


Abstract
Objectives: To report and describe the management and response to treatment of patients referred to the osteoporosis clinic after prolonged use of bisphosphonate BPs) (4 years and more) with and without new fracture (any site) or any other new skeletal symptoms.
Methods: This is a single center observational retrospective cohort study conducted from January 2009 to May 2016 in a tertiary center. We describe cause of referral, X-rays findings, management, and response to treatment.
Results: Thirty-four patients, aged 46-89 years, were collected. Reason for referral included review of therapy (11 patients), recent low trauma fracture (21 patients), or chronic severe thigh pain (2 patients) of unknown etiology. All patients with fracture or thigh pain (23/34 patients) were treated with teriparatide 20 mcg daily. Sixteen of them (16/23) completed teriparatide course (18-24 months), 11 patients had complete healing of fracture at the end of the course, and 5 remained with nonunion of fracture, the remaining 5 patients were lost to follow up.
Conclusion: Prolonged use of bisphosphonates can lead to atypical femoral fracture that may involve sites other than femoral shaft or rarely chronic thigh pain without fracture. Teriparatide may facilitates fracture healing and improve thigh pain.
Alendronate (fosamax) and zolendronic acid (ZA) 5mg are nitrogen-containing bisphosphonates that inhibit bone resorption. The food and drug administration (FDA) approved alendronate for fracture prevention in postmenopausal women in 1995.1 The approval for alendronate was based on results of the Fracture Prevention Trial (FIT).2 In 2007 zolendronic acid 5 mg got FDA approval for the same indication3 following the results of the HORIZON trial.4 The benefits of bisphosphonates beyond the recommended duration (5 years for alendronat, 3 years for ZA) remained uncertain. In the FIT long-term extension trial (FLEX) alendronate use was extended in a group of FIT patients up to 10 years.6 The FLEX trial showed that women who discontinued alendronate after 5 years had no higher fracture risk other than for clinical vertebral fractures compared with those who continued alendronate. These results suggested that women at very high risk of clinical vertebral fractures might benefit from continuing alendronate beyond 5 years.
In 2005, Odvina et al7 described 9 patients who suffered spontaneous non-vertebral fractures while on alendronate. These fractures were characterized by delay or absent fracture healing, markedly suppressed bone formation and diminished matrix synthesis. These worrying findings may indicate that long term alendronate therapy induced over-suppression of bone remodelling and subsequent increase in fracture risk. Similar reports followed Odivan. These diaphyseal and subtrochanteric femoral fractures where named “atypical femoral fractures (AFF)”.
In September 2010, after a literature review of 310 cases (all were AFF following prolonged use of alendronate), a task force from the American Society of Bone and Mineral Research (ASBMR) found that 94% of cases used alendronate for more than 5 years.8 The conclusion was that atypical femur fractures could be a result of long-term bisphosphonate use. In October 2010, the FDA issued a warning about this complication. The FDA decided to add a warning about the fractures to the labels of all bisphosphonates.
By May 2011 there have been 56 papers describing a total of 329 similar cases.9 Atypical femoral shaft fractures in postmenopausal osteoporosis following prolonged use of ZA 5 mg are not reported. The aim of this study is to identify the clinical and radiological characteristics of patients with a history of prolonged use of bisphosphonates referred to the osteoporosis clinic in a tertiary hospital.
Methods
This is observational, retrospective, cohort study included the medical files and x-rays of patients referred to the osteoporosis clinic at Prince Sultan Military Medical City (PSMMC), Riyadh, Saudi Arabia from January 2009 to May 2016. Inclusion criteria were patients 45 years or older with osteoporosis (postmenopausal or steroid induced) who used a BP for more than 4 years regardless of fracture history. There were no exclusion criteria. Clinical characteristics including age, history of chronic steroid use, history of proton pump inhibitor (PPI) site, of recent fracture, cause of referral, x-rays of the fractures that occurred following alendronate or ZA use, management, and response to treatment were recorded. Delayed healing is described as absence of radiological signs of healing in the form of persistent radiolucent sign 6 months after the fracture. Institutional Review Board approval was provided by the research committee.
Results
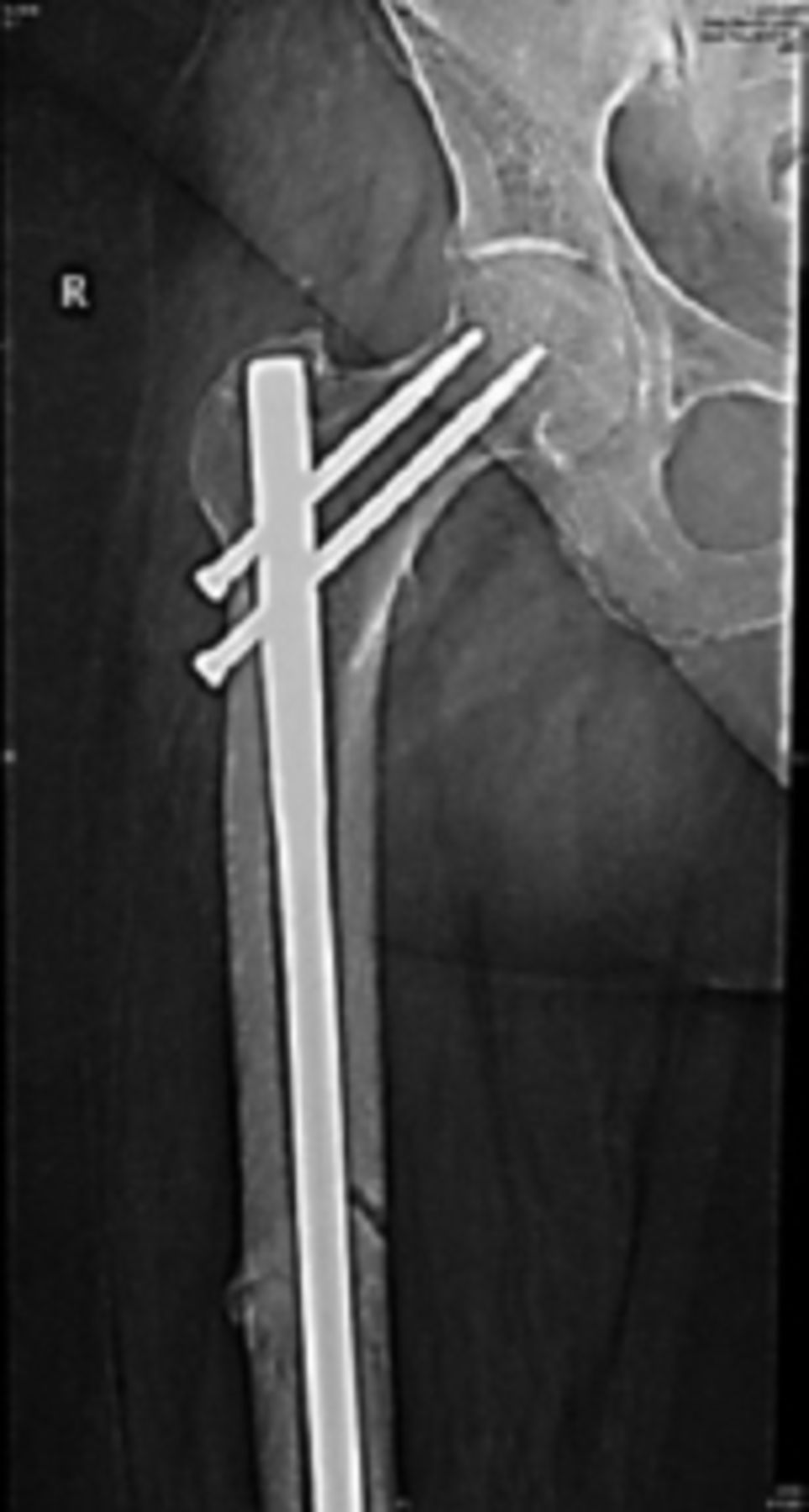
Thirty-four patients were found (33 females, one male). Thirty-three used alendronate (Fosamax, MSD, Fosamax, MSD, USA), are one used ZA 5m (Aclasta, Novartis, Aclasta, Novartis, Switzerland). The patient’s ages ranged between 46-89 years. Reason for referral to the osteoporosis clinic included: Group 1: Review of osteoporosis therapy without new fracture or pain (11 patients). Group 2: patients with a new fracture that occurred after 4 or more years of BP use (21 patients; 20 females, one male), of which 20 used alendronate, and one used ZA 5mg. Group 3: Two patients had chronic severe thigh pain of unknown etiology not responding to analgesia and leading to an inability to walk. Among group 2, 8 patients (38%) were chronic steroid users including the patient on ZA 5mg. All patients were PPI users, none had cancer or used other antiresorptive therapy during or prior to alendronate use. All fractures occurred after at least 4 years of BP use. In the fracture patients, the site included: the femoral shaft in 16 patients (76.1%) (Figure 1), 4 patients (19%) had tibia or fibula fractures (Figure 2), and one patient (4.7%) had a pelvic fracture (Figure 3).

X-rays of 15 patients with atypical fracture femoral: A) transverse fracture of mid femoral shaft with intramedullary nailing, B) transverse fracture of mid femoral shaft with intramedullary nailing and atrophic non-union 10 months after the fracture, C) greenstick fracture of mid femoral shaft, D) displaced oblique fracture of mid femoral shaft, callus formation around the fracture site, with plate, E) comminuted fracture of distal femoral shaft with non-union 9 months after plate fixation, F) hemiarthroplasty in a comminuted proximal hip fracture, G) comminuted mid shaft fracture with wires and non-union 10 months after the fracture. H) displaced comminuted fracture of distal femoral shaft after intramedullary nailing. I) non-union comminuted fracture of proximal femoral shaft with intramedullary nailing. J) transverse displaced fracture of mid shaft in a patient with old operated hip fracture, K) comminuted fracture of distal femoral shaft fixed with a plate in a patient with knee replacement, L) Greenstick fracture of mid shaft with hypertrophid union after intramedullary fixation, M) Greenstick fracture of mid shaft with non union after intramedullary fixation in a patient with knee replacement, N) displaced transverse fracture of mid femoral shaft, O) spiral fracture of proximal femoral shaft.

X-ray showing A) transverse fracture of upper tibia with non-union one year after fracture, B) comminuted fracture of fibuls, and C) & D) greenstick fractures of lower tibia.

X-ray showing A) acute spontaneous pelvic fracture in a 66 years old lady who used alendronate for 15 years, B) non-union of pelvic fracture after one year, and C) healing of pelvic fracture after 2 years of teriparatide.
Figure 1 shows a spiral fracture of the femoral shaft. One patient had AF following 6 years of ZA (Figure 4).
X-ray of a 70-year-old lady with rheumatoid arthritis after 4 years of aclasta. It shows old fracture of right femoral head, intramedullary nailing, recent transverse fracture (greenstick) of femoral shaft and clear cortical thickening.
Figure 2 illustrates x-rays of stress fractures involving tibia and fibula (4 patients).
Figure 3 illustrates an x-ray showing pelvic fracture of a patient who used alendronate for 15 years. Complete healing occurred only after using teriparatide for 2 years. Figures 3A & 3B were taken over 18 months prior to teriparatide,Figure 3C was taken after the teriparatide course. Figure 4 shows a rare case of AFF that followed 4 years of aclasta in a patient with rheumatoid arthritis. Eight patients (38%) had osteoporotic fracture prior to use of alendronate. All of the group 2 patients showed radiological signs of delayed union of fractures at time of presentation. Delayed union is defined as absent of radiological signs of healing 6 months after the fracture (visible fracture line, very little callus formation, or periosteal reaction). An x-ray of the femur of group 3 patients showed marked cortical thickening (Figure 5). All groups 2 and 3 patients (total 23/34) were treated with teriparatide 20 mcg daily for 18-24 months. Sixteen fracture patients completed the teriparatide course (18-24 months), 11 (68.75%) patients showed complete healing of the fracture at the end of the course (Figure 6), 5 patients (31.25%) remained with nonunion of fracture (3 tibiae, 2 femoral shaft), and 7 patients (33.3%) were lost to follow up. Group 3 patients reported marked improvement in pain and the ability to walk, but remained with mild pain 3 years after completing teriparatide. Bone density using a bone density measurement scan at the time of presentation showed osteopenia in 6 patients in group 2 patients, and all of the group 3 patients. There was osteoporosis in 15 of the group 2 patients.

X-ray femur of a 66 years old lady complaining of chronic severe thigh pain after receiving alendronate for 10 years. It shows marked cortical thickening.

X-ray ray showing A) left displaced fracture of mid femoral shaft with non-union six months after surgery and B) healing of the fracture after 2 years of teriparatide. Screw are removed.
Discussion
This report supports the previously perceived belief that prolonged use of alendronate may increase the risk of developing AFF. It is hypothesized that long-term alendronate use results in over suppression of bone turnover (a state of frozen bone), leading to an accumulation of microdamage and increased susceptibility to low trauma fracture. This has been shown in animal studies.11,12 Suggested risk factors are use of PPI, cancer, or simultaneous use of other antiresorptive drugs. Neither presence of previous fractures, nor bone density results can predict the risk of atypical fractures. All patients in our report are PPI users. It is not possible to assess risk of AFF in postmenopausal osteoporosis after prolonged use of BPs. It is probably beneficial to study the pre-treatment state of bone turnover. Do patients with low bone turnover have higher risks?
Figure 1 shows an unusual spiral fracture of the upper femoral shaft. This patient had all the major and the minor features required to satisfy the case definition of AFF required by the ASBMR taskforce.8 The report excluded intertrochanteric fractures with spiral subtrochanteric extension from the criteria of AFF. Schneider21 reported a patient who suffered a spiral fracture of the upper femur. She used alendronate for 7 years prior to the fracture. If similar reports are reported in the future, the ASBMR should revised their definition of AFF to include spiral femoral fractures. Chronic severe bilateral thigh pain is not reported as a separate entity that may complicate prolonged use of alendronate. It was rather described as moderate pain during the prodromal phase that proceeds the atypical fracture. Doctors caring for osteoporosis patients should reassess the fracture risk of their patient after 5 years of alendronate or 3 years of ZA use, and give them a drug holiday unless their risk is high. Warning signs, such as thigh pain should alert doctors to consider discontinuing bisphosphonates.
We are also reporting a single case of AFF following prolonged use of ZA 5 mg. We believe that AFF is a class side effect related to prolonged use of BPs, and it is not restricted to alendronate. The cases reported in the literature of AFF after ZA16-18 are either cancer patients or those with other medical problems (for example, thalassemia). In breast cancer patients, the dose of ZA used is 4mg/month. In these 3 reports, none had postmenopausal osteoporosis. Clinicians may need to observe patients using other BPs or other antiresorptive medications. We propose to use the term “over-suppression syndrome” in these patients as a spectrum syndrome that ranges from severe thigh pain or radiological evidence of cortical thickness at the femur to atypical non-spinal fracture either femoral or elsewhere. This may help to predict which patients will fracture. We suggest carrying out routine x-rays of the thigh to measure cortical thickness in these patients after 2-3 years of therapy. Fukuda13 reported a patient who achieved union of a bilateral AFF after 3 months of only once-weekly administration of teriparatide 56.5 mcg/week. The benefits of treating AFF with teriparatide have been shown in many other reports.14,15 Tibia fractures respond poorly to teriparatide therapy.
Being the sole anabolic agent among osteoporosis medications, teriparatide activates bone remodeling, stimulates osteoblasts required for proper bone healing, and reverses the over-suppression that is induced by bisphosphonates, which is considered the main pathophysiology underlying AFF. The American Society of Bone and Mineral Research updated their report on AFF.19,20 They included a new case definition of AFF, it also stated that there is inconsistent evidence that teriparatide may advance healing of AFFs. We believe that the use of anabolic therapy is beneficial in AFF as no alternative medical therapy is available. Use of teriparatide in AFF remains “off-label.” Whether prophylactic nailing and/or teriparatide can be used in these cases to relieve pain, prevent development of fracture, and the reverse process needs further research. In the absence of other measures, clinicians may have low thresholds to use teriparatide in these cases.
In conclusion, clinicians managing patients with osteoporosis should be aware of the risk of AFF after prolonged use of BPs. They should be aware of the symptoms that may predict AFF like thigh pain as it may reflect over-supression of bone resorption caused by prolonged use of BPs. Further research is needed regarding the use of teriparatide in patients with AFF or even chronic thigh pain not responding to analgesia. Until then, its use in such cases remains off-label.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received December 17, 2016.
- Accepted February 15, 2017.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}