


Abstract
In the differential diagnosis of patients with ulcers on the lips characteristics like the duration of the ulcer, number, size, depth, shape, base, margins, and distribution are considered. Such ulcers arise from many diseases particularly, viral and bacterial infections, malignancies can also be responsible. Classic syphilitic chancres are painless erosions settled on hard papule; these are evident in the genital area in more than 90% of patients. This study describes a case of a 38-year-old female patient presenting with a painful ulcer covering 3 quarters of the upper lip showing settlement on erythematous, edematous, and indurated plaque covered with hemorrhagic crusts. The aim of this study was to consider differences between the classic syphilitic chancre typically found in the genital region from extragenital chancres and to raise awareness of the possibility of primary syphilis when patients present with painful ulcers on the lip.
Syphilis is a chronic infectious disease that is generally transmitted sexually and caused by Treponema pallidum (T. pallidum), which is a spirochete.1 It may affect the organs and the whole system in different sequential clinical stages due to its nature. It is known as the “imitator of a variety of diseases”.2 The chancre seen at the primary stage is classically a painless erosion overlying a firm papule, which emerges in genital areas in more than 90% of the patients.3 However, extragenital chancres may differ from classic ones in terms of localization, amount, size, depth, base, and edges thus, they may cause diagnostic problems.1,4 In this report, the case of a female patient with a painful, erythematous, indurated, ulcerated lesion on the upper lip with an oedematous base and covered with hemorrhagic necrotic crusts is presented. We aim to remind physicians of syphilis-“the great imitator”-in the diagnosis of patients who are admitted due to lip ulcers with lesions and to review the characteristics of extragenital syphilitic chancres.
Case Report
A 38-year-old female patient was admitted to our polyclinic with the complaint of a gradually enlarging painful wound that had appeared on the upper lip approximately 2 months prior. It was noted that the patient had previously consulted her family physician and a dermatologist at another clinic with the same complaint. She had been pre-diagnosed with herpes labialis, and systematic antiviral, and topical antibacterial treatment had been initiated. Then, the patient had consulted the plastic surgery clinic, as there had been no improvement in her complaint. She had been evaluated as having squamous cell carcinoma and excision had been advised. The patient’s medical background and family history were normal. In the dermatological examination, a painful, erythematous, indurated, ulcerated lesion with distinct edges and adherent hemorrhagic necrotic crusts on top, covering the three-fourths of the upper lip and extending towards the lip mucosa, was observed (Figures 1A & 1B). A mobile, painless, nodule complying with lymphadenopathy (LAD) was present on the right submandibular area. An asymptomatic eroded lesion was detected at the proximity of the intergluteal area; this was approximately 1.5 cm in size with livid edges and a bright red ulcer base. Moreover, it had indistinct borders, a polished surface and a firm base on palpation (Figure 2). The routine laboratory tests revealed the following results; total leukocyte count: 6.99 10^3/uL, hemoglobin: 10.4 g/dL, hematokrit: 32.7%, platelet count: 222 10^3/uL, sedimentation rate: 24 mm/hr, and, C-reactive protein (CRP): 8.3 mg/L. The patient’s human immunodeficiency virus (HIV) test was negative and she was immunocompetent. Other routine biochemical investigations were insignificant. Venereal Disease Research Laboratory (VDRL) was reactive at 32 dilutions and T. pallidum hemagglutination test (TPHA) was positive. In the histopathological examination of the punch biopsy obtained from the lip of the patient, an ulcerated area rich in lymphocytes and plasma cells with high inflammation, vascular proliferation and swelling of endothelial cells in vascular structures were detected (Figure 3). Although atypical in clinical presentation, given the histopathological and laboratory findings, the patient was diagnosed with primary syphilis. Since there was no sign of generalized LAD, typical secondary manifestations such as maculopapular eruptions, organ and system involvement we have concluded that the patient presents with primary syphilis with a classic chancre and an atypical extragenital painful chancre. As treatment, the patient was administered benzathine penicillin G in 2.4 million units intramuscularly as a single dose. The VDRL titres of the patient became negative in 4 months. When the patient’s husband was invited to the clinic to be evaluated for syphilis, it was noted that he had lesions in the oral mucosa consistent with mucoid plaques; he had been diagnosed with secondary syphilis, and given benzathine penicillin G in 2.4 million units intramuscularly as a single dose for treatment and had been following up at the infection clinic. He was also immunocompetent (HIV test: Negative). At the third month of the follow-up, it was observed that the patient’s oral ulcer completely regressed, with slight pigmentation remaining (Figure 4). The intergluteal lesion regressed as well.

Extragenital chancre on the upper lip.

Typical extragenital chancre on the intergluteal cleft.

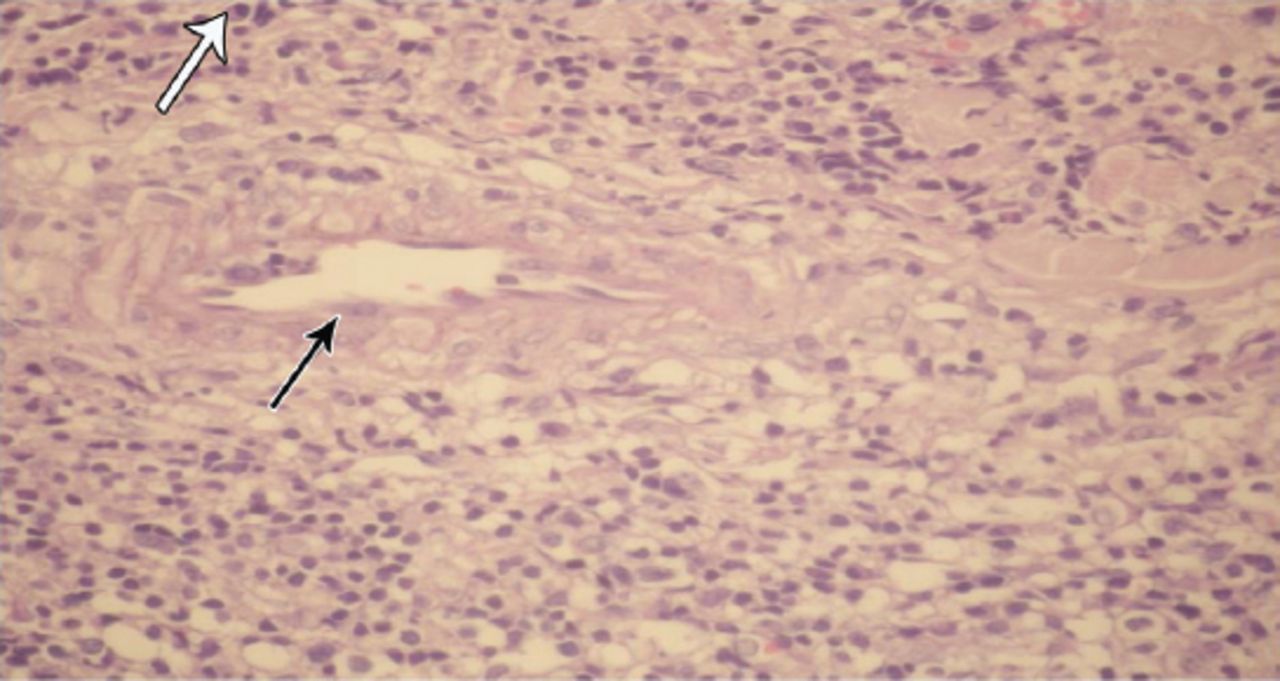
An ulcerated area rich in lymphocytes and plasma cells with inflammation, vascular proliferation and swelling of endothelial cells in vascular structures (hematoxylin-eosin staining; x20 magnification. Plasma cell (white arrow), swelling of endothelial cells in vascular structures (Black arrow).

The patient’s ulcer regressed completely after treatment
Discussion
Primary syphilis is characterized by a syphilitic chancre that appears at the site of contact at 10 to 90 days, approximately 3 weeks after infection with T. pallidum and regional lymphadenopathy that develops a week after the appearance of the chancre.5 The syphilitic chancre is generally singular.1 The erosion is indistinct at the edges, and the tissue in the middle is bright red in colour, with a film layer that looks like polish on which the serosity develops, and a base that feels firm on palpation (Table 1).2,6 There were no other complaints.3 The syphilitic chancre appears in the genital area in more than 90% of patients.3
Features of typical genital chancre and a typical extragenital chancre.
Extragenital chancres may differ in terms of localization, number, size, shape, ulcer depth, and base and edge characteristics, as well as subjective complaints (Table 1). They can be localized anywhere, including the lip, tongue, palate, face, eyes, neck, truncus, nipples, palmar surface, and fingers.1 However, 40-70% of extragenital chancres are located in the oral area and half of them are localized on the lips.1,6 Anorectal chancres are generally encountered in homosexual males, with a prevalence of 2% of cases.7 Extragenital chancres located on the lips may present atypically, wherein they resemble impetigo, traumatic ulcers, herpes labialis, squamous cell carcinoma, leishmania, cheilitis, lichen planus, drug reactions, Behcet disease, bullous diseases, ulcers due to Epstein Barr virus, and/or Cytomegalovirus or cutaneous tuberculosis.1,8,9
In our case, the extragenital chancre found on the intergluteal area is suggestive of a classic syphilitic chancre. The patient was unaware of this lesion, which was detected during our skin exam. The extragenital chancre, located on the upper lip, had an extraordinary clinical appearance.
In conclusion, extragenital chancres may present in different clinical forms. Syphilis must be considered in the differential diagnosis of ulcerated lesions located on any part of the body, whether painful or painless. In the diagnosis, it is crucial to conduct a full dermatological examination, including all mucosa. When sexually transmitted diseases are considered in differential diagnosis, it may become necessary to question partners and even examine them separately.
Case Reports
Case reports will only be considered for unusual topics that add something new to the literature. All Case Reports should include at least one figure. Written informed consent for publication must accompany any photograph in which the subject can be identified. Figures should be submitted with a 300 dpi resolution when submitting electronically. The abstract should be unstructured, and the introductory section should always include the objective and reason why the author is presenting this particular case. References should be up to date, preferably not exceeding 15.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company.
- Received June 15, 2016.
- Accepted August 17, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.