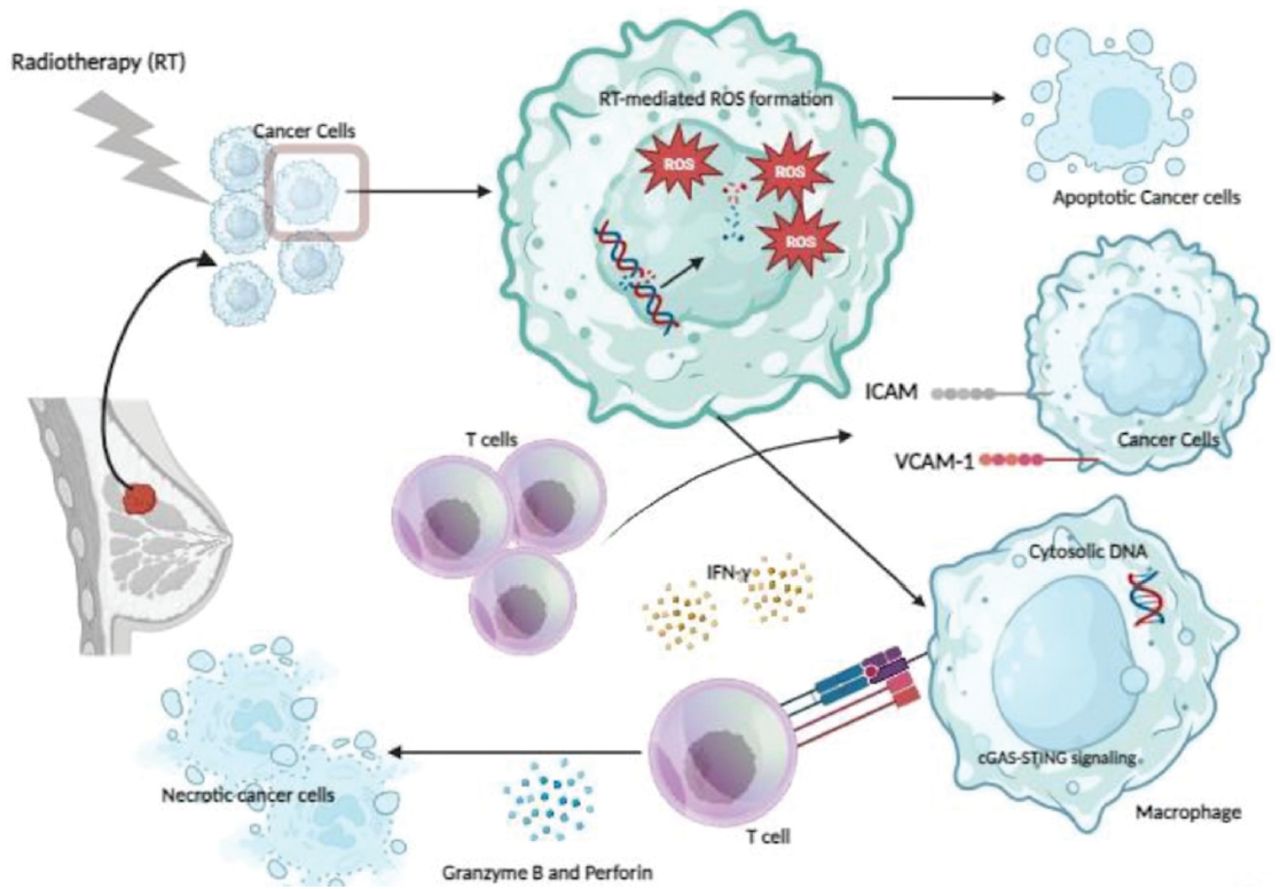
As cancer cells are irradiated, DNA double-strands and water molecules are broken. While fragmented DNA-strands lead to apoptosis, the water molecule breakage induces reactive oxygen species (ROS) formation. The ROS generates cytosolic DNA, which is sensed as cGAS. Subsequently, cGAS activates STING, which upregulates type-1 IFN, inflammatory interferon-stimulated (ISG) and senescence-associated secretory phenotype (SASP) genes. The IFN-γ is secreted by surveilling immune cells such as T-cells (mainly CD8+ cells), NK cells, and Th1 cells, which further enhance the expression of MHC I molecules on the surface of macrophages (representing antigen processing cells [APCs]) within which the tumor antigens are processed.43 On the other hand, irradiation increases VCAM-1 and ICAM on the surface of cancer cells, which will be sensed by T-cells to come closer and bind them. Upon binding, the tumor is rejected.44 The mechanism of RT stimulating the systemic immune response is shown in Figure 2.

- Radiotherapy-mediated immunomodulatory effects.
The RT is commonly applied post-surgery to reduce the risk of locoregional recurrence and to enhance overall survival. It comes with adverse consequences, unfortunately. After RT, significant decreases are observed in respiratory muscle strength, chest wall mobility, exercise capacity, and pulmonary function tests.45 Due to anatomical proximity, breast RT might also be toxic to the heart. According to the findings of the Breast Cancer Working Group of the German Society for Radiation Oncology (DEGRO), the risk of breast cancer-specific mortality and a patient’s cardiac risk factor must be individually considered in the context of radiation-induced cardiotoxicity.46
Notwithstanding the success stories in common types of BC, RT does not seem to provide an excellent outcome in TNBC.17 Whether TNBC is insensitive to RT or this radiation resistance is associated with multi-gene-target overexpression or deletion of the cancer cells remains impugnable to date.47 The good news is that a study carried out more than a decade ago demonstrated that deletion and overexpression of various gene targets in TNBC activates the PI3K/Akt pathway, ultimately causing RT insensitivity. To inactivate this, blocking the conduction pathway involved in these molecules or receptors is suggested.48
Tailoring both success stories and drawbacks that have been recorded all these years is one critical point that has aspired to the rapid evolvement of RT in the BC regiment realm. This is not only in the context of RT as monotherapy but also in combination with other platforms, mainly immunotherapy, which is hitherto deemed to provide more advantages for BC across histological subtypes. The RT has redefined its clinical implementation in the form of increased dose per fraction, shortened duration of RT course, and lowering toxicity, which in general result in modernized paradigms that have been broadly accepted as the gold standard of care and, further, paves the way to significant improvement of RT.49
Future directions of anti breast cancer therapy
Each platform in anti-BC therapy has exhibited substantial advancement. Adjuvant chemotherapy was widely demonstrated to be efficacious in targeting ER and Her-2 in the early and advanced stages, but it could not do much for TNBC. Relapse after halting endocrine therapy is a common event in hormone receptor-positive patients who receive endocrine therapy, which reflect tumor dormancy that is not completely overcome by the therapy.50 However, decades of massive work on enhancing new therapy platforms seem to have yielded promising results, which is a gain for those who are affected by the diseases.
In 2021, olympiA-PARP inhibitor (PARPi) Olaparib, which had already commenced phase 3 of the clinical trials, was reported to be successful at elevating invasive disease-free survival (IDFS) significantly. In addition, Olaparib improved distant DFS (DDFS).50 Adverse effects were observed beyond 1% in those with grade 3, which manifested as anemia, neutropenia, leukopenia, fatigue, and lymphocytopenia.51 As monotherapy, Olaparib prolong median progression-free survival and reduces the risk of disease progression in patients with a germline BRCA mutation and Her-2-negative metastatic BC.52
The substantial progression on immunotherapy is summarized in Table 1.
- Recent anti-breast cancer immunotherapy platforms commencing clinical trials.
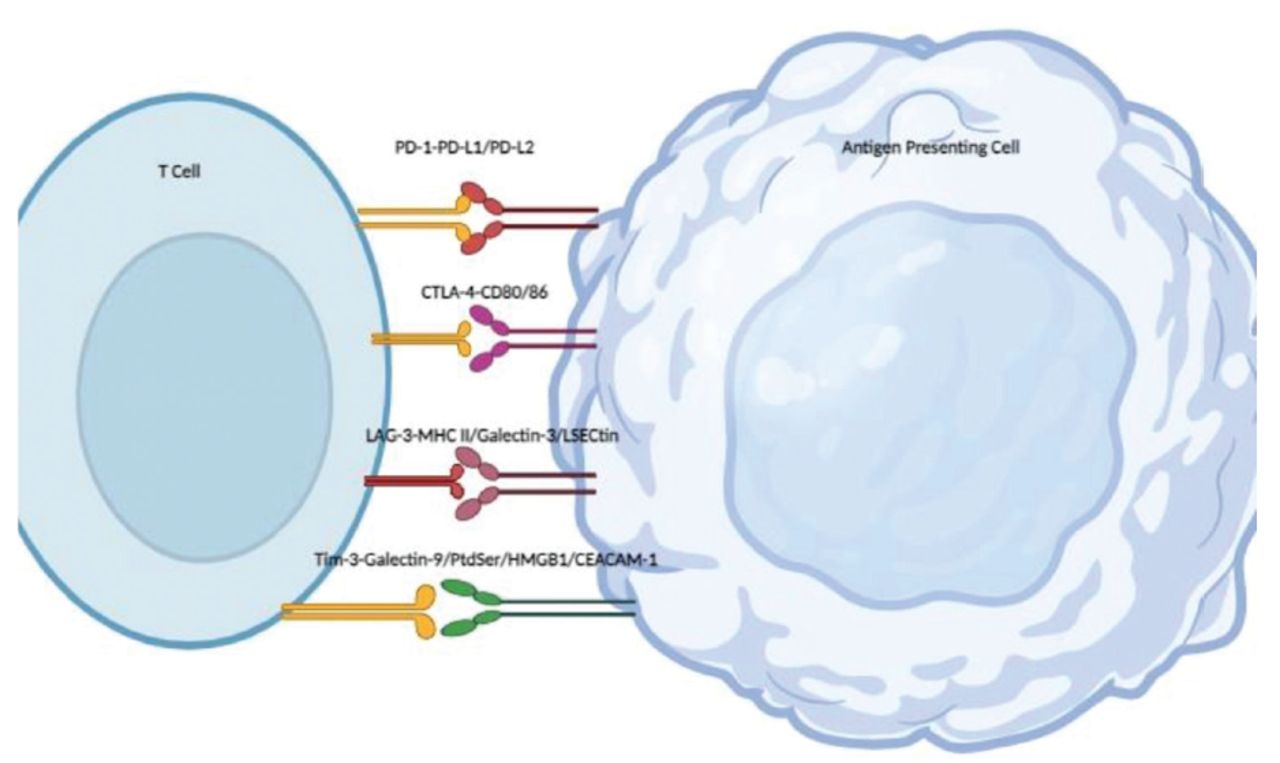
Also, worth describing here is immune checkpoint inhibitors (ICIs) as the brand-new platform in the immunotherapy realm. Most immune checkpoints are expressed in the adaptive, primarily T-cells, and innate immune systems. They are keys for self-tolerance maintenance but in cancer this is not beneficial because immune checkpoints enervate the anticancer response.57 The ICIs are aimed at removing inhibitory signals of T-cell activation and thus re-enabling reactive T-cells to mount an effective antitumor response.60 There are some major immune checkpoints, such as programmed cell death protein-1 (PD-1), cytotoxic T-lymphocyte antigen-4 (CTLA-4), T-cell immunoglobulin and mucin-domain-containing-3 (TIM-3) as depicted in Figure 3.

- Immune checkpoint-based immunotherapy.
Among ICIs, PD-1-based ICI is the most popular. Its clinical implementation has reached a much wider scope of cancers, including BC, although it was initially approved by the FDA for non-small cell lung cancer (NSCLC). Pembrolizumab, a humanized monoclonal antibody that targets the cell surface of PD-1, which was approved by the FDA in 2015 to treat metastatic NSCLC, is the most studied ICI.59 The KEYNOTE-119 (a phase III trial) enrolled 622 metastatic TNBC patients to compare the overall survival (OS) of those being treated with pembrolizumab at a dose of 200 mg intravenously every 3 weeks and those being treated with chemotherapy such as capecitabine, eribulin, gemcitabine, or vinorelbine 1-2 before the course of treatment. The length of OS of those patients with a combined positive score (CPS) beyond 10 with the pembrolizumab was 12.7 months, whereas those with chemotherapy had 11.6 months.61 In a separate study by Cortes et al,62 where the pembrolizumab was applied in combination with chemotherapy, the pembrolizumab effect was shown to increase by PD-L1 enrichment. Grades 3-5 treatment-related AE rates in the pembrolizumab-chemotherapy cohort were observed at a level of 68%, whereas in the placebo-chemotherapy cohort was at 67%. These suggested that the combination of pembrolizumab with standard chemotherapy for the first-line treatment of metastatic TNBC was beneficial.62
As such, it can be highlighted that recent platforms of intervention are directed toward more targeted therapy. To do that, immune and genetic profiles, especially those that are widely known as crucial players in tumorigenesis, should be integrated synergistically. This is critical to determining the proper treatment course, which should not only be aimed at prolonging the OS or disease-free survival but also preventing off-target toxicity that might potentially develop into debilitating comorbidities such as lymphedema.63
Inspired by novel findings of the molecular signature of cancers, targeted therapy has also been terrifically improving. This therapy is a type of treatment that blocks the growth of cancer cells by perturbing key molecules in carcinogenesis and tumors rather than by interfering with rapidly multiplying cells as with conventional chemotherapy. This is also referred to as “personalized medicine”. To date, the number of FDA-approved monoclonal antibodies and small molecules targeting cancer that suggest a therapeutic approach is growing.64
Breast cancer-targeted therapies are employed to cure patients with overexpression of proteins that are pro-tumorigenic. The most efficient BC-targeted therapy hitherto is therapy that targets Her-2 protein overexpression,65 but there are some other BC-targeted therapies as listed in Table 2.
- Food and Drug Administration approved breast cancer targeted therapy.
These evolvements have shed light on the, mainly, therapeutic realm as they provide the affected patients with alternatives that can be opted for according to their pathological examination and molecular as well as genetic signatures, including hereditary traits, although the latter mentioned is not discussed here. Although none of these can be deemed as their final forms of pertinent evolvements, every further move has created much bigger hopes.
Unlike the other BC subtypes, TNBC is seen as the most challenging type. It is sensitive to chemotherapy. Sequential anthracycline- and taxane-based neoadjuvant chemotherapy (NACT) is, so far, the standard therapeutic approach that renders a pathologically complete response that correlates significantly with long-term survival outcomes in early-stage TNBC. Yet, in the context of effectiveness for patients with residual disease, NACT is still conflicting.66 Capecitabine is also used to treat patients with TNBC, although some reports show that it is less active in TNBC compared to hormone receptor-positive BC, and its use as monotherapy in TNBC is also limited, so it is hard to exhibit its specific function as a curative agent for TNBC. The TNBC alone is a heterogenous BC, making it difficult to stratify right away. Limited data show that the BRCA1 mutation may be the key to the particular sensitivity of TNBC to platinum agents and less sensitivity to taxanes.67 This suggests that we need more biomolecular markers to be incorporated into patient stratification strategies in order to formulate effective and efficacious treatments. This is also the case in BC in general, where heterogeneity is seen not only in the cancer cell population but also in immune cell infiltration, which represents the immunity status of the patients. These orchestrations do not only determine or predict patients’ responses toward therapy but also the therapy that the patients can benefit the most from. Not only are these therapies designed to assure patients achieving their success story in battling BC, but they are also designed to prevent them from more financial loss due to the high price of BC regiments they must afford.
Concluding remarks
The therapeutical platform for BC has evolved tremen-dously as a response to the findings that patients with phenotypes of BC have failed to respond favorably to the mainstay therapies. Unfortunately, these findings become more evident over time and thus demand multidisciplinary attention. More advanced therapy platforms consider not only the results of diagnosis but also risk factors presented by affected patients’ genetic or molecular assessments. These are synchronously tailored to re-strategize with clinical maneuvers through which the patients benefit the most. The status of hormone receptors and molecular signatures of at least RB1 as well as PI3K/Akt are of paramount consideration because their dynamics determine the patients’ responses toward the prescribed treatment. Furthermore, these orchestrations predict the risk of early recurrence as well as off-target cytotoxicity, both of which have frequently been overlooked because the primary aim of cancer therapy in general is to eradicate cancer cells. The eradication, however, has consequences that, to some extent, manifest as adverse effects such as fibrosis. The mainstay treatments such as RT and surgery have also shown huge redefinition, as seen in the shifting toward breast conserving surgery and the use of a lower dose or fractionated dose, for which the outcomes showed not less than radical surgery and a higher dose. It is also worth acknowledging that immunotherapy, in parallel to the aforementioned therapy platforms, undergoes improvement (following novel findings on promising targets) in such a way that anti-BC immunity is grandly reinvigorated to put carcinogenesis under excellent control.
Acknowledgment
The authors gratefully acknowledge the Chairperson of Research Center for Vaccines and Drugs (BRIN), Banten, Indonesia, for continuously supporting the effort to carry out the research accordingly. The authors also would like to thank RIZALDI proofreader for English language editing.
Footnotes
Disclosure. This study was supported by Chairperson of Research Center for Vaccines and Drugs (BRIN), Banten, Indonesia.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.