


Abstract
Objectives: To investigate the incidence rate, clinical characteristics across different age groups, antimicrobial susceptibility, and outcomes of Elizabethkingia meningoseptica (E. meningoseptica) infections.
Methods: A retrospective analysis was carried out to include 66 cases with confirmed E. meningoseptica cultures from sterile samples between January 2014 and June 2022 at King Faisal Specialist Hospital and Research Centre in Riyadh, Saudi Arabia.
Results: A total of 66 cases were identified, with an incidence rate of 0.3 per 1000 admissions. Most cases were hospital-acquired (80.3%), primarily in critical care areas. All patients had underlying diseases, with respiratory (40.9%) and cardiovascular (39.4%) diseases being the most common. Minocycline showed the highest susceptibility (96.0%), followed by trimethoprim/sulfamethoxazole (77.0%), whereas tobramycin and colistin were fully resistant. The in-hospital mortality rate was 34.8%, whereas the 28-day mortality rate was 22.7%. Clinical characteristics across age groups showed a higher prevalence of cardiovascular disease in pediatrics than in adults, whereas exposure to mechanical ventilation, immunosuppressive therapy, previous infection, anemia, and in-hospital mortality were reported more frequently in adults (p<0.05).
Conclusion: Our study provides valuable insights into E. meningoseptica infection in Saudi Arabia, emphasizing the importance of robust infection control measures. Incidence and mortality rates align with global trends. Variations in clinical characteristics across age groups highlight the importance of tailored treatments based on patient demographics and underlying comorbidities.
Elizabethkingia meningoseptica (E. meningoseptica), formerly recognized as Chryseobacterium meningosepticum or Flavobacterium meningosepticum, is a gram-negative rod characterized by its aerobic, non-motile, non-fermenting nature, absence of spore formation, and multidrug resistance.1 This bacterium is widely distributed in various environmental sources such as water bodies, fish, soils, insects, and amphibians, as well as frequently encountered in healthcare settings, where it can contaminate medical devices and solutions used for flushing.1,2
Currently, the Elizabethkingia genus comprises 6 species: E. meningoseptica, E. miricola, E. anophelis, E. bruuniana, E. ursingii, and E. occulta, with E. meningoseptica being recognized as the most pathogenic among them.2-4
A study by Choi et al5 carried out in South Korea stated that the incidence rate of Elizabethkingia species increased significantly from 0.02 in 2009 to 0.88 in 2017 per 1,000 admissions. In addition, a study by Ma et al6 carried out in China reported a rapid increase in the prevalence rate of E. meningoseptica from 0 in 2011 to 0.19 in 2019 per 1000 inpatients.
Infections associated with E. meningoseptica primarily occur in patients with indwelling medical devices such as mechanical ventilation.5 Being an opportunistic pathogen, E. meningoseptica has the ability to form biofilms, enabling it to endure for prolonged periods in moist or aquatic environments, including tap water.7 Nevertheless, a study by Nori et al8 indicated that E. meningoseptica infection is associated with the COVID-19 virus. Furthermore, some studies have reported that Elizabethkingia species infect not only immunocompromised individuals but also immunocompetent individuals.9-11
Given its significance as a nosocomial pathogen, accurate identification of E. meningoseptica is crucial for clinical diagnosis and subsequent treatment decisions.12 Moreover, due to its inherent resistance to commonly used antibiotics such as aminoglycosides and β-lactams, E. meningoseptica infections pose a significant challenge in terms of treatment, often resulting in high mortality rates.1,13
In Saudi Arabia, limited studies have been published regarding E. meningoseptica infection, and the majority were case reports, case series, or investigations with relatively small sample sizes.4,14-20 Therefore, this study reports a considerable number of cases with E. meningoseptica infection over nearly 9 years (2014-2022). The study aims to explore several key aspects related to E. meningoseptica, including the incidence rate, clinical characteristics, antimicrobial susceptibility, and outcomes of E. meningoseptica infections at a tertiary care center in Saudi Arabia.
Methods
This retrospective single-center study was carried out at King Faisal Specialist Hospital & Research Centre in Riyadh, Saudi Arabia. It is a tertiary referral hospital offering general and highly specialized inpatient and outpatient medical treatment, transplantation, and oncology services.
All patients, with a confirmed culture of E. meningoseptica from sterile samples, including blood, drainage fluid, tracheal aspirate, urine, vascular tip, and wound culture, between January 2014 and June 2022 were included in the study. Both pediatric and adult patients were included. In our hospital practice, the pediatric population comprises individuals up to 14 years of age, while adults are defined as those aged above 14 years. Patients with missing documentation were excluded.
The study was carried out in accordance with the Declaration of Helsinki, and approved by the ethics committee of King Faisal Specialist Hospital and Research Centre, Riyadh, Saudi Arabia (reference number: 2231011 and date of approval: 19/01/2023).
Data were gathered by chart review and then stored in REDCap (10.8.0 - © 2021 Vanderbilt University). The extracted data included demographic information, medical history, investigations, clinical manifestations, diagnosis, antibiotic susceptibility, and outcomes.
Hospital-acquired or healthcare-associated infection was documented if it occurred >48 hours after admission to the healthcare facility.21 In addition, previous infection, antimicrobial use, and interventions such as ventilation were defined as occurring within 30 days prior to Elizabethkingia infection.
Elizabethkingia species were identified using the VITEK® 2 (bioMérieux, located in Marcy-l’Étoile, France). Gram-Negative Card 292 was used to determine antibiotic susceptibility. The Clinical and Laboratory Standards Institute (CLSI M100) recommendations were used to interpret zone dimensions for classification as susceptible, intermediate, or resistant.22
Furthermore, leukopenia was defined as white blood count <4.5×109/L, thrombocytopenia as platelet count <150×109/L, neutropenia as an absolute neutrophil count <1.5×109/L, and anemia as hemoglobin (Hb) concentration <12.5 g/dL in adults, <11 g/dL in children aged 6 months to 6 years, and <12 g/dL in children aged 6-14 years.
Statistical analysis
Data analysis was carried out using STATA, version 18 (College Station, TX: StataCorp LLC). Categorical variables were reported as frequencies and percentages (%), and continuous variables as medians and interquartile ranges (IQRs) due to a lack of normality assumption using the Kolmogorov-Smirnov test. In addition, Fisher’s exact test was used to compare clinical characteristics across age groups (pediatrics age ≤14 years versus adults age >14 years). Graphs were generated in Microsoft Excel 2016.
Results
A total of 66 patients with E. meningoseptica infection were identified from January 2014 to June 2022, with overall incidence rate of 0.3 per 1000 admissions (66/204,426), the peak incidence was noted in 2016 with a rate of 1 per 1000 admissions (20/20,514), then it was gradually decreased to 0.1 per 1000 admissions in June 2022 (2/22,625, Table 1). Of these, 31 (47.0%) were females. Regarding age, 35 (53.0%) were pediatrics (aged ≤14 years) with a median age of 0.4 years (IQR: 0.25-2), and 31 (47.0%) were adults (aged ≥15 years) with a median age of 51 years (IQR: 36-62, Table 2).
- The incidence of Elizabethkingia meningoseptica over the years (2014-mid 2022).
- Characteristics of study participants (N=66).
The origin of infection indicated that 13 (19.7%) cases were community-acquired, whereas the majority (53 [80.3%] cases) were hospital-acquired. Among hospital-acquired infections, the majority (98.1%) occurred in critical care areas such as the intensive care unit (ICU), operating room (OR), or emergency room (ER, Table 2).
Many patients had previous hospitalization (72.7%), infections (57.6%), and antimicrobial use (83.3%) within one month prior to E. meningoseptica infection (Table 2).
Remarkably, all 66 patients had underlying diseases (100%). The most reported primary diagnosis was respiratory disease (40.9%), followed by cardiovascular disease (39.4%), immunodeficiency, and liver disease (24.2%), hematological/oncological diseases (21.2%), and renal disease (18.2%). Furthermore, 10.6% had a stem cell transplant, and 19.7% had a solid organ transplant. Immunocompromising therapies such as immunosuppressant therapy was reported in 30.3% and chemotherapy was reported in 10.6% of patients (Table 2).
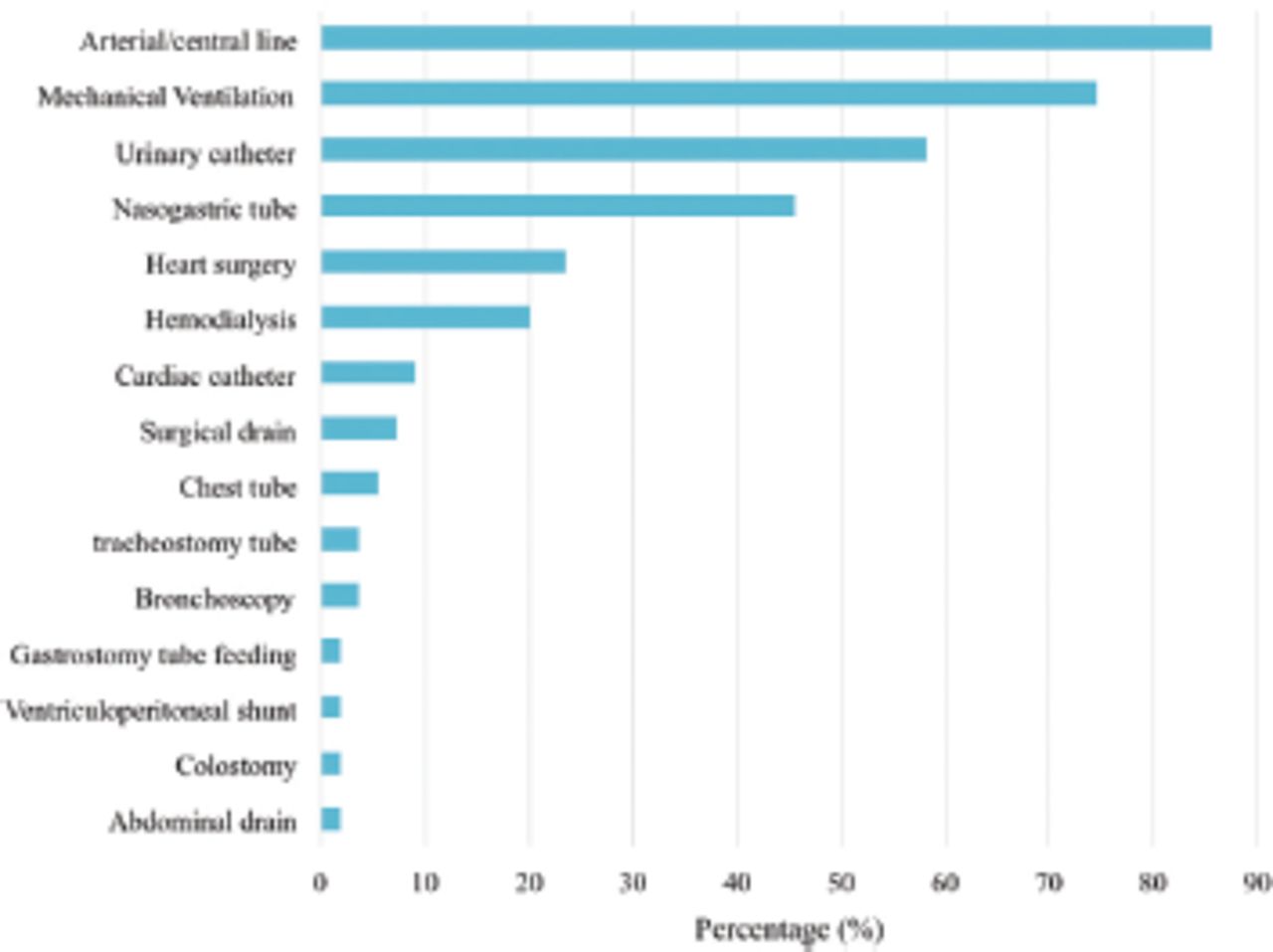
Moreover, 55 of the 66 (83.3%) patients had received previous interventions within one month before the episode; of them, 85.4% had arterial/central line insertion, 74.5% were on mechanical ventilation, 58.2% had urinary catheterization, 45.4% had nasogastric tube placement, 23.6% underwent heart surgeries, 16.4% were on hemodialysis, and 9.1% underwent cardiac catheterization (Figure 1).

- Previous interventions within one-month prior the infection (n=55).
Of the total cases, 7.6% had E. meningoseptica colonized infection, whereas the majority (92.4%) presented with an active infection. Among the active infection cases, various symptoms were reported, with fever being the most common (32.8%), followed by respiratory distress (45.9%), tachycardia (34.4%), hypotension (23%), lethargy (18%), and gastrointestinal symptoms (6.6%, Table 2).
The most common source used in isolating E. meningoseptica in our series was tracheal aspirate (77.3%). Furthermore, 42 (63.6%) patients had polymicrobial infections at the time of the episode; of them, 40 (95.2%) had a bacterial infection, including gram-positive bacterial infection in 6 patients (Enterococcus, Staphylococcus) and gram-negative bacterial infection in the remaining 36 patients (gram-negative rods, Pseudomonas, Stenotrophomonas, Acinetobacter, Enterobacter, Chryseobacterium, Escherichia coli, Klebsiella, and Serratia). Lastly, 12 (28.6%) patients had a fungal infection (Candida species). Notably, 10 patients had both fungal and bacterial infections (Table 3).
- Investigations and hospital course.
Laboratory results revealed a high prevalence of anemia (81.8%) and thrombocytopenia (48.5%). Elevated procalcitonin levels (>0.25 ng/mL) were observed in 53.5% of cases, whereas C-reactive protein (CRP) levels (>50 mg/L) were elevated in 27.3% of cases (Table 3).
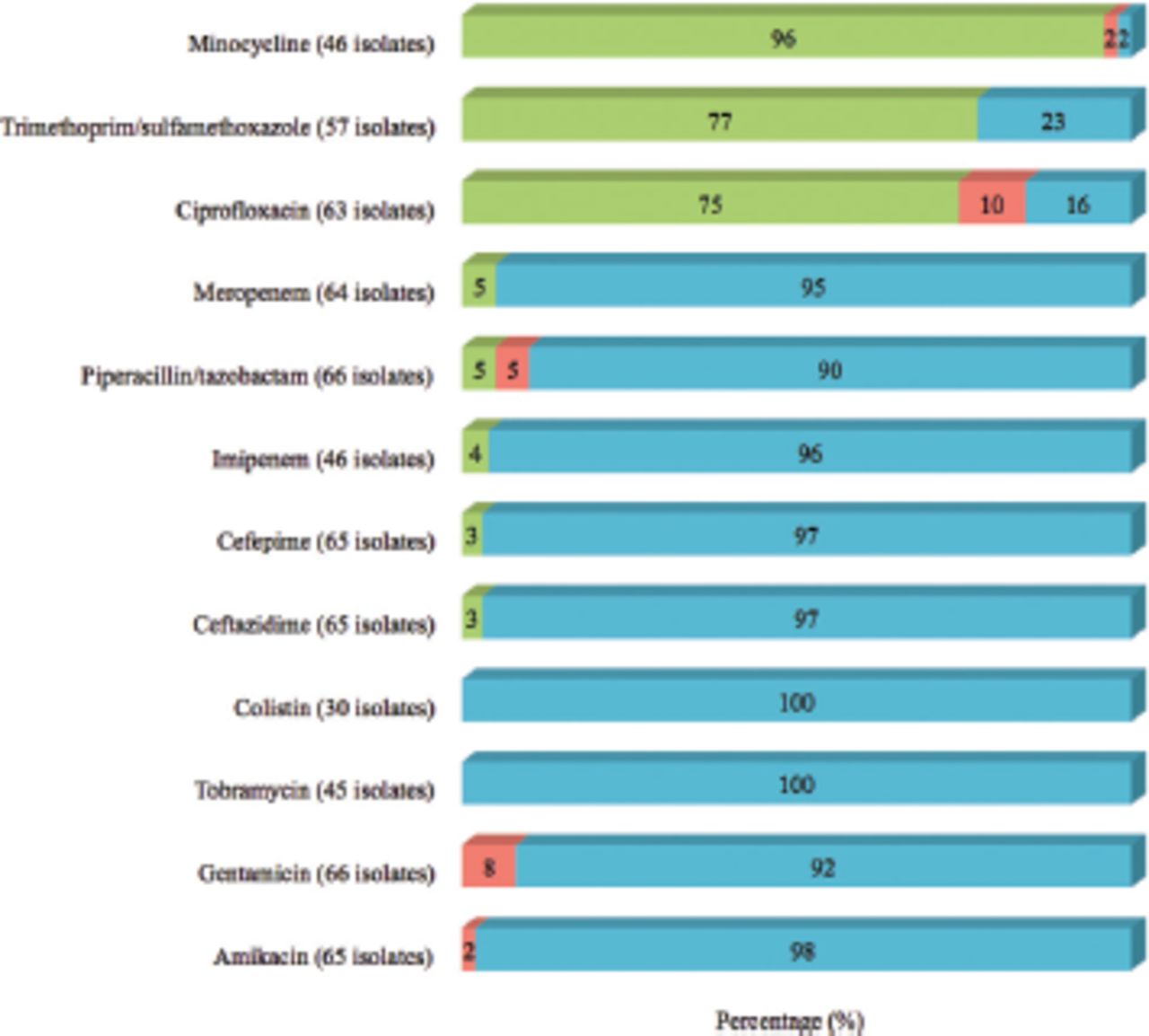
In terms of antibiotic susceptibility, minocycline had the highest susceptibility (96.0%), followed by trimethoprim/sulfamethoxazole (77.0%) and ciprofloxacin (75.0%). In contrast, E. meningoseptica was resistant to most antibiotics, including tobramycin (100%), colistin (100%), amikacin (98%), ceftazidime (97%), cefepime (97%), imipenem (96%), meropenem (95%), gentamicin (92%), and piperacillin/tazobactam (90%, Figure 2).

- The antibiotic susceptibility of Elizabethkingia meningoseptica isolates.
A total of 43 (65.2%) patients received targeted antimicrobial treatment for the episode, with a median treatment duration of 20 days (IQR: 14-29). The most prescribed antimicrobial agents were ciprofloxacin (46.5%) and trimethoprim/sulfamethoxazole (23.3%) (Table 3).
Outcomes varied, with 59.1% of patients recovering, 34.8% succumbing to the infection, 3.0% exhibiting a relapse infection (while on treatment), and 3.0% exhibiting recurrence of the infection within one month. The in-hospital mortality rate was 34.8% (23/66 patients), with a median duration of 17 (IQR: 5-41) days from infection to death. The 28-day mortality rate was 22.7% (Table 3).
The majority of clinical characteristics did not significantly differ across age groups. However, cardiovascular disease was twice as high in pediatrics than in adults (51.4% vs. 25.8%; p<0.05), whereas exposure to mechanical ventilation (80.6% vs. 45.7%), immunosuppressive therapy (51.6% vs. 11.4%), previous infection (74.2% vs. 42.9%), anemia (93.5% vs. 71.4%), and in-hospital mortality (54.8% vs. 17.1%) were more frequently reported in adults than in pediatrics (p<0.05, Table 4).
- Clinical characteristics by age group (N=66).
Discussion
The emergence of E. meningoseptica as a significant nosocomial pathogen has raised concerns globally, particularly due to its inherent resistance to common antibiotics and association with high mortality rates. This retrospective study, carried out over nearly 9 years, aimed to shed light on various aspects of E. meningoseptica infection, including its incidence rate, clinical characteristics, antimicrobial susceptibility, and mortality rate.
The study highlights the clinical importance of E. meningoseptica infections, with an overall incidence rate of 0.3 per 1000 admissions, mainly being hospital-acquired. Interestingly, the highest incidence rate was observed in 2016 (1 per 1000 admissions), then gradually decreased to (0.1 per 1000 admissions) in mid-2022, which could be explained by the increase of infection control precautions in our center post-COVID-19. Thus, our overall incidence rate aligns with those of similar studies reporting annual incidences of E. meningoseptica ranging from 0.007-0.399 cases per 1,000 admissions.23,24 Moreover, Choi et al5 stated that the incidence rate of Elizabethkingia species increased significantly from 2009 (0.02) to 2017 (0.88) per 1,000 admissions during 2009-2017, with mechanical ventilation being a significant risk factor. Similarly, in our study, a significant proportion of adult patients had a history of prior mechanical ventilation exposure (within one month prior to the infection).
Demographic and clinical characteristics of patients with E. meningoseptica infection revealed that pediatrics comprised a substantial portion of the series, with respiratory and cardiovascular diseases being the most prevalent underlying conditions in this population.
Moreover, previous studies have reported that the majority of patients with Elizabethkingia infections have underlying chronic conditions such as diabetes, cardiovascular disease, malignancy, renal disease, and liver cirrhosis.25 Additionally, cardiovascular disease was significantly associated with E. meningoseptica infection in the pediatric group in this study, whereas previous infection, immunosuppressive therapy, and anemia were significantly reported in adult patients. This emphasizes the need for heightened surveillance and infection prevention strategies among high-risk populations.
Additionally, a significant proportion of patients had a history of previous hospitalization, infections, and antimicrobial use within one month prior to the E. meningoseptica infection. Moreover, most cases in the study had an active infection, with only 7.6% having a colonized infection of E. meningoseptica. In contrast, a retrospective study by Alyami et al4 investigated Chryseobacterium/Elizabethkingia species infections in 27 patients at Prince Sultan Military Medical City in Riyadh, Saudi Arabia, and reported a hospital-acquired infection in 92.5%, colonization rate in 22.2%, previous hospitalization within 90 days prior to the infection in 33.3%, and a 28-day mortality rate of 11.0%. The reason for the difference in findings could be that most of our patients were critically ill and had previously underwent multiple hospitalizations.
Moreover, laboratory investigations demonstrated common hematological abnormalities such as anemia and thrombocytopenia, along with elevated inflammatory markers. Similarly, a retrospective study by Li et al26 investigated E. meningoseptica infections among 24 patients at a tertiary care center in China and reported anemia in 75%, hypoproteinemia in 75%, elevated CRP in 66.7%, neutrophilia in 54.2%, and leukocytosis in 50.0%. These findings are indicative of the systemic nature of E. meningoseptica infections.
The antimicrobial susceptibility profile in this study revealed limited treatment options, with some variability observed in the susceptibility of different antibiotics. Notably, minocycline and trimethoprim/sulfamethoxazole showed the highest susceptibility, suggesting their potential utility in the management of E. meningoseptica infections. Furthermore, the antibiotic resistance profile of Elizabethkingia spp. is characterized by intrinsic resistance to several antibiotic classes due to the presence of unique metallo-β-lactamases (MBLs) and extended-spectrum β-lactamases (ESBLs).27-29 Notably, Elizabethkingia spp. possess multiple chromosomally encoded MBLs, distinguishing them from other bacteria.30 Reports indicate resistance to β-lactams, aminoglycosides, macrolides, and vancomycin, with variable susceptibility to other antibiotics such as fluoroquinolones, tetracycline, and trimethoprim-sulfamethoxazole.2,28,31-33 However, susceptibility testing is challenging due to the lack of established minimum inhibitory concentration breakpoints, necessitating alternative methods such as broth microdilution for accurate determination.2,13 Despite anecdotal success with vancomycin, its efficacy is uncertain, prompting recommendations for combination therapy involving ciprofloxacin, linezolid, or rifampicin.13 Whole-genome sequencing has revealed a multitude of antibiotic resistance genes in Elizabethkingia spp., offering insights into their resistance mechanisms.28,29 Nevertheless, genomic studies from the Middle East on Elizabethkingia spp. are lacking, highlighting the need for further research in this region.
Despite treatment efforts, the 28-day mortality rate in this study was 22.7%, and the in-hospital mortality rate was 34.8%. Notably, the in-hospital mortality was significantly higher in adults, highlighting the challenges in managing this pathogen among adult patients. Similarly, Seong et al34 reported a 28-day mortality rate of 25.2% among patients with Elizabethkingia infections, with a mean age of 66.5 years in their study cohort. Moreover, a systematic review by Ma et al6 revealed that the fatality rate associated with E. meningoseptica infection varied between 11.0-66.6%. After accounting for the influence of limited sample size, mortality rates fell within the range of 23.4-65.6% across 5 studies encompassing over 30 patients.6 However, it is unclear whether E. meningoseptica infection or the underlying disease was the cause of death in our study and other studies.
Thus, the comparison of clinical characteristics across age groups revealed some interesting differences, particularly in the prevalence of cardiovascular disease and the utilization of mechanical ventilation and immunosuppressive therapy. These findings underscore the importance of tailoring treatment approaches based on patient age and underlying comorbidities.
Study limitations
Although this study reported a considerable number of E. meningoseptica infection cases, its retrospective and single-center design inevitably constrain its generalizability.
In conclusion, our study provides valuable insights into the epidemiology and clinical characteristics of E. meningoseptica infections at a tertiary care center in Riyadh, Saudi Arabia. Aligning with global trends, the incidence rate of E. meningoseptica infection in this study was 0.3 per 1000 admissions, with most cases being hospital-acquired, emphasizing the importance of robust infection control measures. Laboratory investigations revealed common hematological abnormalities and elevated inflammatory markers, indicative of the systemic nature of E. meningoseptica infections. Antimicrobial susceptibility testing revealed limited treatment options, including trimethoprim/sulfamethoxazole or minocycline, highlighting the challenges in managing these infections. The mortality rates were substantial, aligning with the findings of other studies, particularly among adults. Variations in clinical characteristics across age groups highlight the importance of tailored treatment approaches based on patient demographics and underlying comorbidities. Further research, particularly genomic studies, is warranted to better understand the antibiotic resistance mechanisms and improve treatment strategies for E. meningoseptica infections in the Middle East region.
Acknowledgment
The authors gratefully acknowledge the ContentConcepts company for their English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received April 1, 2024.
- Accepted July 4, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.