


Abstract
Objectives: To determine specific positive immunoglobulin E (IgE) antibodies to various inhaled allergens in residents of Ajman and the northern region of the United Arab Emirates (UAE) using an automated evaluation of a membrane-based test.
Methods: A total of 104 patients’ blood samples were received from various hospitals and clinics in Ajman and other northern Emirates regions at Thumbay Laboratory, Thumbay University Hospital, Ajman, UAE, to carry out inhalation allergy tests during the study period of 12 months (February 2023 until January 2024). Using the EUROLINE immunoblotting method, 20 different inhalation allergens-impregnated latex strips were used to carry out the allergy test on the patients’ serum samples.
Results: In total, 67 (64.4%) patients tested positive for various inhaled allergens. Approximately 59.7% (n=40) of the positive patients were commonly sensitized to the house dust mites Dermatophagoides farinae and Dermatophagoides pteronyssinus, cockroach, and Candida albicans. High to very high IgE antibody titers (17.5≤sIgE<50.0 and 50.0≤sIgE<100.0 kU/l) to the dust mites were detected in the patients’ age groups 1-15 and 31-45 years, and 31.25% of them from the same age groups were polysensitized to ≥3 different allergens.
Conclusion: The prevalence of positive IgE to various allergens among men was higher than women. These findings highlight the prevalence of IgE sensitization to various inhaled allergens to emphasize more public awareness and implement preventive measures necessary for controlling inhalation allergy-related diseases.
Allergies are a common ailment, affecting over 20% of the population in both developed and developing countries.1 Major allergic diseases, such as allergic rhinitis, asthma, atopic dermatitis, and urticaria, are chronic conditions that cause significant disability and impose substantial costs on individuals and society.2,3 Allergic diseases affect millions of people worldwide and pose a huge global health and socioeconomic burden.4 Globally, 400 million people have allergic rhinitis and 339 million have allergic asthma.5 Numerous studies have demonstrated a strong association between immunoglobulin E (IgE) sensitization to inhaled allergens and the development of allergic rhinitis, asthma, and atopic dermatitis, collectively classified as type 1 allergies.6
Aeroallergens are classified as outdoor, including pollen, fern spores, and soy dust, or indoor, such as mites and animal dander. However, molds are present in both categories. Pollen, one of the most significant components of inhalant allergens, affects approximately 40% of individuals with atopic conditions.7 Environmental changes, climate shifts, and global warming are expected to worsen respiratory allergies by increasing air pollution and plant allergen levels.8 Moreover, factors such as genetics, age, gender, race, and exposure to microbial infections affect susceptibility to allergies.9,10 Although aeroallergens often trigger IgE-mediated inflammation, the symptoms are frequently overlooked. Many individuals do not report their symptoms or seek treatment.11
A recent study carried out in Japan indicated that 78% of individuals tested positive for IgE to inhaled allergens.6 In the United Arab Emirates (UAE), where approximately 1.3 million residents live, the dusty, arid, and sandstorm-prone environment exacerbates allergic conditions.12 Common allergens contributing to allergic rhinitis and asthma in the region include perennial indoor allergens, seasonal pollens, molds, and even traditional Arab incense (bokhor).13,14 A study carried out in the UAE also found that adolescents exposed to tobacco smoke at home were more likely to experience asthma, wheezing, and dry cough.15
The international study of asthma and allergies in childhood (ISAAC) demonstrated that the prevalence of asthma and allergies in some developing countries was comparable to, or even higher than, that in developed nations, with significant regional variability.16 In the UAE, the prevalence of allergic asthma is slightly higher (7.4%) than that in other Gulf Cooperation Council countries, such as Kuwait (6.4%), Oman (4.8%), and Saudi Arabia (3.6%).9,15,17 A recent study reported that 8.1% of children aged 6-9 years in the UAE had allergic rhinitis, with similar prevalence rates observed among children aged 6-7 and 13-14 years in other Middle Eastern countries participating in ISAAC.14,18
However, a limited number of studies have been carried out on the prevalence of respiratory allergies caused by inhaled allergens among the general population of the UAE.14,15 None of the studies have focused on determining individual inhaled allergens that induce specific IgE antibodies among the UAE residents. Therefore, the current study aims to address this gap by examining the prevalence of positive allergen-specific IgE antibodies in blood samples from allergic patients at various hospitals and clinics in northern UAE. Measuring allergen-specific IgE antibodies in response to indoor and outdoor allergens is crucial for diagnosing and assessing the risk of allergic diseases such as allergic rhinitis and asthma.
Methods
A retrospective case series study was carried out on blood samples collected from various hospitals and clinics across the northern Emirates of the UAE. These samples were received by the Department of Microbiology and Immunology at Thumbay Laboratory, Thumbay University Hospital (TUH), Ajman, UAE.
In accordance with the institutional review board approval, the study data were retrieved from the laboratory records of Thumbay Laboratory, TUH, for the period from February 2023 until January 2024.
Patients who visited the internal medicine, pediatrics and otolaryngology departments of TUH, Ajman, and other health centers across the northern region of UAE for allergy screening test. The inclusion criteria included: all the blood samples received for the purpose of carrying out allergy screening tests were included during the study period. Blood samples specifically designated for non-allergy-related purposes, such as genetic or biochemical tests not involving IgE sensitization, were excluded.
This study was approved by the institutional review board of Gulf Medical University, Ajman, UAE, with an approval letter dated January 31, 2023, and reference number IRB/COHS/STD/06/JAN-2023. The study design, data collection, study population, and protocol adhered to the World Medical Association Declaration of Helsinki (DoH-Oct2013) and to the 2021 Good Clinical Practice guidelines established by the National Drug Abuse Treatment Clinical Trials Network as well. In addition, the provisions of the ethics statement in the Helsinki study and the principles of patient information confidentiality were observed during all stages of this study. Related research data for the current study were obtained from PubMed, Scopus, references from relevant articles and other databases.
A total of 5 milliliters (mL) of whole blood were collected from patients by qualified phlebotomists at Thumbay Laboratory, TUH, for allergy screening tests. Additionally, 5 ml blood samples were received from various health centers across the northern region of the UAE for allergy screening at Thumbay Laboratory. The collected blood samples were sent to the Department of Microbiology and Immunology at Thumbay Laboratory, TUH, for automated evaluation using a membrane-based immunoblot test. This test employed blotting strips impregnated with 20 different inhaled indoor and outdoor allergens to detect the presence of specific IgE antibodies to the different inhaled antigens and their ranges from low to very high concentration.
The EUROLINE Inhalation Gulf (IgE) test kit (EUROIMMUN Medizinische Labordiagnostika AG, Lübeck, Germany) is designed for the semiquantitative in vitro determination of allergen-specific IgE (sIgE) in serum or plasma, aiding in allergy diagnosis.19 This immunoblot test is a multiparameter assay, with the membrane strip embedded with 20 allergens (timothy grass, cultivated rye, alder, birch, oak, olive, common ragweed, mugwort, Dermatophagoides pteronyssinus [D. pteronyssinus], Dermatophagoides farinae [D. farinae], cockroach [German], cat dander, dog dander, horse dander, camel dander, Penicillium notatum, Cladosporium herbarium, Aspergillus fumigatus, Candida albicans [C. albicans], Alternaria alternata) and one cross-reactive carbohydrate determinant marker, allowing the simultaneous analysis of sIgE against multiple allergens. According to the kit protocol, the test strips are first moistened with 1.0 mL of phosphate-buffered saline (PBS) for 5 minutes (min), followed by incubation with 400 µL of undiluted patient serum for 60 min at room temperature (18-25°C) on a rocking shaker. After the serum is aspirated, the strip is washed 3 times with 1.0 mL of PBS for 5 min. If specific IgE antibodies are present in the sample, they bind to allergens on the strip. Detection of bound antibodies requires a second incubation for 60 min with 1.0 mL of enzyme-labeled anti-human IgE (enzyme conjugate). After the removal of excess conjugate, the strip is washed 3 times with 1.0 mL of PBS for 5 min. A substrate solution (1.0 mL) is then added and incubated for 10 min on a rocking shaker to catalyze a color reaction. The strip is subsequently placed onto the adhesive foil of the work protocol sheet, airdried in a dark environment, and scanned using the EuroBlotScanner (EUROIMMUN Medizinische Labordiagnostika AG, Lübeck, Germany).20 The intensity of the reaction bands is measured and assigned to enzyme-allergo-sorbent test classes, ranging from 0-6, reflecting concentration grades consistent with the radio-allergo-sorbent test system used in the allergy diagnostics (EUROIMMUN Medizinische Labordiagnostika AG, Lübeck, Germany).20
Statistical analysis
Data were analyzed using the Statistical Package for the Social Sciences, version 28.0 for Windows (IBM Corp., Armonk, NY, USA). Descriptive statistical tests were carried out, the categorical data are presented with frequency and percentage. The inferential statistical analysis was carried out by using bivariate analysis (Chi-square test) and results are presented with odds ratio (OR), with the significant level at a p-value of 0.05.
Results
A total of 104 blood samples were collected and processed for routine inhalation allergy testing during the study period. Of these, 61 samples were from male patients and 43 from female patients, further categorized by ethnicity into Arab and non-Arab groups and distributed across 5 age groups. Immunoblotting tests indicated that 67 (64.4%) samples were positive for single or multiple inhalation allergens, whereas 37 (35.6%) samples were negative. Details of the study population, including age groups, ethnicity, and IgE status, are provided in Table 1. No statistically significant difference in overall allergy test was observed between gender or ethnicities. In this study the Chi-square test was carried out, and the association was presented by p-values. No confidential intervals were used. In all inferential statistics, only bivariate analysis was carried out and no multivariate analysis.
- Immunoglobulin E status in the demographic subgroups of the study population (N=104).
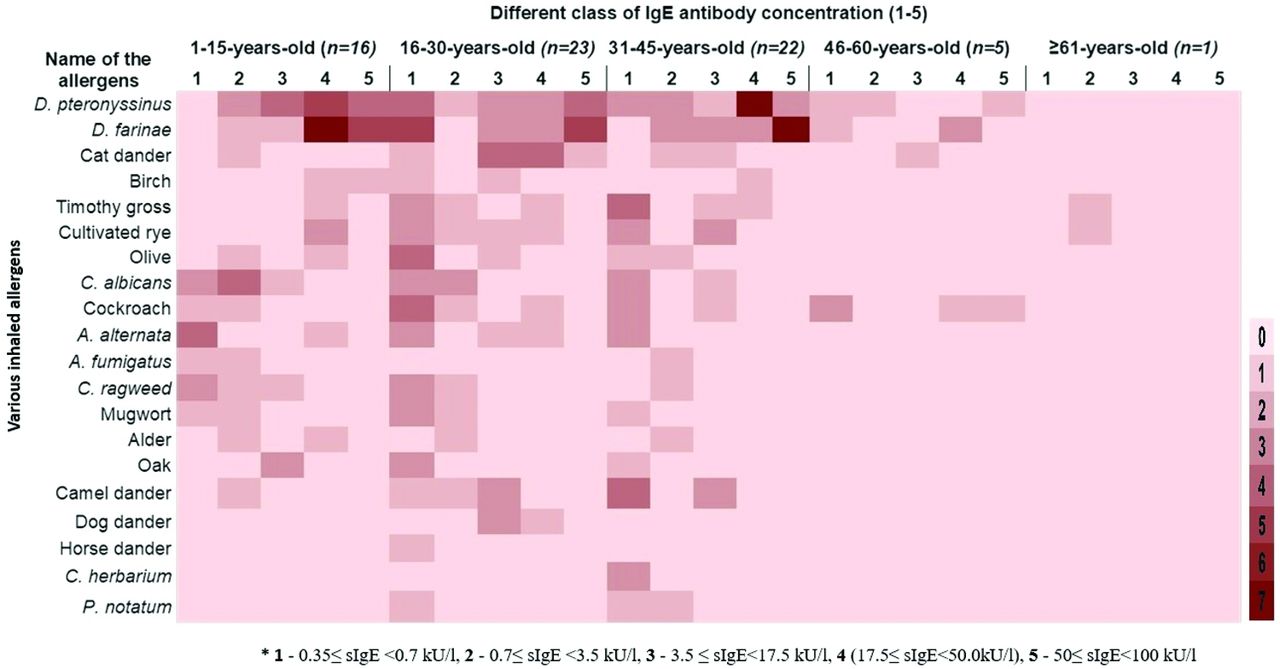
Details of the 20 inhaled allergens tested, along with the ranges of specific positive IgE antibodies categorized into 6 classes, are mapped to each patient’s age group, gender, and ethnicity are shown in Tables 2 & 3, and Figure 1. In all the tables only bivariant analysis was carried out and no multivariant analysis carried out.
- Frequency of single and multiple inhaled allergens in male and female patients of different age groups in both Arab and non-Arab study populations with varying classes of immunoglobulin E concentration.

- Frequency of patients sensitized to various inhaled allergens across different age groups of the study population based on immunoglobulin E antibody titer classes (1-5).
- Allergen-specific sensitization according to gender, ethnicity, and age group.
In 1-15 years old age group, 66.7% of patients tested positive for one or more inhaled allergens, with IgE concentrations ranging from 0.35 to <100 kU/l. Among the positive samples, one patient exhibited sensitization to 10 allergens, and 75% had antibodies against D. pteronyssinus and D. farinae. Furthermore, 69% of patients showed high IgE levels (17.5 to <100 kU/L). Additionally, 37.5% were sensitized to C. albicans and 25% to common ragweed, with antibody concentrations ranging from 0.35 to <17.5 kU/l.
In the 16-30 years old group, 71.9% of patients tested positive for at least one allergen. Of these, 43.5% were sensitized to D. pteronyssinus and D. farinae, with IgE ranging 0.35 to <100 kU/l. Among the positive cases, 17.4% had very high titers of IgE (50 to <100.0 kU/l). Two samples showed sensitization to 11-13 different allergens, with antibody ranging from 0.35 to <50 kU/l.
In the 31-45 years old age group, 64.7% of samples were sensitized to various inhaled allergens. Among these, 36.4% (n=8) exhibited very high antibody titers to D. pteronyssinus and D. farinae, whereas 18.2% (n=4) showed positive reactions to 6-9 different allergens, with IgE titers ranging from 0.35 to <100 kU/l.
In the 45-60 years old group, 80% (n=4) were positive for cockroach allergen and 60% (n=3) of the samples were also sensitized to D. pteronyssinus and D. farinae, with varying IgE titers. In the age group ≥61 years old, 25% of samples showed positive sensitization to timothy grass and cultivated rye, with low antibody titers (0.7 to <3.5 kU/l).
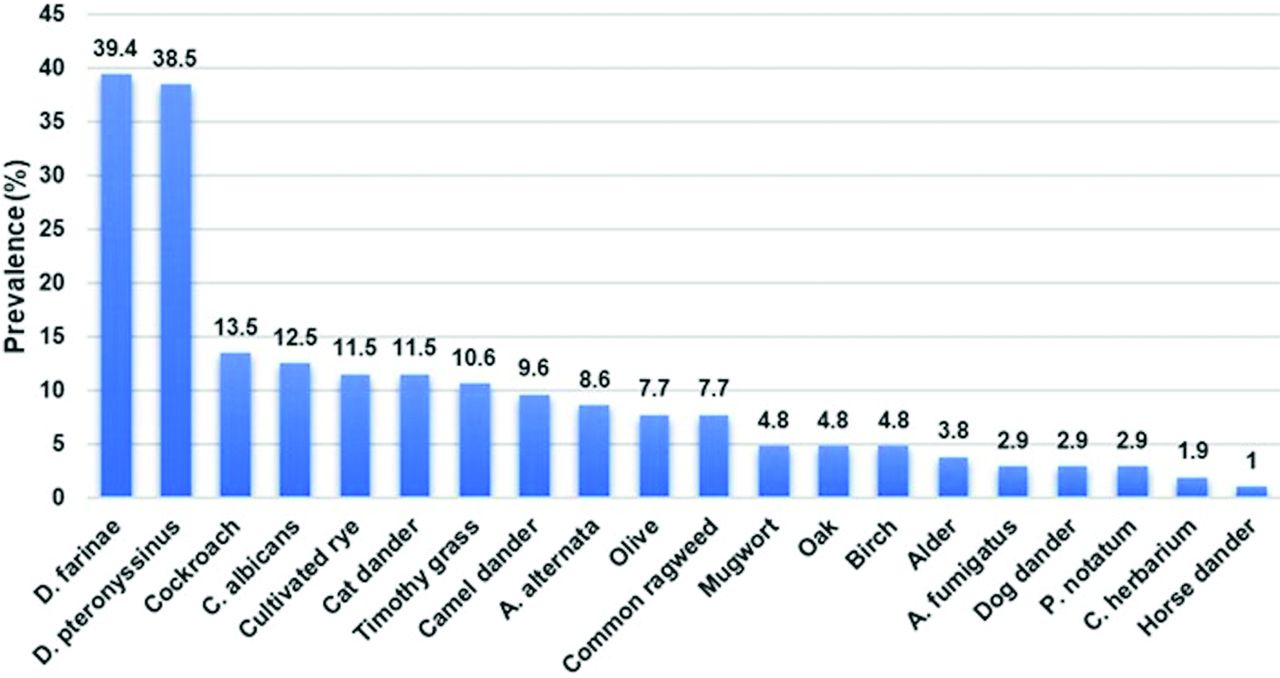
The overall prevalence of sensitized IgE antibodies to various inhaled allergens is summarized in Table 4 and Figure 2. The Chi-square statistical analysis was carried out in Table 4 between male and female showing some significance differences for the following allergens: D. pteronyssinus (p=0.007), D. farinae (p=0.005), cockroach (p=0.027), and C. albicans (p=0.042). No significant differences were identified for other allergens in relation to the male and female study population.
- Prevalence of immunoglobulin E sensitization to various inhaled indoor and outdoor allergens according to the gender and ethnicity.

- Prevalence of immunoglobulin E sensitization to 20 inhaled indoor and outdoor allergens represented in a descending manner.
Discussion
Respiratory allergies affect a significant portion of the global population and adversely affect quality of life, highlighting the need to understand potential causes for effective prevention.21 Atopic reactions to respiratory allergens commonly involve the upper and lower airways, eyes, and skin, and can occasionally lead to systemic effects.22,23 Prolonged exposure to allergens, even at low levels, can worsen symptoms and trigger bronchial hyperresponsiveness. Indoor dust mites are the leading cause of allergenicity worldwide, making the home a critical microenvironment for indoor allergens. Even minimal allergen exposure can induce hyperresponsiveness in individuals already sensitized to specific allergens.24 Assessing the prevalence of respiratory allergens in both indoor and outdoor environments is essential for implementing effective preventive measures. The present study investigated the prevalence of serum-specific IgE antibodies to various inhaled allergens in blood samples collected from sensitized individuals in the northern region of the UAE.
In the present study, 64.4% of patients exhibited varying concentrations of IgE antibody titers to a range of indoor and outdoor allergens. In the 1-15 year age group, 24% of samples showed sensitization to different antigens, with 75% testing positive for house dust mites (D. pteronyssinus and D. farinae), displaying antibody titers ranging from 3.5 to 100 kU/L. Nearly 44% of these patients were sensitized to more than 3 allergens, primarily A. alternata, A. fumigatus, and C. albicans, whereas 12.5% of samples were poly-sensitized to 10 or 11 allergens. Regional variations in inhaled allergen sensitization have also been reported. Moradi et al25 found that 20-23% of children under 6 years were sensitized to D. farinae, A. fumigatus, and A. alternata. Similarly, in Brazil, 12.3% of children under pediatric age group and 2.5% of adults were tested positive to allergic bronchopulmonary aspergillosis and also so high IgE antibody titer.27 In comparison, 44% of patients in the UAE were sensitized to multiple inhaled allergens.
In this study, 52.2% of patients aged 16-30 years were sensitized to D. pteronyssinus and D. farinae, 34.1% to cat dander, and 13.7% to cultivated rye and cockroach allergens. These results are nearly double of those reported by Xue et al,28 who found that 20% of individuals in the same age group in China were sensitized to D. dust mites. Similarly, a study from Iran reported that 21.1% of patients were sensitized to D. farinae and 20.6% to cockroach allergens, consistent with the findings of our study.25 In India, 23.4% of participants were sensitized to indoor dust mites.28 In our study, 39% of participants were poly-sensitized to 3 or more allergens, with 2 individuals sensitized to 11-14 allergens at varying IgE concentrations. In addition, 9.2% of positive samples showed sensitization to the fungal pathogens C. albicans and A. alternata. Similarly, 9% of serum samples from a healthy Japanese population were sensitized to A. alternata and Aspergillus species.6
In the current study, 59% of patients aged 31-45 years were sensitized to D. pteronyssinus and D. farinae, 22.7% to timothy grass, and 18.2% to camel dander and cultivated rye. Similarly, 50.5% of healthy individuals in the same age group in Japan were sensitized to D. pteronyssinus, whereas 41.3% of pregnant women in Taipei, Taiwan, were sensitized to D. farinae and D. pteronyssinus.6,29 In this age group, 4 samples showed polysensitization to 6-9 allergens, with antibody titers ranging from low to high concentrations. Among patients aged 46-60 years, 7.5% of positive cases were identified. Of these, 4 (80%) samples were sensitized to cockroach allergens, followed by 60% sensitization to D. pteronyssinus and D. farinae. Only one positive sample was recorded in the ≥61-year age group, showing sensitization to timothy grass and cultivated rye allergens.
In the present study, 25.4% of serum samples exhibited monosensitization, whereas 74.6% demonstrated polysensitization to inhaled allergens. Overall, 39.4% of the samples were sensitized to the indoor allergen D. farinae and 38.5% to the indoor allergen D. pteronyssinus, followed by cockroach (13.5%), C. albicans (12.5%), cultivated rye (11.5%), cat dander (11.5%), timothy grass (10.6%), camel dander (9.6%), and other indoor and outdoor allergens (≤9.6%). Men (70.15%) were predominantly sensitized to inhaled allergens compared with women, with non-Arab men (50.74%) showing higher sensitization than Arab men (19.4%). Similar trends have been reported in previous studies from Iran, Japan, and Saudi Arabia, where the prevalence of positive IgE to various inhaled allergens was higher in men than in women.6,7,18 However, contrasting findings were observed in studies by Al-Tamemi et al30 and Heck et al,31 where women were more frequently sensitized to indoor and outdoor allergens than men. Al-Tamemi et al30 also reported a higher prevalence of IgE to inhaled allergens among Arabs compared with non-Arabs. Additionally, a slightly higher rate of polysensitization to 3 or more allergens was observed in the non-Arab population (6.34%) across all 5 age groups compared with 2.61% in the Arab population. Notably, the highest rate of polysensitization (8.95%) was found in the 16-30 and 31-45 years age groups within the non-Arab population.
Study limitations
The study samples were received from various hospitals, clinics, and Thumbay hospitals located in and around the northern emirates of the UAE (Sharjah, Ajman, Umm-Al-Quwain, and Fujairah) and did not receive samples from other Emirates (Dubai, Abu Dhabi, and Ras-Al-Khaimah). Additionally, the study did not include the allergic symptoms of the patients, physician documentation, and the patients’ response to treatment. This important limitation should be addressed in future studies.
In conclusion, this study highlights a slightly higher prevalence of inhalation allergen-specific IgE antibodies in the northern region of the UAE, potentially linked to unique environmental and lifestyle factors characteristic of the area. The dominance of D. farinae and D. pteronyssinus as primary allergens underscores the significant role of indoor environmental conditions, such as dust accumulation and humidity, in sensitization.
The prevalence of positive IgE to various allergens was higher in men compared to women. Notably, higher sensitization rates in male patients suggest possible differences in allergen exposure and immune response between genders. Additionally, children aged 1-15 years demonstrated elevated IgE titers and a higher likelihood of polysensitization to more than 4 allergens. These findings emphasize the critical need for early intervention and prevention strategies in pediatric populations to mitigate the risk of severe allergic reactions and associated comorbidities.
The study also stresses the importance of targeted awareness campaigns and preventive measures, particularly focusing on indoor allergen management in high-risk regions and populations. The results offer valuable insights for the development of region-specific diagnostic tools and treatment strategies to improve patient outcomes. To build on these findings, further large-scale, population-based studies are recommended to better understand allergen sensitization patterns across the UAE and refine public health initiatives. These findings intensify the significant prevalence of IgE sensitization to inhaled allergens, highlighting the need for increased public awareness and the implementation of preventive measures to manage inhalation allergy-related diseases.
Acknowledgment
The authors gratefully acknowledge the efforts of the physicians, microbiologists, and other staff of Thumbay Laboratory and Hospitals, Ajman, United Arab Emirates, for their contributions to data collection and for carrying out this study. We also wish to express our gratitude to the College of Health Sciences and the College of Medicine at Gulf Medical University for their unwavering support throughout the research process. Additionally, the authors would like to thank ContentConcepts Native English Editing Service Company (www.contentconcepts.com) for their English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received October 26, 2024.
- Accepted February 6, 2025.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.