


ABSTRACT
Objectives: To analyze the outcomes of carotid endarterectomy in individuals with carotid artery stenosis in the context of a tertiary care center.
Methods: We carried out a retrospective cohort investigation between 2015-2022. Patient data includes demographics, risk factors, preoperative medications, and operative details. The primary outcomes were 30-day postoperative stroke and mortality rates, while the secondary outcome of the study was to assess the morbidity of the procedure.
Results: The mean age of the 54 patients was 66.9±9.88 years, and 57.4% were men. The 30-day stroke rate was 3.7%, and the mortality rate was 1.9%. Most patients did not develop postoperative complications; however, surgical site hematoma was the most common complication encountered (12.9%). Long-term follow-up showed disease regression in 68.5% of patients, with a minority of patients developing ipsilateral restenosis. Admission to an intensive care monitoring unit was the only independent predictor of postoperative complications.
Conclusion: This study provided insights into the outcomes of carotid endarterectomy in patients with carotid artery stenosis, emphasizing the importance of careful patient selection and postoperative monitoring. Perioperative risks, including stroke and mortality, were within acceptable limits. Further research incorporating structured and non-structured data for predictive analyses, should explore refining patient profiling and optimizing treatment approaches for different carotid artery stenosis clinical and morphological presentations.
Carotid artery stenosis (CAS), also termed carotid artery disease, is a clinical condition marked by the constriction or obstruction of the carotid arteries, primarily owing to atherosclerosis. Plaques can develop anywhere along the carotid artery, extending from its origin at the aortic arch to its termination within the cranial region; however, the term CAS refers to the atherosclerosis process at the common carotid artery bifurcation, particularly incorporating the origin of the internal carotid artery and the carotid bulb.1 Carotid artery stenosis can induce cerebral hypoperfusion, resulting in increased susceptibility to ischemic strokes. Despite the compensatory function of the circle of Willis in individuals with asymptomatic CAS, symptomatic CAS is responsible for approximately 20% of stroke cases.2 Notably, approximately 2% of the adult population is estimated to have asymptomatic CAS.3
Common risk factors for CAS include non-modifiable conditions, such as old age and male gender, and diverse modifiable factors, such as tobacco smoking, dyslipidemia, hypertension, and diabetes mellitus. Other risk factors encompass obesity, physical inactivity, and a family history of cardiovascular disease or CAS. Moreover, high dietary intake of saturated fats, trans fats, and cholesterol can contribute to the buildup of arterial plaques.4
Early management and treatment of CAS are crucial, considering its association with ischemic strokes.5 Medical therapy advancements have contributed to a reduced stroke rate in individuals with symptomatic and asymptomatic CAS.6 However, Gaba et al7 suggested that advancements in medical therapies have revived uncertainties regarding the generalization of results from older randomized controlled trials, after a comparison of outcomes after carotid intervention with current medical practices. Concerning surgical procedures, different strategies are available. Nevertheless, despite the expanding application of carotid artery stenting, the most effective preventive and therapeutic measure for strokes in atherosclerotic CAS remains carotid endarterectomy (CEA).8 According to the recent guidelines released by the Society for Vascular Surgery, CEA is the primary option for symptomatic low-risk surgical cases with 50-99% stenosis and asymptomatic individuals presenting with 70-99% stenosis.9
Carotid endarterectomy is considered highly effective for CAS; nevertheless, a careful assessment of risks is essential since meticulous surgical procedures can cause stroke in approximately 5-7% of individuals.10,11
Based on these considerations, this study aimed to explore the primary outcomes of CEA in the context of a tertiary care center, specifying 30-day postoperative stroke and mortality rates, while dissecting different variables collected during the perioperative course.
Methods
This investigation employed a retrospective, single-center cohort design. The research was carried out as per the principles stated in the Declaration of Helsinki and was approved by the institutional ethics committee of King Saud University, College of Medicine, Riyadh, Saudi Arabia (project no.: E-23-7516). According to the retrospective nature of the study, informed consent was not required.
Patient data were recorded using a computerized sheet containing all relevant variables, including demographic information and patient risk factors. Variables such as smoking status, presenting symptoms and their duration, degree of stenosis bilaterally, relevant preoperative medications, and the interval between symptoms and surgery were analyzed. Additionally, operative details such as the type of anesthetic utilized, mean carotid clamping time, and type of patch utilized were collected.
The primary objective of this study was to evaluate the 30-day postoperative stroke and mortality rates following CEA. Additionally, we aimed to analyze the procedure’s associated morbidity as a secondary outcome measure. Furthermore, we carried out a comparative analysis distinguishing between patients on single versus dual antiplatelet therapy prior to the operation.
The study included patients that underwent CEA between 2015-2022. Exclusion criteria included individuals of <18 years old and those managed either through best medical therapy or carotid artery stenting.
Surgical intervention was indicated based on the presence of symptoms, such as transient ischemic attacks (TIAs) or strokes, or the degree of stenosis. Patients with symptomatic CAS, experiencing TIAs or strokes, or asymptomatic individuals with severe stenosis, typically defined as 70% or greater narrowing of the carotid artery, were considered candidates for surgical intervention. The evaluation of patients with CAS to assess surgical indications involved a comprehensive approach that combined clinical assessments, imaging studies, and additional diagnostic procedures when deemed necessary. Symptom assessment included TIAs, strokes, or other neurological deficits. Additionally, carotid duplex ultrasound was used to evaluate the extent of the stenosis. In particular, the degree of the stenosis was quantified using established criteria, based on the North American Symptomatic Carotid Endarterectomy Trial (NASCET). The preoperative assessment was also aimed at unveiling high-risk features, such as ulceration or intraplaque hemorrhage. These features contribute to the overall risk stratification of our patients for surgical intervention.
The procedures were carried out under general or local anesthesia. Patients were either taking single or dual antiplatelet therapy preoperatively. Concerning technical aspects, an incision was made along the medial side of the sternocleidomastoid muscle, dissecting deeply until the carotid artery was exposed. Therefore, both ends of the artery were clamped. Subsequently, the surgeon incised along the length of the artery to assess both ends of the plaque. The clamps were gradually released, and a flexible shunt was carefully introduced to maintain distal perfusion around the endarterectomy site while clearing the blockage. A routine shunt was placed for most cases. Finally, the plaque was removed, tacking sutures were added, and a patch was placed on the arteriotomy site. Concerning the postoperative assessment, arterial assessments using carotid duplex ultrasound are carried out to monitor for complications and potential postoperative restenosis. Moreover, patients underwent regular and systematic assessments 30 days after the procedure, every 6 months for 2 years, and then annually thereafter.
We carried out a statistical power analysis for comparing single (n=22) and dual (n=32) antiplatelet therapies. The findings indicated that, based on the obtained sample sizes for each group, the post-hoc test of power (1-β err prob) yielded a result of 0.923 or 92.3%, surpassing the minimum threshold of 0.80. Therefore, the attained statistical power for this specific test, employing a 2-tailed parameter, a medium effect size, and an alpha level of 0.05, affirms the adequacy of the sample sizes for both single (n=22) and dual (n=32) antiplatelet therapies.
Statistical analysis
Descriptive statistics were calculated, with categorical variables shown as frequencies and proportions (%), while continuous variables were shown as mean and standard deviation (SD). The relationship between preoperative medications and patient baseline, operative, and postoperative characteristics was carried out using Fischer’s exact test and independent sample t-test. Univariate regression analysis was executed to assess the predictors of postoperative complications. Statistical significance was set at a p-value of <0.05. We analyzed data using the Statistical Packages for the Social Sciences software for Windows, version 26.0 (IBM Corp., Armonk, NY, USA).
Results
The analysis encompassed a total of 54 patients, of whom 31 (57.4%) were men and 23 (42.6%) were women. The mean age was 66.9±9.88 years. The patients were predominantly nonsmokers (83.3%). Most patients had severe ipsilateral stenosis (96.3%), with no stenosis on the contralateral side (40.7%). Before the procedure, 59.3% of patients received dual antiplatelet therapy and 40.7% received single antiplatelet therapy. Most patients were symptomatic at presentation (75.9%). Surgery was indicated in the remaining 24.1% of patients who were asymptomatic owing to the presence of high-grade stenosis. The mean interval between symptom onset and surgery was 15.4±11.2 days. Table 1 provides a summary of patient demographics and clinical characteristics.
- Baseline characteristics of the patients (N=54).
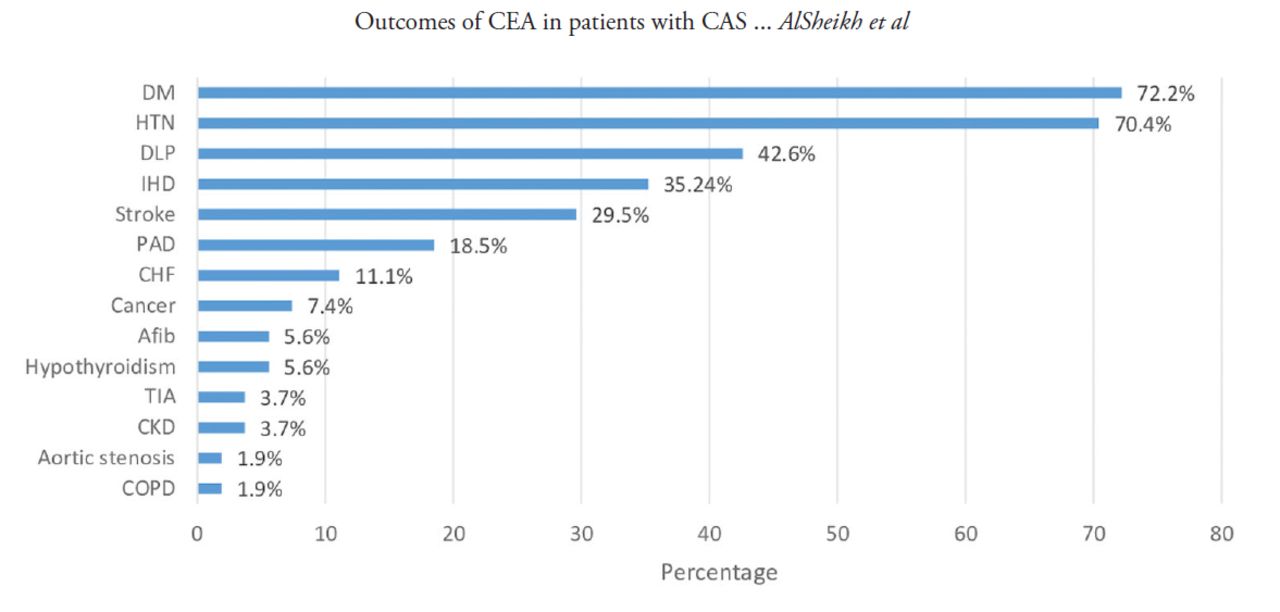
There was a notable prevalence of patients with comorbidities, such as diabetes (72.2%), hypertension (70.4%), dyslipidemia (42.6%), ischemic heart disease (35.2%), previous strokes (29.5%), and peripheral artery disease (18.5%, Figure 1).

- Patients risk factors. DM: diabetes mellitus, HTN: hypertension, DLP: dyslipidemia, IHD: ischemic heart disease, PAD: peripheral artery disease, CHF: congestive heart failure, Afib: atrial fibrillation, TIA: transient ischemic attack, CKD: chronic kidney disease, COPD: chronic obstructive pulmonary disease
In the analysis of the surgical characteristics, the mean interval time between symptom onset and surgery was 15.4±11.2 days. No predilection towards the operated side was observed (53.7% right vs. 46.3% left). Almost all patients received general anesthesia (n=53, 98.1%), whereas only one procedure utilized only regional anesthesia. A pericardium patch was preferentially utilized in 94.4% of patients to close the arteriotomy site, with only 3 (5.6%) cases utilizing the Dacron patch. Moreover, the mean carotid clamp time was 13.5±7.75 minutes, which was found to be compatible with most published studies (Table 2).3,7
- Operative characteristics (N=54).
The primary outcome measures in the postoperative course evaluation were stroke (3.7%) and mortality (1.9%) rates. Concerning the secondary outcome measures, most patients did not develop postoperative complications; however, surgical site hematoma was the most commonly reported complication (12.9% of cases). Other less commonly reported complications included seizures (3.7% of cases). Hoarseness of the voice, surgical site infection, and acute coronary syndrome were reported in a minute number of patients (1.9%).
Furthermore, most patients (68.5%) had full regression of their disease at the mean follow-up of 19.9±19.9 months, whereas a minority had mild (18.5%), moderate (1.9%), or severe (1.9%) restenosis. One patient had an incidental carotid floating thrombus during a long-term follow-up, which was managed conservatively.
The mean length of hospital stay was 13.9±12.9 days. Half of the patients necessitated admission to either the intensive care unit (ICU) or high dependency unit (HDU). Additionally, the average duration of stay in the ICU or the HDU was 1.98±4.22 days (Table 3). This relatively long hospital stay can be attributed to patient admission to the neurology unit, with the surgery being performed within the same index hospital admission.
- Postoperative course and outcomes (N=54).
The relationship between preoperative medication according to patient baseline, preoperative, and postoperative characteristics was evaluated (Table 4). Patients received either single or dual antiplatelet therapy. The 2 groups did not vary significantly regarding patient age, gender, smoking status, symptoms, operated side, the interval between symptoms and surgery, carotid clamp time, ICU or HDU stay or admission, and ward and total hospital stays (p>0.05).
- Univariate analysis on the relationship between preoperative medication (single vs. dual antiplatelet therapy) and baseline and postoperative variables (N=54).
The analysis of the most common risk factors showed that ischemic heart disease was significantly more prevalent in patients receiving single antiplatelet therapy than in those receiving a dual strategy (59.1% vs. 18.8%; p=0.004). In contrast, a significant difference was observed in the prevalence of previous strokes between the 2 groups: 13 (40.8%) patients receiving dual antiplatelet therapy had a previous history of stroke compared with only 3 (13.6%) cases among those receiving single antiplatelet therapy (p=0.039). However, there were no significant differences in risk factors, including hypertension, diabetes, peripheral artery disease, dyslipidemia, and congestive heart failure, between the 2 groups (p>0.05). Moreover, a significant difference was observed in the indication for surgery between the 2 groups: 14 (63.6%) patients receiving single antiplatelet therapy had a stroke as an indication for surgery compared with 50% of those receiving dual antiplatelet therapy (p=0.043).
Furthermore, only postoperative admission to the ICU/HDU was identified as a predictor of postoperative complications, wherein patients admitted to ICU/HDU were 4.7 times more likely to have postoperative complications than those who did not require intensive care monitoring (odds ratio [OR]=4.706; 95% confidence interval [CI]: [1.124-19.704]; p=0.034, Table 5).
- Univariate analysis on the relationship between preoperative medication (single vs. dual antiplatelet therapy) and
Discussion
Carotid artery stenosis is a major cause of acute ischemic cerebrovascular events; however, interventional procedures for the secondary prevention of strokes are usually under-utilized.12 An accurate definition of risk profiles, with an assessment of variables related to the pre-surgical course and elements closely related to the procedure and its outcomes, can be a valuable opportunity for establishing calibrated pathways. Similarly, it can aid in encouraging the implementation of invasive methods in areas where there is a greater need. These considerations are particularly essential in clinical scenarios with greater uncertainty, such as the optimal management of individuals with asymptomatic severe carotid stenosis.13
In contrast to medical therapy, extended follow-up has demonstrated a significant reduction in the occurrence of ipsilateral stroke and death among patients with severe CAS who undergo CEA.14 The analysis of our sample of CEA procedures revealed a 3.7% postoperative stroke rate and a 1.9% mortality rate, consistent with the values reported in a larger case series. For example, Bennett et al15 found that the overall one-month postoperative stroke or death rate was 3%, with a breakdown of 1.9% in asymptomatic patients and 4.6% in the symptomatic cohort.
Concerning preoperative risk, a high prevalence of comorbidities was found in our cohort, with the most common comorbidities being diabetes (72.2%) and hypertension (70.4%). This is consistent with results from other studies that identified these clinical conditions as major stroke risk factors in patients with CAS.13 The treatment of CAS depends on the occurrence of symptoms and the degree of stenosis. Carotid artery stenosis is particularly beneficial for asymptomatic patients with ≥70% stenosis; however, those with 50-69% stenosis may only experience marginal benefits.9 In our study, 41 (76%) patients were symptomatic, 30 (55.6%) of whom presented with symptoms of a stroke, and 11 (20.4%) presented with a TIA. Notably, evaluating the prevalence of TIA is challenging since most patients who experience a TIA fail to report it to a healthcare provider.16 Furthermore, 13 (24.1%) patients were asymptomatic, indicating a lower prevalence than that reported in a previous study involving a similar patient population.17
Many of our patients (96.3%) had a severe degree of ipsilateral stenosis (>70%), with only 2 (3.7%) having a moderate degree of stenosis (50-69% stenosis). The most common symptom among symptomatic patients was dysarthria (38.9%), followed by hemiparesis (37%), which is similar to the reports of a study involving a corresponding patient population.18
In a previous investigation, Varetto et al19 assessed the impact of early CEA on postoperative complications related to stroke or death in patients with symptomatic CAS. They compared patients who underwent surgery within 2 weeks to those operated on after 2 weeks and suggested that those who received earlier treatment were more likely to have a better neurological outcome. In our study, the mean interval between symptom onset and surgery was just over 2 weeks. Our analysis did not demonstrate a statistically significant association between an increasing interval between symptom onset and surgery and the presence of postoperative complications.
The carotid clamping time is a vital element of the CEA procedure. Several studies have emphasized that reducing carotid clamping times may decrease the risk of adverse events in patients undergoing this intervention.20,21 In our center, the mean carotid clamping time was 5.3±3.7 minutes; however, no significant link between prolonged clamping time and the development of postoperative complications was found. This may be attributed to the accurate preoperative diagnostic methods and prudent application of the shunting approach.
The analysis demonstrated that 32 (59.3%) patients received dual antiplatelet therapy, preoperatively, whereas 22 (40.7%) received single antiplatelet therapy. No statistically significant differences were found concerning postoperative complication rates between these 2 cohorts (Table 4). On the other hand, an evidence-based (EBM) analysis demonstrated that dual antiplatelet therapy provides some advantages in CAS, as evidenced by a reduced risk of TIA.22 In contrast, dual antiplatelet therapy was correlated with an elevated risk of bleeding complications in patients undergoing CEA.23
The anesthetic technique has been discussed extensively in previous studies, with general and local anesthesia having advantages and disadvantages with respect to each other.11 Due to the absence of a clear consensus on the anesthetic technique, the decision should be informed by local expertise and consideration of complication rates.24 In our center, almost all patients received general anesthesia (n=53, 98.1%), whereas only one procedure involved only regional anesthesia, with no significant postoperative complications.
Patch angioplasty is a routine procedure following CEA, as it enhances both perioperative and long-term stroke prevention rates and diminishes restenosis rates when compared to primary closure of the arteriotomy.8 All our patients were patched, with pericardium patches being preferentially adopted (94.4%) to close the arteriotomy site, and only 3 (5.6%) cases utilized the Dacron patch. Ren et al25 illustrated that the hemostasis time with a polytetrafluoroethylene (PTFE) patch in CEA exceeded that with a venous or Dacron patch. However, the comprehensive presurgical and long-term mortality rates, stroke rates, restenosis, and operative times demonstrated similarities between using venous and synthetic patch materials or a Dacron patch to PTFE patch material in CEA. Comparable results were achieved in other EBM investigations.26
The analysis of postoperative course and outcomes (Table 3) showed that the most common postoperative complication was surgical site hematomas (13%), similar to the reports in other studies.1,8 Moreover, most patients (68.5%) had full regression of their disease upon further follow-up, whereas a minority had mild (18.5%), moderate (1.9%), or severe (1.9%) restenosis rates.
Finally, regarding predictors of postoperative complications (Table 5), we found that ICU/HDU admission was linked to a 4.7 times increased risk of developing postoperative complications, whereas other predictors, such as baseline, preoperative, and postoperative characteristics, did not yield statistically significant associations. Patients at high surgical risk should receive careful management, with a special focus on modifiable risk factors and calibrated perioperative programs. Using perioperative risk calculation tools and other evaluation strategies is encouraged in these cases.27
Study limitations
This retrospective analysis had some limitations. Notably, the sample size was too restricted to allow generalizability of the results. For instance, a methodological limitation involves the inclusion of cases managed with different anesthesia techniques. Only one patient underwent local anesthesia, with the remaining 98% undergoing general anesthesia. Despite this imbalance, evidence-based investigations confirm that the type of anesthesia does not affect the incidence of stroke or death.11 Additionally, a multivariate analysis encompassing the interplay of numerous variables would have facilitated a more profound comprehension of the investigated associations. However, our choice was to narrow the focus of the analysis to the most pertinent data in the dataset. Given these limitations, we have planned to advance the analysis by employing more sophisticated methodologies, such as principal component analysis, discriminant analysis, multivariate regression, and cluster analysis, taking advantage of a more substantial sample size. Additionally, we are considering implementing machine learning (ML) techniques in the next phase of the study. For instance, Tan et al28 adopted an ML approach to predict postoperative hypertension in patients who underwent CEA. Other studies have also had notable advancements in predicting outcomes following CEA with ML.29 The aim remains to uncover patterns, trends, or associations that might be unclear in the analysis of individual variables.
In conclusion, this study offered significant findings regarding the perioperative risk factors of CEA in individuals with CAS. The results emphasize the significance of meticulous patient selection, careful preoperative medication considerations, and vigilant postoperative monitoring, particularly concerning ICU/HDU admissions. Additional studies incorporating innovative technologies such as artificial intelligence and ML are imperative to advance the comprehension of patient profiling. The findings may guide choices regarding surgical and medical approaches, including the perioperative management of CAS and the subsequent prevention of cerebrovascular complications and other procedure-related events.
Acknowledgment
The authors gratefully acknowledge Editage (www.editage.com) for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received November 17, 2023.
- Accepted March 18, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.