


Abstract
Adult onset Still’s disease (AOSD) is a chronic inflammatory disorder involving multiple systems. The symptoms mimic those of lymphomas, therefore, the diagnosis of lymphoma needs to be excluded prior to establishing the diagnosis of AOSD. Another similar condition is dermatopathic lymphadenopathy (DL). In DL, the histopathological appearance of lymph node biopsy may also mimic AOSD. The DL is associated with several systemic pathologies, such as malignant lymphomas, and rarely AOSD. We present a case of a 43-year-old male presented with 3 months history of fatigue, fever, and lymphadenopathy. Initial work-up satisfactorily met the criteria for diagnosis of AOSD. But considering the well-known association of DL with hematological malignancies, detailed pathological studies were considered, including tumor markers to rule out the possibility of malignancy. The patient was started on steroids and showed remarkable recovery within 2 weeks. Evaluation of malignant lymphomas in a patient with DL is important, in order to diagnose AOSD and rule out hematological malignancy.
First described by Sir George Frederick Still in 1897 in 22 children with juvenile idiopathic arthritis, Still’s disease was mainly considered a disease of children.1 1971, Bywaters2 described the first series of 14 adults with a rare multisystemic anti-inflammatory disorder with high spiking fever, polyarthralgia, a salmon pink rash, and hepatosplenomegaly.2 The median age at diagnosis is 36 years, but may occur as late as 83 years. Prevalence is more in women as compared as with men.3 Although some studies have identified HLA susceptibility antigens, no familial studies have shown a genetic association. Due to involvement of inflammatory cells, lymphadenopathy is a common feature of this condition. The spectrum of lymphadenopathy in adult onset Still’s disease (AOSD) has been analyzed in various studies, but the association of AOSD with dermatopathic lymphadenopathy (DL) has not been reported in these studies before.4 The DL is a type of lymphadenopathy in which there is a localized paracortical proliferation of histiocytes and melanin is deposited in the lymph nodes.5 It is a reactive hyperplasia of the lymph nodes, which has also been reported to be associated with cutaneous T cell lymphoma (CTCL) and Hodgkin’s lymphoma.4 We describe a 43-year-old male with a differential diagnosis of AOSD and lymphoma. The objective from presenting this particular case it to highlight the rare association of DL with AOSD and to emphasize the importance of ruling out other conditions associated with DL before establishing the diagnosis of AOSD.
Case Report
A 43-year-old male without any past medical history was hospitalized with progressive fatigue over a period of 3 months. It was associated with intermittent high-grade intermittent fevers of 40°C. In addition, he complained of sore throat, anorexia and 15 kilograms unintentional weight loss. He denied history of night sweats, nausea, vomiting, early satiety, abdominal pain, or changes in bowel habits. He never smoked cigarettes or used illicit drugs. Review of history was significant for severe pain, and morning stiffness in multiple joints including both ankle joints, metacarpophalangeal joints and proximal interphalangeal joints of both hands. His joint pain in hands was severely limiting his activities to the limit that he had difficulty in walking due to ankle pain. On presentation, vital signs were within normal limits. There was swelling, tenderness, warmth and decreased range of motion due to pain of small hand joints in symmetric fashion. Skin was free of any rash. Abdominal examination revealed a 16 cm hepatomegaly. There were palpable axillary and inguinal lymph nodes bilaterally. Rest of the systemic examination was unremarkable for any significant findings. The laboratory exam revealed anemia (hemoglobin 9.53 gm/dl), leukocytosis (white blood cells 23,6 X 10.e9/L), thrombocytosis (platelet count 941 X 10.e9/L), deranged liver function tests (aspartate amino transferase 75 U/L, gamma-glutamyl transferase 151 U/L, LDH 343 U/L, alkaline phosphatase 351 U/L), elevated erythrocyte sedimentation rate (67 mm/H), and C-reactive protein concentration (186 mg/L). Thyroid profile and immunoglobulin panel were normal. Antinuclear antibodies and rheumatoid factor were negative, ferritin levels were found to be extremely high (8267 ug/l). The C3 and C4 complement levels were within normal limits. Blood and urine cultures were negative. A computed tomography of the chest, abdomen, and pelvis showed hepatosplenomegaly and enlargement of para-tracheal, axillary, inguinal and iliac lymph nodes. Bone marrow biopsy and fine needle aspiration biopsy of inguinal lymph node showed normal results, so an excision biopsy of axillary lymph node was carried out, which showed DL (Figure 1). The immunohistochemical studies for CD20, CD79A, CD3, CD5, CD10, BCL6 were negative. Initial work-up satisfactorily met the Yamaguchi criteria for the diagnosis of AOSD.6 Considering the well-known association of DL with hematological malignancies, detailed pathological studies were considered including tumor markers. Once the results were negative, a final diagnosis of AOSD was established as a ‘diagnosis of exclusion’. He was started on low dose steroid and showed a remarkable recovery within 2 weeks. His symptoms of arthritis improved within 3 days and he was discharged to follow up in rheumatology clinic.

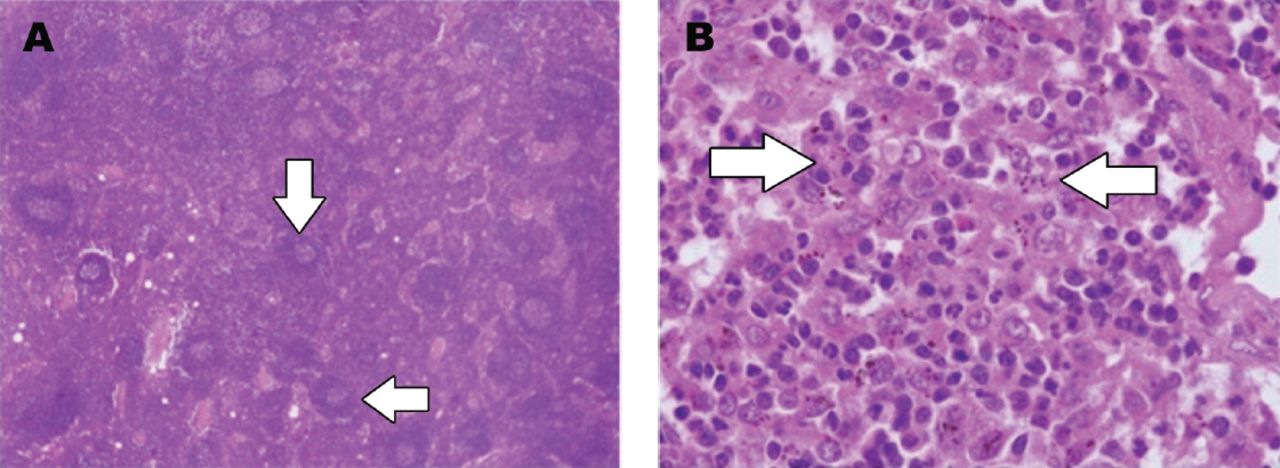
Histopathological examination showing: A) Low power view showing expansion of paracortical areas with preservation of lymphoid follicles. B) High power view showing a mixture of histiocytes, dendritic cells, plasma cells, neutrophils, eosinophils, and lymphocytes. Note the melanin pigment in the histiocytes, which suggests the name ‘dermatopathic’.
Discussion
The diagnosis of AOSD is based upon exclusion since it consists of heterogeneous symptoms and has no definite diagnostic tool. The AOSD is commonly considered as one of the differential diagnosis in fever of unknown origin, especially if associated with multiple organ involvement. Lymphadenopathy commonly occurs in AOSD. Sometimes it may be difficult to differentiate malignant hematologic disorders from AOSD. Not only clinical features are similar, but also, histopathological features of lymph node biopsy may also mimic lymphoma. One such pathology is DL. In DL, there is reactive paracortical hyperplasia of lymph nodes. It is characterized by increased number of Langerhen cells, dendritic cells, and histiocytes with cytoplasmic melanin deposition.5 It is well known to be associated with malignant lymphomas, especially Hodgkin’s lymphoma. Other major associations include Langerhans cell histiocytosis, myeloid sarcoma with monocytic differentiation, and metastatic melanoma.4 There are certain cell markers, which can be used to narrow down the differential diagnosis. In Hodgkin’s lymphoma, the Reedsternberg and Hodgkin cells are positive for CD15 and CD30, and negative for CD45, whereas in Langerhans cell histiocytosis, lymph nodes demonstrate sinusoidal pattern associated with focal necrosis.7 In myeloid sarcoma with monocytic differentiation, the myeloid/monocytic antigens are positive, and the S100 protein is negative as compared with metastatic melanoma, in which the melanoma cells are S100 positive with atypical mitosis.4 Other system conditions like syphilis and HIV are also associated with DL.8,9 Skin conditions associated with DL, include pemphigus vulgaris, psoriasis, eczema, neurodermatitis, toxic shock syndrome and atrophia senilis.4 Three fourth of the patients with sezary syndrome and mycosis fungoides have DL.10 Considering the multiple associations of DL in multiple systemic disorders, definite diagnosis may be challenging to establish. Signs and symptoms of various chronic disorders presenting with lymphadenopathy may be similar to each other; which makes the diagnosis complicated. The association of DL with previously mentioned diseases are well known, however, AOSD is an important differential, which is rarely reported in association with DL.-
In conclusion, AOSD is rarely reported to have DL. Evaluation of malignant lymphomas, especially Hodgkin’s lymphoma, in a patient with DL is crucial in order to exclude hematological malignancy and diagnose AOSD. This is very critical from therapeutic point of view as treatment approaches are entirely different. Further research needs to be carried out to determine the prevalence of DL in AOSD.
Acknowledgment
The authors gratefully acknowledge Dr. Shadi Qasem, MD, Wake Forest Baptist Medical Center, North Carolina, USA for his assistance in preparation of figure legend.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company.
- Received May 15, 2016.
- Accepted August 24, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}