


Abstract
Objectives: To uncover the predictive value of systemic immune-inflammatory index (SII) and systemic inflammatory response index (SIRI) on early pregnancy loss.
Methods: A total of 535 individuals were enrolled in this retrospective analysis. The early pregnancy losses (EPL) group included patients between 18-35 years old who experienced EPL. The control group comprised healthy pregnant women who gave birth at ≥37 weeks.
Results: The EPL group had significantly lower plateletcrit (p=0.04), platelet distribution width (PDW, p<0.0001), and RDW (p<0.0001) and higher monocyte (p<0.0001) and SIRI (p<0.0001) values than the control group. The hemoglobin, white blood cells, platelet count, neutrophil count, lymphocyte count, mean platelet volume, neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR), monocyte-to-lymphocyte ratio (MLR), and SII values were not significantly different between the EPL and control groups (p>0.05). The cut-off value for the SIRI that offers the best sensitivity/specificity balance was 1.48 (sensitivity of 63%; specificity of 63%) in the receiver operating characteristics curve. Among the inflammatory parameters for predicting EPL, PDW had highest specificity (84%), and RDW had the highest sensitivity (80%).
Conclusion: This study provides compelling evidence that various inflammatory pathways may significantly contribute to EPL pathogenesis. Moreover, our findings suggest that SIRI could be a more effective marker than NLR, PLR, MLR, and SII in predicting EPL in an ongoing pregnancy, thereby potentially revolutionizing early pregnancy loss diagnostics.
Early pregnancy losses (EPL) are one of the common problems of the reproductive period, which is the most extended period of a woman’s life. Early pregnancy losses refers to conditions that are diagnosed in the intrauterine period up to 12 weeks and 6 days of pregnancy, wherein fetal heartbeats cannot be monitored and are incompatible with life.1 Although the incidence of EPLs is uncertain, as there may be cases that have not been diagnosed clinically, it has been reported to be approximately 12.8-13.5% in the current studies.2 Approximately 80% of pregnancy losses are detected in the first 12 weeks of pregnancy.3 Despite the high frequency of EPL, its pathophysiology remains not fully understood. When the etiology of EPLs is examined, genetic, infectious, endocrinological, anatomical, and immunological factors come to the fore.4,5 However, approximately 40% of EPLs are classified as idiopathic.5 Investigating the factors affecting EPLs, which are relatively common, may play a key role in preventing these losses.
In previous literature, it was elaborated that inflammation played a significant role in pregnancy loss or threatened abortion (TA).6 Elevated levels of inflammatory mediators (TNF-α, IFN-γ, IL-6, and IL-10) were detected in cases with EPL compared to healthy controls.7 However, the high cost and difficulties in processing these biomarkers limit their utilisation in daily routine practice. Regarding this fact, haematological indices derived from complete blood analysis and white blood cells (WBC) can be preferred due to their ease of use. Platelet-to-lymphocyte ratio (PLR) and neutrophil-to-lymphocyte ratio (NLR) were investigated previously.8-10
In various inflammatory diseases, such as acute pancreatitis and acute coronary disease, or in determining the prognosis of malignancies, the systemic immune-inflammatory index (SII) and systemic inflammatory response index (SIRI) were utilised as biomarkers.11-13 Within the scope of this research, we aimed to elucidate the predictive value of SII and SIRI on EPL.
Methods
A total of 535 individuals were enrolled in this retrospective analysis. Patients between 18-35 years old who experienced EPL were included in the EPL group. The control group comprised healthy pregnant women who gave birth at ≥37 weeks. Among healthy pregnant women who had EPL and had a live birth after 37 weeks, those with hemogram parameters in the first 7 weeks were retrospectively scanned and analysed. Patients whose data could not be accessed, who had fetal chromosomal/structural anomalies, multiple pregnancies, pregnancies with assisted reproductive technology, recurrent pregnancy loss (RPL), chronic maternal nicotine and alcohol use, any medical disease history, and congenital uterine anomalies were excluded from the study.
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Ethics committee approval has been granted from Istanbul Başakşehir Çam and Sakura Hospital, Istanbul, Turkey, on 13/09/2023 with protocol number 224.458.204. As this was a retrospective research, no informed consent was obtained from participants.
Patient data were obtained from the hospital’s information system and patient records. Patients’ age, gravida, parity, miscarriage, and body mass index (BMI) were evaluated when the blood sample was obtained. All blood count analyses were carried out in the same Istanbul Başakşehir Çam and Sakura Hospital, Istanbul, Turkey, laboratory. Hemoglobin (Hb), WBC, neutrophil count, lymphocyte count, platelet (PLT) count, plateletcrit (PCT), platelet distribution width (PDW), red cell distribution width (RDW), and mean platelet volume (MPV), along with the newly identified inflammatory markers NLR, PLR, monocyte-to-lymphocyte ratio (MLR), SII, and SIRI, were retrospectively examined. Systemic immune-inflammatory index was calculated as (PLT count × neutrophil count/lymphocyte count). Systemic inflammatory response index was calculated as (monocyte count × neutrophil count/lymphocyte count). The success of all variables in predicting EPL and the cut-off values of the significant ones were calculated.
Complete blood count (CBC) research used tubes containing tri-potassium ethylenediaminetetraacetic acid. Its parameters were measured by flow cytometry using an automatic haematology analysis device (XN1000, Sysmex, Roche Corp., Japan).
Statistical analysis
Statistical software package SAS, version 15.2 (SAS Institute Inc.) was used for statistical analyses. Continuous variables were tested for the normality assumption using the Kolmogorov-Smirnov test. In this study, the comparison between case and control groups regarding sociodemographic and clinical characteristics was carried out using 2 statistical tests. For categorical data, the Chi-square test was applied. This test is suitable for determining if there is a significant association between 2 categorical variables. For continuous data, the Mann-Whitney U test was utilized. A p-value of <0.05 was deemed statistically significant in this analysis.
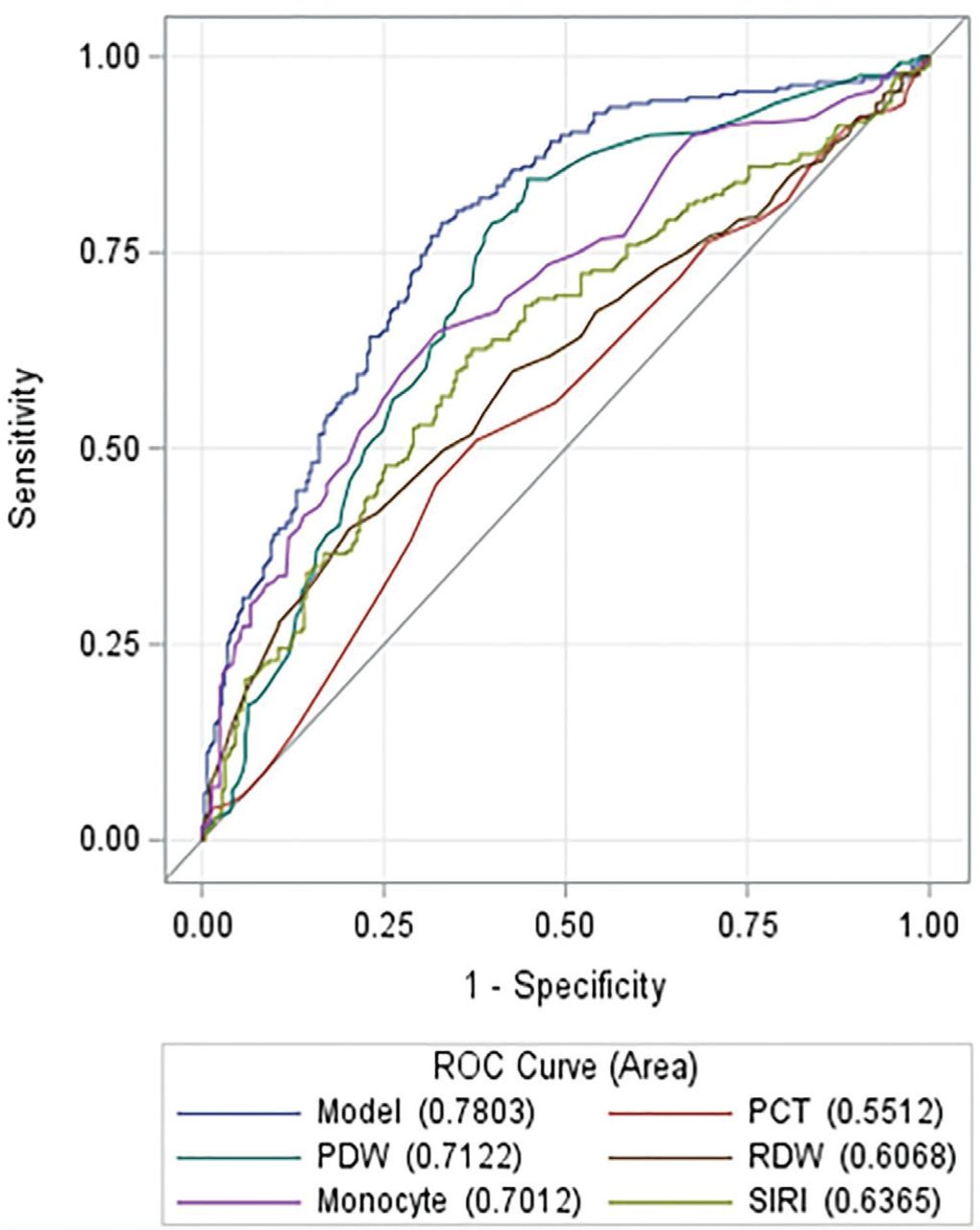
In this study, the predictive power of several biomarkers (PCT, PDW, RDW, monocyte count, and SIRI) in identifying missed early miscarriages was assessed using receiver operating characteristic (ROC) curves. The area under the curve (AUC) was calculated for each parameter to quantify their discriminative ability.
Results
Overall, 249 patients with EPL were compared with 286 individuals in the control group who gave birth at term. The median age of the EPL group was 27.5 years and the median age of the control group was 27.1 years. No significant difference was observed between the 2 groups in terms of age, BMI, gravida, parity, and abortion. Demographic characteristics, blood count parameters, SII, SIRI, and other inflammation indices of the study population are presented in Table 1.
- Demographic and clinical characteristics of the participants.
The EPL group had significantly lower PCT (p=0.04), PDW (p<0.0001), and RDW (p<0.0001) and substantially higher monocyte (p<0.0001) and SIRI (p<0.0001) values than the control group. The Hb, WBC, PLT count, neutrophil count, lymphocyte count, MPV, NLR, PLR, MLR, and SII values were not significantly different between the EPL and control groups (p>0.05).
The ROC curve was used to analyse the performance of inflammatory parameters in predicting EPL. For EPL diagnosis, to determine the cut-off values that provide an optimal balance of sensitivity and specificity, we used the Youden index. The cut-off value for the SIRI that offers the best sensitivity/specificity balance was 1.48 (sensitivity of 63% and specificity of 63%) in the ROC curve. Among the inflammatory parameters for predicting EPL, PDW had the highest specificity (84%), and RDW had the highest sensitivity (80%). The corresponding AUCs and 95% confidence intervals are presented in Table 2 and Figure 1.
- Biochemical parameters and inflammatory indices for early pregnancy loss.

- Receiver operating characteristic curves for comparisons. ROC: receiver operating characteristic, PDW: platelet distribution width, PCT: plateletcrit, RDW: red cell distribution width, SIRI: systemic inflammatory response index
Discussion
In this study, data of patients who experienced EPL and healthy pregnant women who had a live birth at ≥37 weeks of gestation were retrospectively examined regarding routinely measured CBC parameters in the first 7 weeks, and novel inflammatory markers were calculated from these. Certain serum inflammation markers were associated with EPL in this study, which investigated the relationship between inflammation and EPL. This suggested that increased inflammation can play a role in EPL pathogenesis and that SIRI can be a helpful marker in EPL prediction.
In obstetrics, the role of the inflammatory process in the etiopathogenesis of EPL and RPL has been demonstrated.8,14,15 Peripheral blood contains pro-inflammatory cells, such as neutrophils, PLTs, and monocytes, as well as immune cells, including lymphocytes.16 In our study, higher levels of monocytes were detected in EPL compared to healthy pregnant women. This result is consistent with the detection of higher monocyte values in the peripheral blood of women with RPL in the literature.17 Recent studies have shown that monocytes are involved in basic steps such as trophoblast invasion and tissue and vascular remodeling.18
The relationship between NLR, PLR and EPL, which are good indicators of systemic inflammation, has been valuted in a few studies.8,15,19 Biyik et al8 elaborated that PDW, NLR, and PLR were higher, and MPV was lower in miscarriage incidents (n=40) compared to 40 healthy pregnancies. Liu et al9 examined the relationship between missed miscarriage and inflammation. However, they could not detect a significant change in NLR and PLR values, and they stated that patients with missed miscarriages had decreased MPV compared with healthy pregnant women. Ata et al19 indicated that MPV and PLR were significantly lower in patients with EPL and TA. Still, no significance was detected regarding Hb, PLT, neutrophil count, and NLR in the first trimester. Similar to these, Oğlak et al15 reported significantly higher NLR and PLR values in EPL patients. On the contrary, no significant results have been achieved in NLR and PLR values in patients with EPL and healthy controls. These outcomes might be attributed to the exclusion of patients with recurrent miscarriages or chronic diseases.
Systemic inflammatory response index is a simple and cost-effective novel inflammatory parameter based on peripheral neutrophil, monocyte, and lymphocyte counts. Previous studies indicated a close relationship exists between SIRI and tumour survival.20,21 However, in obstetrics, SIRI has been used in only a few studies. In a recent study, Seyhanli et al22 reported higher SIRI values in preeclampsia patients’ first-trimester blood samples. Sahin et al23 elaborated that high SIRI values detected in the first trimester in pregnant women with SLE are a strong determinant for predicting adverse pregnancy outcomes. In the current research, we analysed that patients with EPL had significantly higher SIRI values than healthy pregnant women, suggesting that SIRI can be leveraged as a useful inflammatory index that can be used for predicting EPL in an ongoing pregnancy.
On the other hand, SII is another index derived from peripheral PLT, neutrophil, and lymphocyte counts invented by Hu et al24 and used in the prognosis of hepatocellular carcinoma. Systemic immune-inflammatory index has been associated with diagnosing, prognosis, and responding to treating various inflammatory diseases and malignant tumours.25,26 A recent meta-analysis revealed the association between elevated SII and poor prognosis in gynaecological, breast, ovarian, and triple-negative breast cancer.24 In the study carried out by Turgut et al,27 miscarriage rates were compared among healthy pregnant women with vaginal bleeding history before 20 weeks of gestation. Consequently, higher SII values can be used as an additional marker in miscarriage prediction in patients with threatened miscarriage. Yakistiran et al14 compared patients with spontaneous abortion, elective abortion, and healthy pregnant women; contrary to the literature, higher SII, NLR, and PLR values were observed in healthy pregnant women compared with those with spontaneous abortion. In our study, although patients with EPL showed lower SII values than healthy pregnant women, we could not detect a significant relationship between them.
Increased RDW values reflect increased inflammation and oxidative stress.28 Mean platelet volume, PDW, and PCT are considered PLT activation markers.29 Large PLTs with high MPV values cause pregnancy loss by reducing placental perfusion.30 Aynioglu et al31 published that PLT count, PCT, and RDW values were significantly higher in patients with RPL. Regarding the outcomes of the current study, we observed a significant decrease in RDW, PCT, and PDW values in cases with EPL compared to healthy pregnancies. However, no significant difference was detected between the groups regarding MPV values. This result contradicts the idea that PLT activation may play an important role in the pathogenesis of inflammation in EPL.
Study strengths & limitations
This study’s strengths include the large number of participants and the assessment of many inflammatory parameters. Only a few studies have examined the relationship between systemic inflammatory markers and EPL. Lastly, the exclusion of women with possible risk factors that may cause EPL, including advanced maternal age, recurrent miscarriages, chronic diseases, and multiple pregnancies, is another strength of this study. The retrospective study design and lack of power calculation constitute the current study’s limitations.
Currently, there is no effective treatment for EPL. Therefore, prediction of EPL may enable high-risk patients to be offered conservative treatment options. Although our study reports that SIRI can be used to predict EPL, the clinical use of biomarkers is still controversial. These results should be supported by future studies. Future studies combining results from systemic inflammatory markers with maternal risk factors and novel markers may provide further information on predicting EPL.
In conclusion, this study supports the idea that inflammation may play an important role in the etiopathogenesis of EPL. Systemic inflammatory response index may be more useful than other markers derived from CBC predicting EPL in an ongoing pregnancy.
Acknowledgment
The authors gratefully acknowledge enago (www.enago.com), ulatus (www.ulatus.com), and voxtab (www.voxtab.com) for their English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 16, 2024.
- Accepted July 4, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.