


Abstract
Objectives: To investigate the long-term effects of Extracorporeal shockwave therapy (ESWT) and ultrasound (US) in treating the trigger finger. Trigger finger, also known as stenosing tenosynovitis, is a common type of tenosynovitis affecting the flexor sheath of any finger. Extracorporeal shockwave therapy and therapeutic US are conservative treatments that use waves of varied frequency to target damaged regions and improve function.
Methods: This cohort study was carried out in Saudi Arabia, using samples obtain from the files of patients with trigger fingers who visited the orthopedic department at Al-Rass General Hospital between May and June 2023. Of the 38 people with trigger fingers who were initially included, 24 satisfied the requirements for inclusion (11 underwent US, and 13 received ESWT). Assessments were conducted in September 2023, two months later. A goniometer was used to measure the range of motion (ROM), an electrical dynamometer was used to test grip strength, a numerical pain rating scale was used to quantify discomfort, and QuickDASH was used to measure general functional capacity.
Results: Extracorporeal shockwave therapy and US significantly affected all outcomes, including pain severity, ROM, hand strength, and general functional capability (p<0.005). In the immediate period, the US outperformed ESWT in enhancing general functional capability. Over time, ESWT was more essential for reducing pain (p=0.001).
Conclusion: This study provides preliminary evidence that ESWT and US have similar effects in treating trigger fingers.
Trigger finger is a common issue in physiotherapy clinics.1 It is distinguished by discomfort, clicking, catching, and a lack of mobility in the afflicted finger, produced by inflammation and subsequent constriction in the pulleys that keep the flexor tendons tight to the finger bones during flexion and extension.2 The most common pulley effect is the A1 pulley, positioned at the base of each digit where the finger meets the palm.3 Trigger finger is more common in diabetics and women, particularly in their fifth and sixth decades.4,5 There are several trigger finger treatments available, depending on how severe the disease is. Both open and closed-incision surgical procedures can be used to address chronic symptoms.6 Patients who seek medical attention shortly after the beginning of symptoms are advised to get conservative therapy for acute instances.7 Orthoses, physical therapy methods, local corticosteroid injections, and anti-inflammatory drugs are examples of conservative therapies.8-10 Recently, extracorporeal shockwave therapy (ESWT) and therapeutic ultrasound (US) have emerged as viable alternatives to surgical treatment of musculoskeletal problems.11,12 Extracorporeal shockwave therapy, a management technique used in physiotherapy, involves directing high-amplitude sound waves toward the treatment location. This mechanism boosts local blood flow and neovascularization, thereby having a therapeutic impact on function and discomfort.13 In contrast, sound waves produced by the US generate micro-vibrations in the tissues, producing heat energy that increases blood flow in the treated region and raises the levels of essential chemicals and oxygen for healing.14
In recent years, numerous studies have examined the efficacy of ESWT and US in treating a variety of pathologies, including plantar fasciitis, lateral epicondylitis, Achilles tendinopathies, carpal tunnel syndrome, shoulder pathologies, myofascial pain syndrome, and spasticity.15-21 However, no study has evaluated the effects of these modalities on the trigger finger nor defined specific criteria and techniques for their use. There are also no guidelines to determine whether ESWT is superior to the US as a conservative treatment for trigger fingers or vice versa. There is a scarcity of research comparing the effectiveness of ESWT and US for treating trigger fingers. The present study aims to compare the long-term effectiveness of ESWT and US for treating trigger fingers.
Methods
This cohort study was conducted at Alrass General Hospital in Saudi Arabia and was approved by the Regional Research Ethics Committee. The study was carried out from July 2023 to September 2023, with samples collected from patients with trigger fingers who visited the orthopedic clinic between May 2023 and June 2023. Previous study considered in the study were discovered using PubMed, ResearchGate, and Google Scholar.
Participants were included if they: Were diagnosed with trigger fingers using Quinnell’s (1980) classification as follows: 0 (normal finger movements), 1 (uneven finger movement), 2 (actively correctable triggers), 3 (passively correctable triggers), and 4 (non-correctable locked fingers), underwent evaluations by a senior physiotherapist for musculoskeletal disorders during pre-treatment, after 5 sessions, and after 10 sessions. These evaluations used the numeric pain rating scale (NPRS), a goniometer to evaluate range of motion (ROM), an electrical dynamometer to test grip strength, and QuickDASH to assess general functional capability, completed 10 sessions of ESWT (2,500 impulses, 1.4 bar, 10 Hz, head diameter 2 cm) or US (1.0 MHz, 70% duty cycle, 6 min, head diameter 3.5 cm) over 5 weeks, in addition to isometric, ball, and rubber band strength training, were at least 18 years old, and had never undergone surgery before.
The exclusion criteria were under the age of 18, using alternative evaluation techniques, not finishing their session, or having other bone diseases, such as osteomyelitis, rheumatoid arthritis, systemic inflammatory disease, an active infection around the hand or wrist, or anticoagulant medication for vascular or neurological failure.
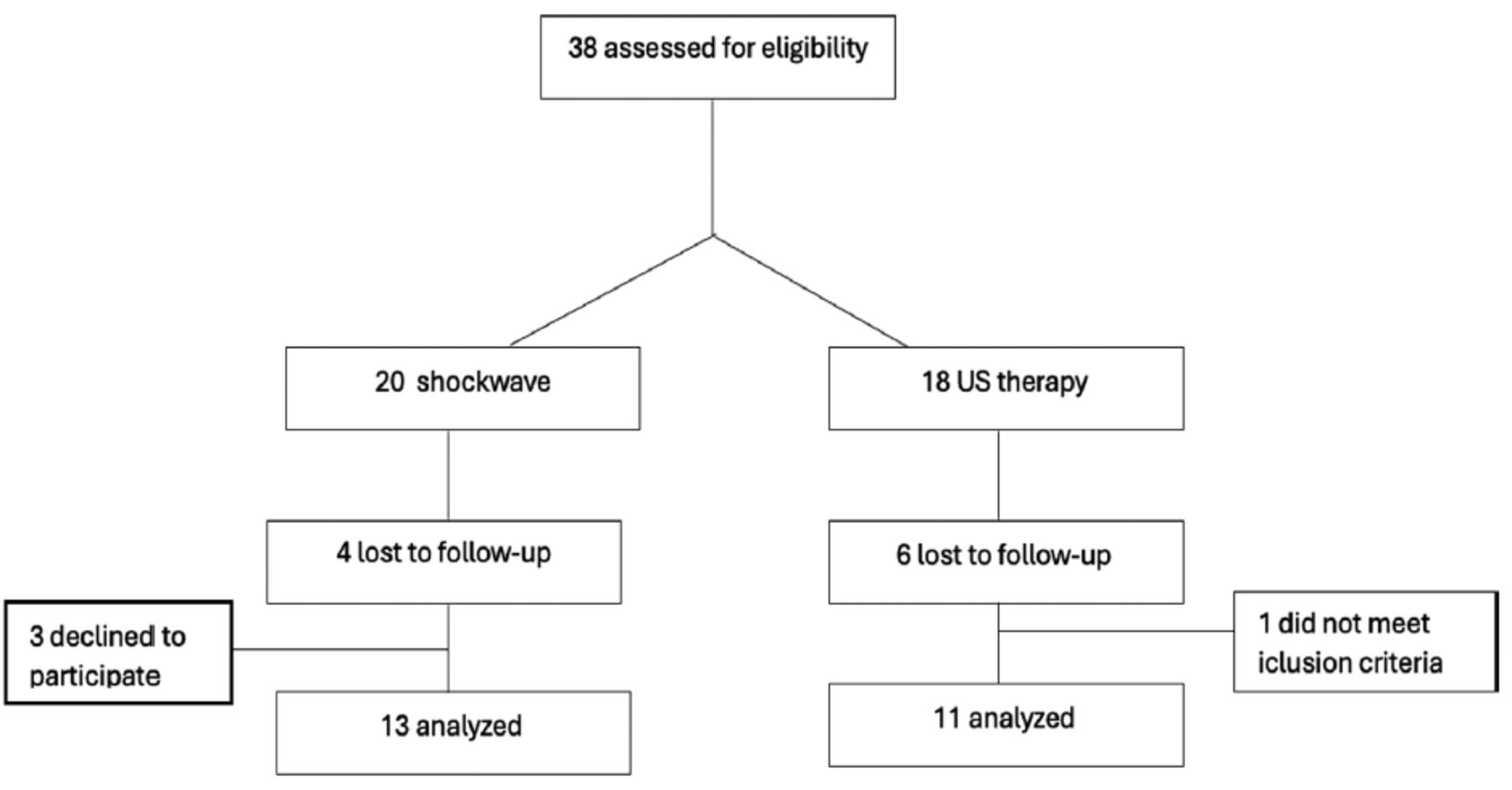
An initial inclusion of 38 individuals over the age of 18 years with trigger fingers was made. Four individuals who had undergone procedures were excluded, leaving 34 participants who had never undergone procedures. Of these, 20 participants underwent ESWT, with 4 lost to follow-up, and 18 underwent the US, with 6 lost to follow-up. Twenty-four participants completed the treatment; 13 underwent ESWT and 11 underwent US. Additionally, all participants were evaluated after 5 and 10 sessions. All individuals who met the criteria for participation were initially informed of the study’s aim, methods to be adapted, and evaluations to be made in written and verbal form. Furthermore, each participant was asked to fill out the approval form to be part of the study.
The first group underwent the US, which was made in Italy, whereas the second group underwent ESWT, which was made in Germany. Therapists administered isometric, ball, and rubber band strength training regimens to both groups. All groups were subjected to 10 sessions of ESWT (2,500 impulses, 1.4 bar, 10 Hz, head diameter 2 cm) or US (1.0 MHz, 70% duty cycle, 6 min, head diameter 3.5 cm) over 5 weeks. Ultrasound gel was used to transmit the ESWT and US signals to the patient’s skin. The treatment posture involved the patient sitting with their elbow flexed at 90°, shoulder adducted beside the body, and forearm supinated (Figure 1).

- The figure illustrates the treatment techniques provided with parameters as following: A) Extracorporeal shockwave therapyparameter: 2,500 impulses, 1.4 bar, 10Hz, head diameter 2cm. B) Ultrasound parameter: 1.0MHz, 70% duty cycle. 6 min., head diameter 3.5 cm. C,D) The treatment posture: patients sitting with their elbow flexed 90 degrees, shoulder adducted beside their body and forearm in supination.
A senior specialist physiotherapist assessed each participant. The NPRS, which goes from 0 (no pain) to 10 (worst possible agony), was used to measure pain. A goniometer was used to measure the range of motion. An electrical dynamometer was used to test grip strength, and the QuickDASH questionnaire was used to measure general functional capability
Statistical analysis
Data were analyzed using the SPSS Statistics for Windows, version 26 (SPSS Inc., Chicago, Ill., USA)’. Variables are presented as means and standard deviations (SD). Before the start of the trial, demographic information and data regarding each participant’s disease were extracted from their files and statistically analyzed. The Chi-square test was employed to determine the relationship between categorical variables, whereas the Mann-Whitney U test was utilized for continuous data. A paired sample t-test was performed to examine the individuals’ outcome measurements, pain ratings (NPRS), general functional capacity (Quick-DASH), joint ROM, and grip strength by comparing baseline data with data collected after 5 and 10 sessions. An independent sample t-test was utilized to evaluate pain intensity, ROM, and overall functional capability between the 2 modalities for the short-term effect (data gathered from patients’ files) and long-term evaluation (2 months later). Statistical significance was set at p<0.05.
Results
This study comprised 38 patients with trigger fingers; 24 finished their sessions and received either ESWT (n=13) or US (n=11) (Figure 2). Table 1 presents baseline demographic data as well as illness characteristics specific to each group. The 2 groups had no statistically significant differences at the start of therapy (p>0.05).

- CONSORT flow diagram for extracorporeal shockwave therapy and ultrasound groups.
- Descriptive analysis of demographic and baseline characteristics for the extracorporeal shockwave therapy and ultrasound groups.
In terms of the immediate results, both the ESWT and the US groups showed a significant improvement (p<0.05 in all outcomes [pain severity, proximal interphalangeal [PIP] joint ROM, distal interphalangeal [DIP] joint ROM, hand strength, and general functional capability) after 5 therapy sessions. After 5 sessions, the US revealed a statistically significant difference in general functional capability (p=0.001) compared to ESWT (p=0.38). When comparing the results after 10 sessions to pre-treatment measurements, both ESWT and US significantly impacted all measures (p<0.05), except for the metacarpophalangeal (MP) and interphalangeal (IP) joints, which showed only minor improvement in the thumb ROM even after 10 sessions (Tables 2 & 3).
- Comparison of pretreatment and posttreatment of the shockwave group.
- Comparison of pretreatment and posttreatment of the ultrasound therapy group.
During the treatment period, there were no statistically significant differences between the 2 modalities. However, after 2 months of therapy or over the long term, ESWT demonstrated efficacy in reducing pain and hand strengthening. In short-term outcomes, the US was more effective in improving general functional capability, but there was no statistically significant difference between the 2 modalities after 2 months of therapy in ROM and general functional capacity (Table 4).
- Comparison of pretreatment, posttreatment, and 2-month measurements of the therapeutic group.
Discussion
The aim of this study is to evaluate the long-term efficacy of US therapy and ESWT in treating patients with trigger fingers. To achieve this, evaluations of general functional capacity, range of motion, grip strength, and pain severity were conducted before treatment, after 5 sessions, after 10 sessions (data were acquired from patient files), and 2 months following treatment (assessed during the study). All outcomes, including pain intensity, PIP and DIP joint range of motion, hand strength, and overall functional capacity, were found to be impacted by both ESWT and US. Despite this, the MP and IP joints showed only a slight increase in ROM, even after 10 sessions. In terms of short-term impacts, the US was more effective than ESWT in enhancing general functional capability. However, over time, no difference was observed between the 2 modalities, except ESWT was notably effective in reducing pain and hand strength. Related study by Dogru et al,22 patients with second-grade trigger fingers, as defined by the Quinnell classification, can benefit from 10 sessions of radial ESWT (rESWT) in terms of range of motion, grip strength, pinch strength, and general function capability. Additionally, ESWT has proven effective in treating a variety of tendinopathies, including calcific shoulder tendinopathies, plantar fasciitis, lateral elbow epicondylitis, hamstring tendinopathy, and patellar tendinopathy.23-27 In a study by Vahdatpour et al,28 ESWT is effective in reducing the intensity of triggering, enhancing function up to 18 weeks after the intervention, and lowering the level of pain.28 Malliaropoulos et al,29 discovered a significant decrease in the intensity of pain and an enhancement in functional levels. In contrast, one randomized controlled trial compared the effectiveness of corticosteroid injections and physiotherapy, which included 10 sessions of US, wax therapy, massage, and stretching exercises. This study used various measures, such as a visual analog scale, the number of triggering events, hand grip, hand function, and patient satisfaction, and found that corticosteroid injection provided an increased rate of pain relief, a reduction in the average number of triggering events, improved hand grip, and enhanced patient satisfaction at 3 months post-management.30 In the current study, US was shown to reduce pain, improve ROM, and enhance general functional capacity, similar to the effects observed with ESWT.
However, directly comparing the results of the current study with those of previous studies is challenging due to the differences in the devices used, treatment parameters, application methods, and follow-up procedures. Additionally, there are no standardized guidelines for the number of sessions or specific parameters required for ESWT or US to treat soft tissue conditions.
Study limitations
This cohort study was conducted in Saudi Arabia to compare the US and ESWT as conservative treatments for trigger fingers. However, several limitations of the current study should be noted. Firstly, patients included in this study had prior symptom durations as short as one month, whereas most previous studies on ESWT and US which only looked at its efficacy for more chronic tendinopathies, focused on chronic tendinopathies with symptom durations of at least 6 months. Secondly, the study did not include a control group, and all patients received the same amount of treatment. Lastly, the study used a small sample size. To guarantee external validity, a control series of studies will be conducted in the future.
In conclusions, this study demonstrates the effectiveness of ESWT and US in treating trigger fingers, evidenced by pain relief, increased ROM, and enhanced functional capacity. Improvements began after 5 treatment sessions and continued for 2 months, with ESWT showing superior long-term benefits in pain relief and hand strength enhancement compared to the US. Both modalities were equally effective in improving functional capacity over the long term. To further validate these findings, the efficacy of ESWT and US should be demonstrated in randomized controlled trials.
Acknowledgment
We are very grateful to Alrass General Hospital for supporting this research, and We would like to thank Editage (www.editage.com)for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received July 27, 2024.
- Accepted November 26, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.



{kind=link}
{kind=link}