


Abstract
Objectives: To investigate epidemiological changes in respiratory fungal infections (RFI), including fungal isolation and colonization, at one of the main centers in Medina. The incidence of RFI is rising due to an increase in the number of immunocompromised individuals, a higher prevalence of respiratory viral infections, and an aging population.
Methods: A retrospective cross-sectional study was conducted by extracting data of patients with fungal-positive respiratory cultures from King Fahad Hospital (KFH), Al Madinah Al Munawwarah from 2013 to 2023.
Results: A total of 352 episodes of fungal-positive cultures were identified in 79 patients, reflecting a 12-fold increase in RFI prevalence. The most frequent fungus was Candida albicans 43% (n=150), followed by C. tropicalis at 34% (n=119), C. glabrata at 7% (n=25), C. parapsilosis at 5% (n=18), C. dubliniensis at 3.4% (n=12), and Aspergillus fumigatus at 3.4% (n=12). Bronchoalveolar lavage was performed 52 times, with 19 cultures growing C. albicans and 8 cultures positive for A. fumigatus. None of the 58 lung biopsy samples grew mold. Only one patient had 2 C. glabrata isolates resistant to voriconazole and fluconazole. The most prevalent comorbidities were respiratory diseases (30%) and lower limb injuries and diabetes (16%).
Conclusion: Candida albicans was the leading cause of RFI. Continuous monitoring, improved diagnostics, and targeted interventions are crucial to address existing challenges and emerging threats. The growing recognition of fungal infections necessitates increased research and education for healthcare professionals.
The vast terrain and diverse climate of Saudi Arabia have long shaped its unique epidemiology, including patterns of infection. While bacterial and viral respiratory illnesses have historically dominated, recent years have seen a concerning increase in the prevalence and nature of respiratory fungal infections (RFIs) and fungal isolation.1,2 This transformation necessitates a closer examination to understand its causes, implications, and necessary responses. Several factors are believed to be driving this shift, including increased awareness and improved diagnostic techniques, particularly for infections caused by Candida and Aspergillus species.3 The adoption of advanced bronchoscopy procedures and more sensitive culture methods has revealed fungal infections that might have previously gone undetected. Additionally, changes in healthcare practices, such as the widespread use of broad-spectrum antibiotics and immunosuppressive therapies, have created an environment conducive to the growth of opportunistic fungal pathogens. The rising immunocompromised population, driven by increasing rates of chronic diseases like diabetes and cancer, further contributes to the susceptibility to fungal infections. Environmental factors specific to the region also cannot be overlooked.4,5 The arid climate of Saudi Arabia, characterized by dust storms, provides a reservoir for fungal spores, facilitating their inhalation and subsequent colonization of the respiratory tract. Rising temperatures in the region may also favor the proliferation of certain fungal species. Moreover, the growing influx of pilgrims to Medina exposes the local population to diverse fungal strains carried by visitors from worldwide. Accurate global data on RFI are lacking due to limited data collection and reporting, diagnostic challenges, and variations in fungal species and infection severity. There are few case reports from Saudi Arabia. However, the vulnerability of the nation’s population to RFI is rising, particularly among individuals with diabetes, lower respiratory infections, and chronic kidney disease.6 The average lifespan of Saudis is expected to increase by 5.3 years for both males and females based on the country’s 1990–2010 birth expectancy.7,8 In this study, we investigated the epidemiological features of RFI at King Fahad Hospital (KFH), Al Madinah Al Munawwarah’s largest hospital. This study explores the reasons behind this shift, its potential consequences and observes the dynamic phenomenon of RFI.
Methods
The General Directorate of Health Affairs in Al Madinah Al Munawwarah, Ministry of Health, Saudi Arabia’s local Institutional Review Board granted approval for this study. Because the study was observational retrospective, the committee decided not to require informed consent.
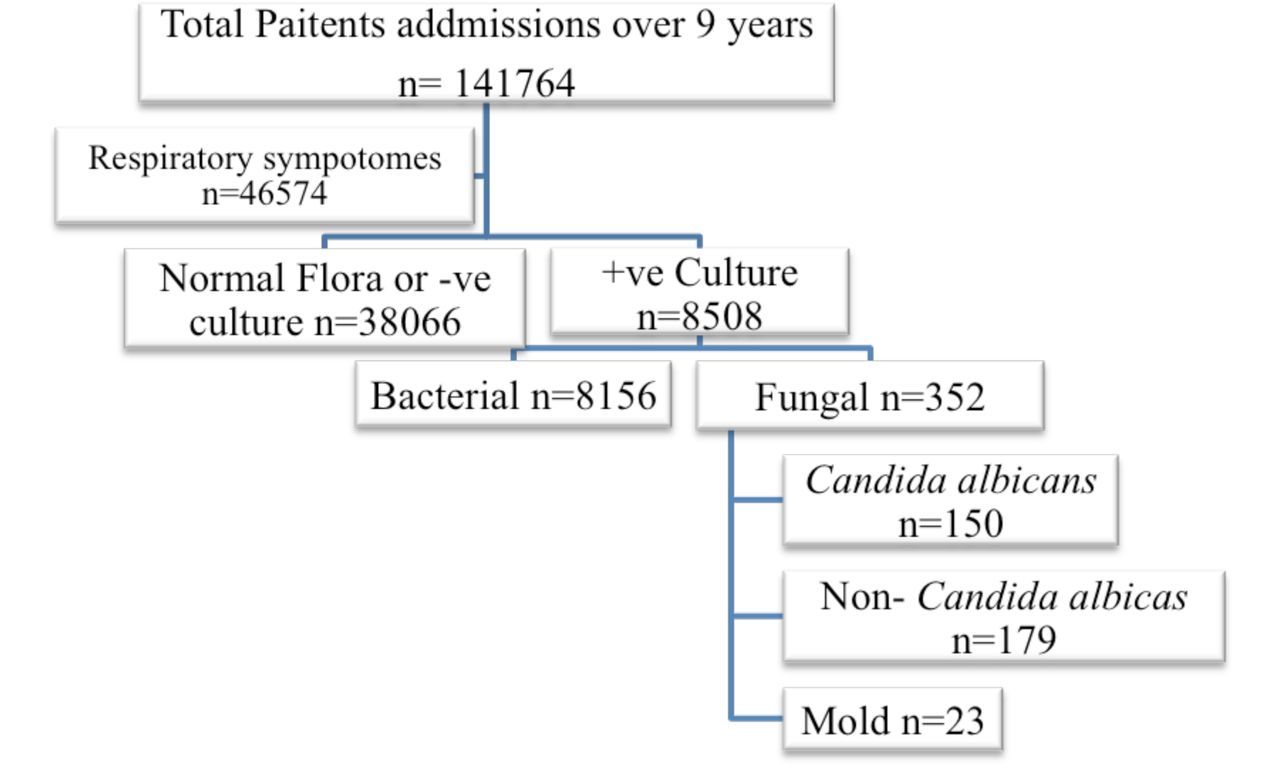
From July 2013 to December 2023, patients with positive fungal respiratory cultures from every department were included (Figure 1). Patient demographics, initial diagnoses, age, comorbid illnesses, species identification, and the outcomes of antifungal susceptibility testing were among the information taken from the KFHM database. The European Organization for Research and Treatment of Cancer/Mycoses Study Group (EORTC/MSG) criteria were used to classify cases. Any pathogenic fungal species isolated from at least one culture specimen in a patient exhibiting infection-related symptoms (fever, x-ray findings, cough, shortness of breath) was considered an episode of respiratory infection. Each admission was considered a new episode if a patient had more than one (Figure 1).

- Flow diagram of the study design and selection criteria. The year 2013 had no fungal positive cultures that met the study criteria.
Laboratory techniques for microbiology
As soon as the symptoms of a respiratory infection were noticed, sputum and bronchoalveolar lavage (BAL) samples were subjected to laboratory diagnosis. Gram staining was used to directly analyze the samples, which were then cultivated both aerobically and anaerobically on Sabouraud Dextrose Agar (SDA) plates and incubated in a mycology incubator at 25–30°C for up to 3 weeks. Germany’s Forma Scientific Incubators were used. When pure isolation of pathogenic fungi or heavy fungal growth were seen, a positive fungal culture was reported. Following the manufacturer’s instructions, the VITEK 2 system (bioMérieux, Marcy-L’Étoile, France) was used to conduct traditional yeast identification and sensitivity tests. The new Clinical and Laboratory Standards Institute (CLSI) recommendations (resistance, sensitivity, and intermediate resistance) were used to interpret antifungal susceptibility.6 Although mold antifungal susceptibility testing was not carried out, molds were identified by macroscopic and microscopic examination using lactophenol cotton blue stain.
Statistical analysis
Microsoft 365 Excel was used to report categorical data frequencies and percentages, whereas mean and mode±standard deviation were used for numerical data. The distribution of fungal isolates among the 3 sample types was compared using the Chi-square test. Multivariate regression was used to examine risk groups and comparative risk variables for candidiasis based on data distributions. Statistical significance was defined as a p-value of less than 0.05. In the data analysis, patients with RFI were counted as one case per year to determine the annual prevalence of fungal infections. Every time a new positive culture was detected, or a treatment was altered, the number of patient episodes was recorded. By dividing the number of patients with RFI by the total number of admissions, the prevalence rate of RFI based on hospital admissions was determined: prevalence rate=(n/total population) × 10n. By dividing the number of RFI episodes each year by the number of episodes in the year before, the change ratio of RFI episodes over time was determined. The number of episodes in 2023 divided by the number of episodes in 2014 yielded the total increase ratio.
Results
Incidence and prevalence of RFI
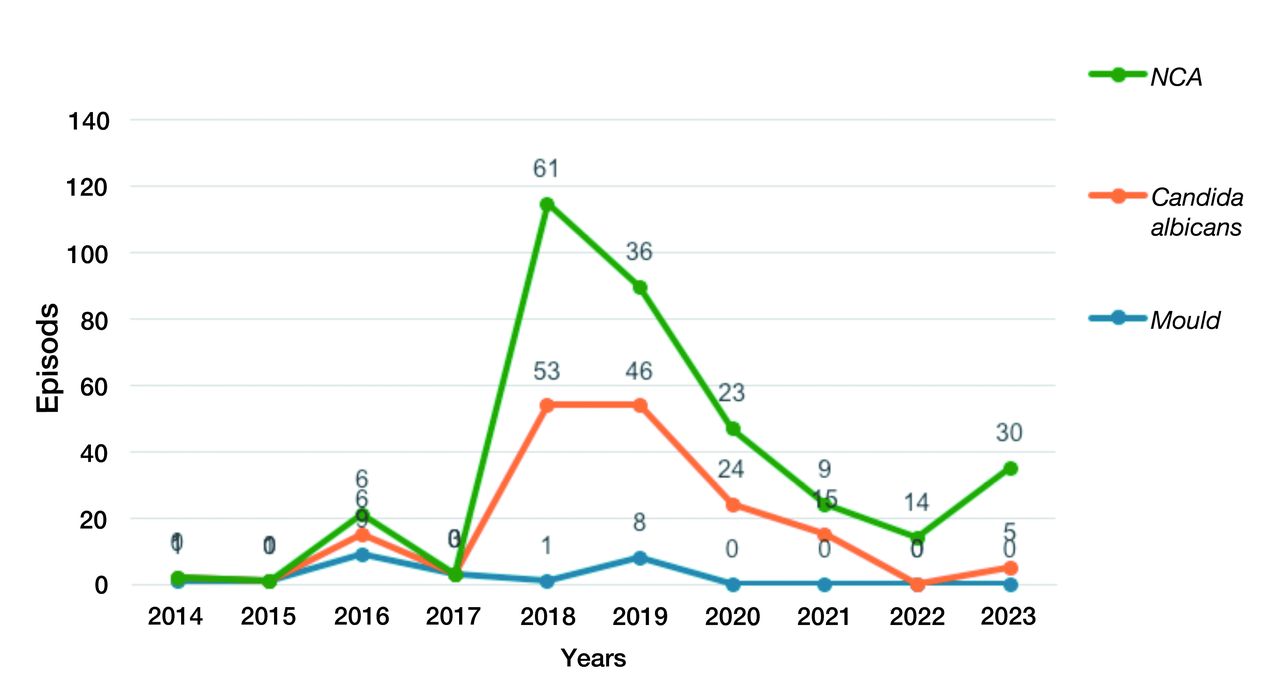
Over the past 10 years, data show a variety of organisms related to respiratory infections, indicated by a significantly high fungal colony count. Among the analyzed population, 22% had RFI with confirmed cultures (n=8508), while the remaining 78% had normal flora or negative cultures (n=38066). The number of all organisms isolated has progressively increased over the study period. No postive fungal results were recorded for RFI in 2013 (n=0). In 2014, there were mold (n=1), C. albicans (n=1), non-Candida albicans (NAC) (n=0) compared with data from 2023 with mold (n=0), C. albicans (n=5), and NAC (n=30) (Figure 2). The incidence peaked in 2018 (mold, n=1; C. albicans, n=53; NAC, n=61) and 2019 (mold, n=8; C. albicans, n=46; NAC, n=36). The total number of fungal isolates was 352, with the highest number being NAC (n=179), followed by C. albicans (n=150), and a few mold isolates (n=23). The incidence of RFI dramatically increased (9.6-fold) from 2013 to 2023, peaking in 2018-2019 (Table 1). The incidence per 10,000 was highest in 2018 (n=3094), 2019 (n=1931), and 2020 (n=862). Accordingly, the prevalence of RFI increased 12-fold, with the highest prevalence in 2018 and 2019 (1.02%, 0.77%). The lowest prevalence of RFI was recorded in 2015 at 0.01%. There was an overall increase in RFI episodes of 17.5-fold over the past 10 years.

- Number of fungal episodes isolated between 2014 and 2023. The year 2013 had no fungal positive cultures that met the study criteria
- Incidence and prevalence of respiratory fungal infections.
Demographic characteristics of patients with RFI and sample type
The distribution of fungal organisms isolated from respiratory samples between 2013 and 2023 was grouped by age: adults (20-60 years old) and seniors (greater than 60 years old). There was a high statistical significance in the predominance of isolates in seniors compared with adults (p-value=4.69×10-23) using multifactor regression analysis (Multiple R 0.87, R Square 0.760) (Table 2). The most common fungal organism isolated was C. albicans, which accounted for 43% of all isolates, with 69% of C. albicans isolates found in patients over 60 years old. The NAC species accounted for 51% of all isolates and were more common in patients over 60 years old (88% of isolates in this age group). Molds were more commonly isolated from patients under 60 years old (59%). A. fumigatus was the most common Aspergillus species isolated, accounting for 3.4% of all isolates, with 33% of Aspergillus isolates in patients under 60 years old. A. flavus was the second most common Aspergillus species, accounting for 1.1% of all isolates, with 50% in patients under 60 years old. Mucor species were the least common fungal organism, accounting for 0.6% of all isolates, with all isolates found in patients under 60 years old. C. tropicalis was the most common fungus in patients under 60 years old (34% of isolates), while C. krusei was the least common in patients over 60 years old (1.4% of isolates). There were slightly more fungal isolations in males (55%, n=194) than in females (45%, n=158). In most organisms, males had more episodes except for NAC, where females had more episodes than males (91; 88). Interestingly, C. krusei and Mucor species were only isolated in females (n=5 and n=2). Using multifactor regression analysis, there were no significant differences in RFI between males and females (Table 2).
- Fungal species distributions among sample type, gender, and age groups.
The analysis showed the number of RFI isolates from different sample types. A total of 352 fungal isolates were identified from 242 sputum samples, 52 BAL samples, and 58 biopsy samples. The most common fungal isolates were C. albicans (150 isolates), followed by NAC species (179 isolates), A. fumigatus (12 isolates), and A. flavus (8 isolates). C. albicans was the most common isolate in sputum (n=114), BAL (n=19), and biopsy (n=17). NAC species were the second most common in sputum (n=113), biopsy (n=41), and BAL (n=25). A. fumigatus was the most common mold isolate in BAL (n=8) and sputum (n=4), with none isolated from biopsy samples. Other Aspergillus species were isolated only from sputum samples, including A. niger (n=5), A. flavus (n=4), and Mucor species (n=2). There was a statistically significant difference in the distribution of fungal isolates between the 3 sample types (p<0.001). The chi-square statistic was 22.43, with 4 degrees of freedom (df), indicating a significant difference in the distribution of fungal isolates between the sample types. C. albicans and NAC species were more likely to be isolated from sputum samples, while A. fumigatus was least likely to be cultured from biopsy samples.
A total of 352 fungal species were tested for resistance to azoles, caspofungin, micafungin, 5-fluorocytosine, and amphotericin B. Of these, 296 (84.1%) were sensitive, and 10 (2.8%) were resistant. Two isolates of C. albicans were resistant, one to fluconazole and the other to micafungin. Among NAC species, there were 8 resistant isolates (4.7%). The most common resistant species were C. krusei (2; 3, 67%) to caspofungin and 5-fluorocytosine, C. parapsilosis (2; 16, 12.5%) to amphotericin B and micafungin, C. glabrata (2; 22, 9%) to fluconazole and voriconazole, and C. tropicalis (2; 117, 1.7%) to 5-fluorocytosine. There were no resistant isolates in C. dubliniensis, and none of the 23 mold isolates were tested for anti-fungal susceptibility. These results suggest that azole resistance is a significant problem in candidiasis, indicating the need for new antifungal agents to treat these infections. The most common resistance was to 5-fluorocytosine.
Comorbidity analysis of the treatment and antifungal resistance in patients with RFI
Respiratory conditions were the most prevalent comorbidity throughout the analyzed period, peaking in 2018 (36 cases) and 2019 (39 cases), with a significant decline in 2021 and 2022. Gastrointestinal (GIT) issues followed a similar pattern, peaking in 2018 (18 cases), dipping in 2019, and rising again in 2023 (11 cases). Lower limb injuries and diabetes exhibited a concerning upward trajectory, peaking in 2023 (10 cases). Few episodes were identified in patients with coma, fever, and hypokalemia (n=6, 1.7% each), with amoebic infections detected in 4 cases in 2021. The GIT issues (22%) and respiratory problems (19%) were notable, while oncology (9%) and kidney disease (4%) also played a role (Table 3). Multifactor regression analysis showed significant associations with respiratory, oncology, coma, fever, GIT, cardiovascular disease (CVD), and accidents. This suggests both opportunistic and potentially causative links between C. albicans and various underlying conditions. NAC infections showed a strong link with respiratory comorbidities (38%), followed by lower limb complications (24%) and CVD (12%). There was a significant association seen in respiratory, hypokalemia, CVD, and sepsis. Table 3,4 shows a gradual increase in the percentage of NAC infections compared with C. albicans over the years. Mold infections, though less frequent, were predominantly associated with respiratory issues (38%) and lower limb injuries with diabetes (42%). There was a significant link between respiratory, GIT, CVD, and sepsis but not significant for lower limb injuries with diabetes (Table 3,4).
- Number of comorbidities over the study period and occurrence in different fungal species.
- Regression analysis of respiratory fungal infections with several comorbidities highlight significant p-value in bold.
The most used antifungal was anidulafungin (13 patients, 26.5%), followed by caspofungin (11 patients, 22%), fluconazole (7 patients, 14%), voriconazole (6 patients, 12%), amphotericin B (5 patients, 10%), and itraconazole (2 patients, 4%). Combination treatment was administered to 5 patients: fluconazole/anidulafungin (3 patients, 6%), and anidulafungin/amphotericin and voriconazole/caspofungin combinations were used to treat one patient each (2%). Only one patient with combination treatment survived (fluconazole/anidulafungin), who had a fluconazole-resistant C. glabrata. Among the 82 treated patients, 18 (21%) survived, whereas 31 (37%) died. Antifungal sensitivity was tested for all isolates in treated patients. Out of 82 patients, 49 (59%) treated with antifungal medication. There were only 2 resistant isolates of C. glabrata, both from one patient diagnosed with malignant neoplasm of the ovary in 2018. The sputum sample from the 59-year-old female patient was positive for fluconazole-resistant C. glabrata. The second episode showed voriconazole resistance.
Discussion
This study provides valuable insights into the trend of rising RFIs. The observed 12-fold increase in prevalence over 1- years, reaching 0.24 per 1000 patients, is concerning. The shift in fungal pathogen distribution was dominated by C. albicans (43%), aligning with previous findings.7-9 However, the emergence of NAC species, such as C. tropicalis (34%), C. glabrata (7%), C. parapsilosis (5%), C. dubliniensis (3%), and C. krusei (1%), was notable. Since Candida is a common oral flora and typically considered a colonization, we cannot claim that every isolate of Candida from lung samples was infectious.10 Although all reported episodes were heavy growth, from a clinical perspective, it is not significant to treat patients for isolated Candida from respiratory samples, except in cases where patients had lung disease or severely immunocompromised. Thus, it is crucial to differentiate between fungal colonization and infection.11 The overall isolation of molds (7%) was dominated by A. fumigatus suggests an increasing presence of molds, demanding vigilance for invasive aspergillosis in high-risk individuals. The dominance of A. fumigatus also aligns with RFI reported by other studies.7,12,13 This study showed antifungal treatment was administered to a substantial proportion (59%) of the patient cohort, with anidulafungin being the most frequently utilized agent. Notably, the mortality rate within the treated group was 16% higher than the overall survival rate. This outcome raises questions about the efficacy and potential adverse effects of antifungal therapy, possibly due to delayed treatment or antifungal resistance.
The RFI was more common in seniors than in adults in yeast infections, while molds were more commonly found in adults than in seniors. This analysis found men were more likely to have RFI, particularly with C. albicans and mold species, while women were more likely to be infected with NAC species. The reasons for these differences are not fully understood but may be due to differences in hormone levels, immune function, or behavior. Limitations of this retrospective study prevent definitive conclusions about gender differences in fungal infection risk.
The study highlights the importance of BAL in confirming mold etiology, especially in A. fumigatus isolation, when non-specific respiratory symptoms persist, particularly in immunocompromised patients. It also suggests that A. fumigatus may be more likely to colonize the lower respiratory tract, while Candida species may cause infections in both the upper and lower respiratory tracts. Several factors might contribute to these trends, such as an increase in dust storms, construction activities, and changing agricultural practices, which could be increasing exposure to fungal spores in the environment. Other host factors, such as an aging population and the rising prevalence of comorbidities like diabetes, which weaken immune defenses, could be creating a more susceptible population. The type of sample collected can significantly impact the types of fungi isolated. Although our data show lower fungal detection in BAL samples, this might be due to decreased requests for BAL samples. Previous studies have shown that for suspected fungal infection of the lower respiratory tract, a BAL sample is more likely to yield a positive culture than a sputum sample. Conversely, for suspected fungal infection of the upper respiratory tract, a sputum sample may be more likely to yield a positive culture than a BAL sample.14-16 Candid albicans and NAC species were more likely to be isolated from sputum samples, while A. fumigatus was more likely to be isolated from BAL samples. A. flavus, A. niger, and Mucor spp. were only isolated from sputum samples. Although only one case of fluconazole- and voriconazole-resistant C. glabrata was identified in sputum samples, it is concerning, but insufficient data are available to draw broader conclusions about antifungal resistance.
The dominance of respiratory conditions as the most prevalent comorbidity was expected. Living in the Saudi climate, individuals are always exposed to air conditioning due to the hot weather or desert storms, and fluctuations in air quality with airborne spores impact susceptibility. In our previous work investigating environmental screening for fungal distribution in the Medina region, we reported an abundance of Candida (34%) and Aspergillus species (15%).4 The decline in respiratory cases during 2021-2022 (during COVID-19) suggests possible factors such as targeted public health interventions promoting respiratory hygiene and early management of respiratory infections, as well as the increased use of air filtration systems reducing exposure to respiratory pathogens. Other comorbidities included GIT issues, which could be due to potential underlying causes such as specific dietary factors, medications, or prevalent gut microbiome imbalances contributing to the rise in GIT issues and their association with RFI. Diabetic patients with lower limb injuries are at increased risk for fungal infections and potentially severe complications. It is also possible that lower limb injuries create an entry point for fungal pathogens, allowing access to other organs. While progress in managing coma, fever, and hypokalemia is evident, the rise in lower limb injuries and emerging threats like amoebic infections demand focused attention on diabetes care and prevention.
In conclusion, the RFI in Saudi Arabia are increasing, becoming more diverse, resistant to treatment, and affecting both upper and lower respiratory tracts. This evolving threat requires improved diagnostics, optimized treatments, and preventive measures to be addressed effectively through collaboration between healthcare providers, researchers, and policymakers.
Acknowledgment
We are grateful to Mr. Sameer Elhendawi and King Fahad Hospital for data extraction. We acknowledge ContentConcepts (www.contentconcepts.com) for the English Language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received October 8, 2024.
- Accepted January 24, 2025.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.