


Abstract
Objectives: To explore the prognostic influence of weight loss (WL) on young overweight/obesity (OW/OB) individuals with heart failure (HF).
Methods: Heart failure enrollees (younger than 45 years, body mass index [BMI] of ≥25 kg/m2) who received medical treatment at Beijing Chaoyang Hospital, Beijing, China, were classified into 2 groups according to whether they experienced significant WL (≥5% from baseline one year after discharge). One-year occurrence rate of major adverse cardiac events (MACEs) comprising cardiac death and rehospitalization for HF was determined.
Results: Of the 191 individuals recruited for this study, 47 had significant WL. The incidence of ischemic heart disease and obstructive sleep apnea syndrome, as well as BMI and blood pressure, were higher in those with significant WL compared to the control group. Although there was no noteworthy discrepancy in the occurrence of cardiac death between the 2 groups, significant WL correlated independently with a lower incidence of HF re-hospitalization (hazard ratio [HR]=0.32, 95% confidence interval [CI]: [0.11-0.91], p=0.032) and overall MACEs (HR=0.37, 95% CI: [0.14-0.94], p=0.036) in young OW/OB individuals with HF.
Conclusion: Significant WL may correlate with favorable prognosis in OW/OB young HF patients.
Obesity (OB) has become a huge burden for the global population. The World Health Organization (WHO) reported that the global prevalence of OB almost tripled from 1975-2016, and nearly 2 billion people were overweight (OW) or obese in 2021.1 Between 2015-2019, approximately 34.3% of Chinese adults became OW, and 16.4% were defined as OB.2 Furthermore, the OW/OB incidence continues to rise among adolescents.1
A previous study confirmed that OB is an independent risk factor for several cardiovascular disorders, including heart failure (HF).3 Generally, HF is considered a primary disease of the elderly, but recent studies have suggested an increasing incidence of HF in younger populations, which is accompanied by a significant increase in body weight and OB.4 It has also been shown that HF patients aged <55 years are more likely to be obese, although the reasons for this association are poorly understood.5 It has been demonstrated that young OB people have a higher susceptibility to developing diabetes mellitus (DM) and hypertension, and these OB-related comorbidities in turn make young patients more vulnerable to HF. Although the overall prevalence of OW/OB was suggested to range from 29-49% in HF patients, studies focusing on the role of OB in young HF patients are rare.6
How weight loss (WL) affects individuals with cardiovascular disease is controversial due to the “OB paradox (OP)”.7 Previous studies showed that WL in chronic HF patients was related to higher long-term mortality, particularly among patients >65 years old.8-10 Interestingly, a recent consensus recommended at least a 5-10% WL for HF patients individuals whose BMI exceeds 35 kg/m2.11 It is hypothesized that excessive body weight in elderly people with HF may be protective against the catabolic complications of HF, but it is not yet completely understood how WL affects clinical outcomes in young HF individuals with OW/OB.12 Accordingly, we explored the prognostic influence of WL in young HF patients with OW/OB in this study.
Methods
After searching the electronic medical records, HF patients between 18-45 years of age with a BMI of ≥25 kg/m2 and New York Heart Association (NYHA) class II-IV were included in this study following the diagnosis recommendations provided by the European Society of Cardiology guidelines.13 Patients were assigned to either a WL of non-WL group according to whether they experienced significant WL (≥5% from baseline one year after discharge from January 2018 to December 2020). Baseline demographic characteristics and clinical parameters were obtained one year after discharge. Healthy eating habits and physical activity were consistently suggested, while WL was not compulsory. Those affected by one of the following illnesses were not enrolled: I) serum alanine aminotransferase ≥3 times the maximum normal value and serum creatinine ≥3 mg/dl; II) end-stage disease (namely, end-stage cancers); and III) no available information of weight. All patients were subjected to physical examinations, laboratory tests, and echocardiography examinations. All patients received standard medication for HF treatment, with the exception of drug use contraindications.
The enrolled population was followed up by outpatient or telephone visits during November and December 2021. The primary observed outcome was major adverse cardiac events (MACEs) within the initial year following WL, including cardiac death and re-hospitalization for HF. All participants signed informed consent forms upon accepting individual interpretation. The research protocol followed the Declaration of Helsinki (2013) and received endorsement from the ethics committee of Beijing Chaoyang Hospital, Beijing, China (2021-ke-623).
Statistical analysis
Continuous data are presented as the mean ± standard deviation (SD) or median (interquartile range [IQR]), and categorical data as numbers and precentages (%). Intergroup comparisons were achieved utilizing the independent-sample t-test or Kruskal-Wallis tests for continuous data according to distribution and the χ2 test for categorical data. Multivariate Cox regression was carried out to evaluate the underlying independent association between WL and MACEs. Cox proportional hazards regression analyses were carried out to obtain hazard ratios (HR) along with the corresponding 95% confidence intervals (CIs). The multivariate model comprised age, gender, BMI, NYHA class, etiology of HF, medical history, HF types, blood pressure (BP), heart rate, malignant arrhythmias (MA), laboratory tests, echocardiography, and medications used. A Kaplan-Meier curve was plotted. Backward selection was carried out to determine the optimal fixed structure using the likelihood ratio test with the estimation of the maximum likelihood. The Statistical Package for the Social Sciences, version 24.0 (IBM Corp., Armonk, NY, USA) was used for data analyses, with a p-value of <0.05 indicating statistical significance.
Results
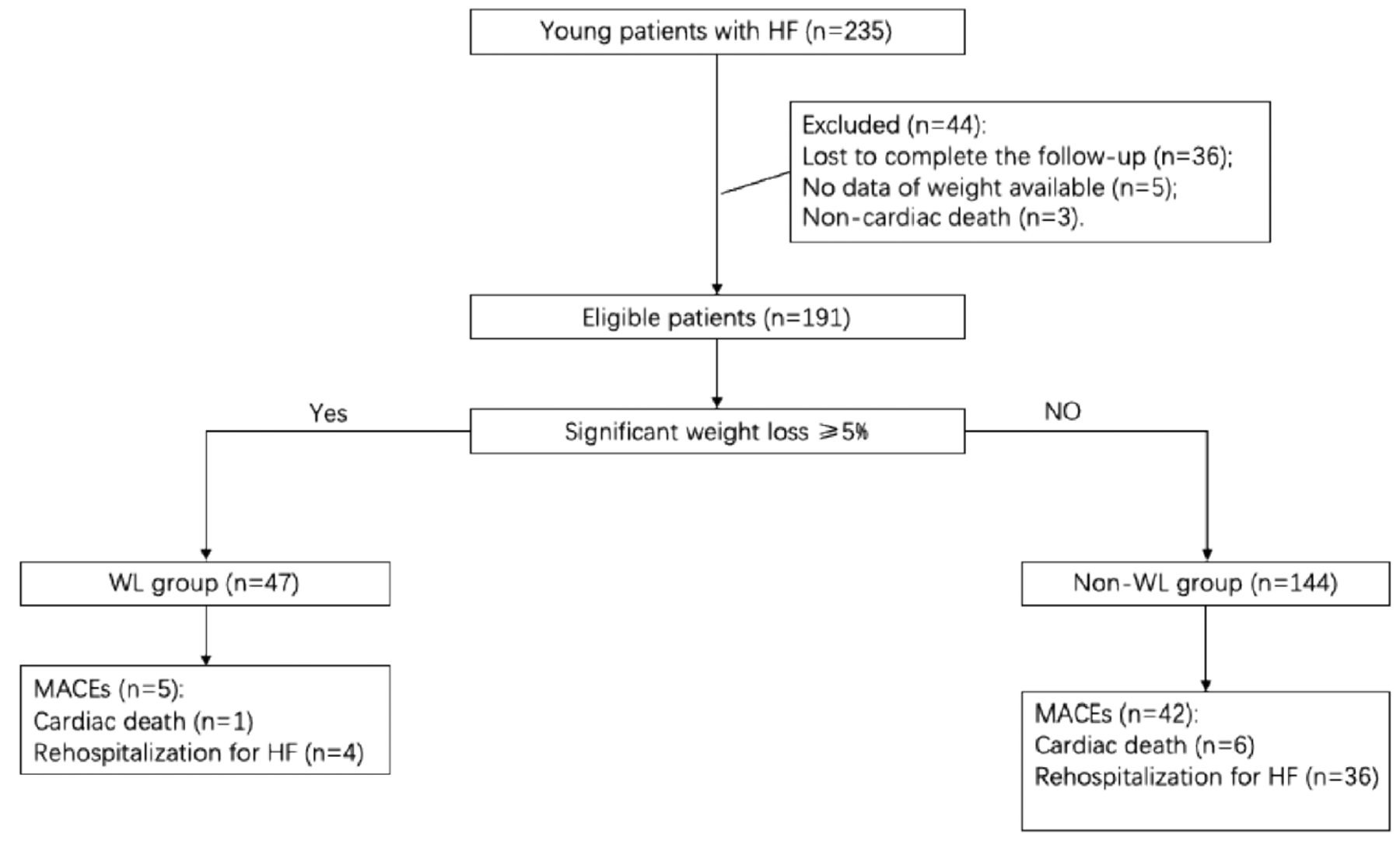
In total, 235 individuals met the inclusion criteria, with 191 patients finally enrolled in our study, including 47 with significant WL and 144 without significant WL. Reasons for the exclusion of 44 patients are shown in Figure 1. Among the included patients, 36 did not complete the follow-up, 5 had no data of weight (those were disabled or failed to have weight data), and 3 suffered non-cardiac death (one died from cancer, one died from accident, and one died from stroke).

- Flowchart of patient inclusion. HF: heart failure, WL: weight loss, MACEs: major adverse cardiac events
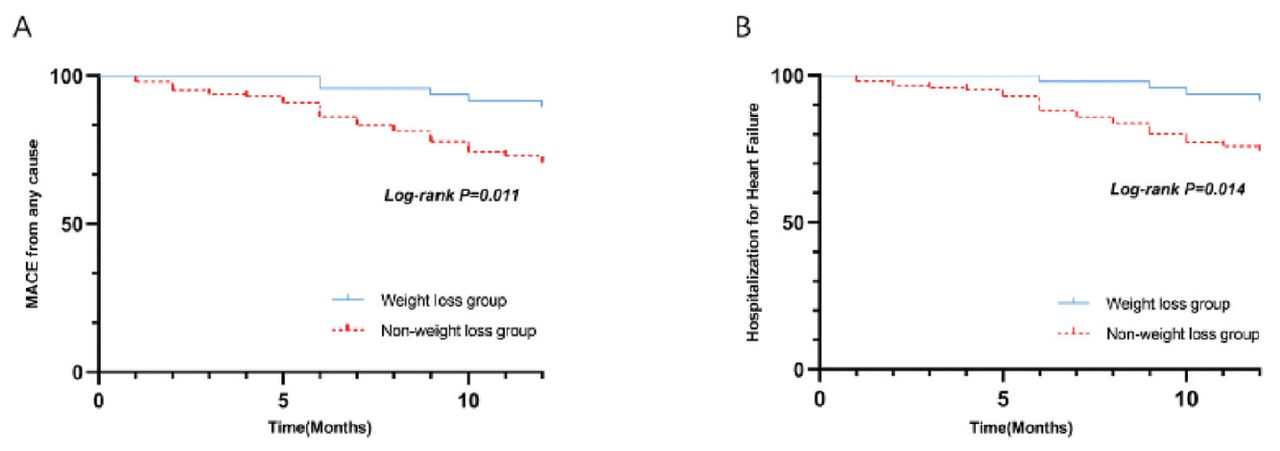
The included patients were predominantly male, with an average age of 37.9 years of age and an average BMI of 29.3. Table 1 presents the baseline characteristics. For etiology, the WL group had more patients with ischemic cardiomyopath compared to the non-WL group. The WL patients were more prone to have obstructive sleep apnea syndrome and exhibited higher BMI and systolic and diastolic BP than patients without WL. There were no noteworthy variations in laboratory tests and echocardiography except left atrial diameter between the 2 groups. During the one-year follow-up, 5 in the WL group and 42 in the non-WL groups had MACEs (Table 2). Patients with significant WL had a lower likelihood of HF re-hospitalization (36 vs. 4, p=0.016), although the incidence of cardiac death was not statistically different between groups. Results of the Kaplan-Meier analysis showed similar results (Figure 2). Subsequent multivariate Cox regression analyses showed that WL was independently correlated with a lower risk of HF re-hospitalization (HR=0.32, 95% CI: [0.11-0.91], p=0.032) and overall MACEs (HR=0.37, 95% CI: [0.14-0.94], p=0.036) in young OW/OB individuals with HF. Moreover, coronary artery disease (CAD), DM, and renal dysfunction were independently related with a higher risk of HF re-hospitalization, whereas MA was also associated with MACEs in our cohort of young patients with HF (Tables 3 & 4).
- Baseline characteristics of patients one-year after discharge.
- Incidence of major adverse cardiac events and other clinical outcomes in the weight loss and control groups.

- Survival curves in patients with and without significant weight loss. A) Major adverse cardiac events and B) re-hospitalization for heart failure. MACEs: major adverse cardiac events
- Multivariable Cox regression analysis for the predictors of heart failure re-hospitalization.
- Multivariable Cox regression analysis for the predictors of major adverse cardiac events.
Discussion
As OB becomes more prevalent in young people, the incidence and prevalence of HF in these populations are expected to increase. Considering the previously proposed OP in HF individuals, how WL contributes to prognosis of HF patients remains unknown, particularly in the young. This study evaluated the influence of significant WL on clinical outcomes after one year in young OW/OB individuals bearing HF. The key discovery was that significant WL was linked to reduced re-hospitalization for HF in this population without significantly affecting the risk of cardiac death, which was consistent with the findings of the RICA registry, but differed from previous studies.8-10,14-16
Age was a primary contributing factor to the results of this study. A previous meta-analysis showed that WL was independently linked to increasing all-cause mortality risk for chronic HF individuals.17 However, patients enrolled in previous studies were older than 60 years. Zamora et al8 suggested an association between WL and greater long-term morbidity, especially in obese HF patients with an average age of 65.8 years. To our knowledge, this study is pioneering in examining the influence of WL on HF individuals aged <45 years. However, the mechanisms underlying the different impacts of WL on prognosis dependent on age remain unclear. One potential factor may be the different pathophysiological characteristics of HF in the elderly and the young. Overweight of aging adults is believed to be beneficial in preventing HF-related metabolic comorbidity, constituting one type of “metabolic pillow” that minimizes cachexia.12
All individuals in this study had OW/OB, with an average BMI of 29.3 kg/m2, which was greater than that in the SOLVD and CHRAM trials and RICA registry. It has been accepted that WL can contribute to cardiac cachexia in normal or underweight patients, which could lead to a poor prognosis. We also found that those having a greater baseline BMI had a great probability of significant WL one year after discharge. Thus, a higher BMI may be beneficial for patients with significant WL, which supports the consensus that a minimum target WL of 5-10% is suggested for individuals with established HF and a BMI of ≥35 kg/m2.11 Moreover, previous studies mainly focused on mortality, and a majority of these studies did not analyze the relation between WL and the re-hospitalization outcome for HF. In this study, we identified an independent association of significant WL with reduced HF re-hospitalization risk. The reason for the decrease in re-hospitalization is unclear, but we hypothesize that WL may be associated with improved hemodynamics in young OW/OB individuals with HF, probably as a result of physical exercise.
The patient cohort in this study may have had different types of HF compared with patient cohorts in previous studies. More specifically, most previous studies involved patients who had HF with reduced ejection fraction (HFrEF). In our study, 61.25% of the population enrolled showed an ejection fraction of ≥40%. In another prior study, HF with preserved ejection fraction (HFpEF) reportedly accounted for more than 50% of HF patients, and >80% of the HFpEF patients were OW/OB.19 Further, OB was nearly twice as common in middle-aged people compared to older people with HFpEF.20 It has been suggested that substantial WL with bariatric surgery or caloric restriction may be promising therapeutic approaches for OB-induced HFpEF.21,22 Thus, different types of HF might alter the influence of WL on clinical outcomes. In our study, we were unable to carry out sub-groups analysis based on HF types given the limited sample numbers in the WL group. Consequently, large-scale studies are warranted in the future.
The severity of HF, as evaluated by the NYHA classification, may also affect the prognostic impact of WL in HF patients.23 The RICA registry study observed no apparent discrepancy in mortality and re-admission between individuals with and without significant WL for acute decompensated HF.24 However, the CHARM and SOLVD trials involved ambulatory, stable patients without overt congestion, and the J-MELODIC sub-analysis included mild chronic HF outpatients.18 These analyses showed that WL was a predictive factor for adverse outcomes. In our study, most patients hospitalized had edema, and therefore the overt congestion status of the patients may partly explain why our study results vary from previous reports.
Comorbidities, such as diabetes, may affect the influence of WL on the prognosis of HF. Significant WL was linked to a lower one-year mortality in non-DM patients but not in DM patients. In patients who were obese before a HF diagnosis, the one-year mortality did not differ between the DM and non-DM populations.25 In our study, we were unable to explore the potential influence of DM status the prognostic impact of WL in young HF individuals due to the limited sample size. Future studies with adequate sample size should be carried out to address this potential factor. Similar to previous findings, our Cox regression analysis revealed associations of CAD, DM, and renal dysfunction with elevated HF re-hospitalization risk in young HF patients, whereas MA was associated with an elevated risk of MACEs. A previous study showed that arrhythmia, hypertension, and CAD were risk factors for HF.26 Furthermore, hypertension, CAD, arrhythmia, and DM were shown to be strong predictors of HF in the young population.26 As for the influence of renal function, it has been suggested that adults with severe OB, BMI of >35 kg/m2, HF or chronic kidney disease may gain benefits from lifestyle alterations leading to intentional WL, which were not seen in patients with mild-to-moderate OB.27
Study limitations
First, WL was not compulsory in our study, as both intentional and unintentional WL were included in our analysis, which might have affected the study outcomes. Secondly, the sample size in our study was relatively small, and sub-group analyses could not be carried out. Future studies with larger sample sizes should be carried out. Thirdly, the characterization of significant WL (≥5% reduction in body weight from baseline one year after discharge) might be arbitrary because no consensus cut-off values for defining WL have been reached, which may be a common limitation of previously published similar studies.8,14,24 Lastly, this retrospective, single center study could only evaluate the association between WL and one-year outcomes after discharge. Multicenter and prospective studies with prolonged follow-up will be necessary to verify the above findings.
In conclusion, the findings of this study revealed an association of significant WL with favorable clinical outcomes in young OW/OB patients with HF, thus supporting the recommendation of WL in young HF individuals with OW/OB.
Acknowledgment
The authors gratefully acknowledge Medjaden Inc. (www.medjaden.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received January 7, 2024.
- Accepted February 16, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.




{kind=link}
{kind=link}