


Abstract
Objectives: To evaluate the potency of Manuka honey UMF +15 against Carbapenem-resistant Enterobacterales (CRE). Bacterial resistance is a worldwide problem that is increasing year by year, especially Carbapenem resistance. Alternatives to antibiotics are needed to both reduce costs, and to reduce the spread of antibiotic resistance, with the ultimate goal of saving lives.
Methods: The efficacy of Manuka honey UMF +15 was tested by 2 methods; Well diffusion assay and minimum bactericidal concentration (MBC) against twenty Carbapenem-resistant isolates which collected from Makkah city hospitals during three months of study from 1st of September 2023 up to 1st of December 2023.
Results: The growth of all isolates of Carbapenem-resistant Enterobacterales (CRE) was severely inhibited by low concentrations of Manuka honey, affecting 25% of isolates at 15% and 75% of isolates at 18% of Manuka honey. In addition, using the honey at different concentrations in a well diffusion assay resulted, as expected, in a variable zone diameter, ranging from large zones(14mm) to small zones (2 mm) according to the concentration of the honey.
Conclusion: This study shows the remarkable antibacterial activity of Manuka honey and suggests that this natural remedy might be used in the future as an alternative treatment option against Carbapenem-resistant Enterobacterales (CRE); however, further clinical trials should be performed to corroborate our initial findings.
Resistance among enteric bacteria has become a serious threat in the medical field, putting patients’ lives at risk. Carbapenem-resistant Enterobacterales (CRE) is a term used for Enterobacterales bacteria that have developed resistance to the Carbapenem group of antibiotics. Carbapenem-resistant Enterobacterales are resistant to most available antibiotics, especially those commonly used, so there is an urgent need to find alternatives. Other Carbapenem-resistant bacteria also show exceptional resistance to multiple antibacterial agents, and they are rapidly spreading across the world.1 Multi-drug-resistant (MDR) bacteria are responsible for high rates of mortality and morbidity throughout the globe. The United Nations (UN) has projected that, in 2050, the mortality rate due to MDR pathogens might exceed 10 million per year.2 The need to find alternatives to antibiotics is increasing in order to minimize the development of resistance and the cost of treatment in the future. Manuka honey is one of the trendiest proposed cures for antibacterial resistance, and its medicinal potential has been widely studied in the last decade. Manuka honey has remarkable activity against bacteria because of its acidity, osmolarity, hydrogen peroxide content, phenolic acid compounds, flavonoids and characteristic compounds, such as methylglyoxal.3-7 Manuka honey has already been shown to be successful in the treatment of certain ailments such as wounds, abdominal pain, ulcers and burns.8,9 Girma et al,10 proved that Manuka honey has widespread effectiveness against multi-drug-resistant Gram-negative bacteria. In addition, a minimum concentration of Manuka honey was found to inhibit the growth of highly resistant bacteria such as methicillin-resistant Staphylococci.11,12 The use of honey has recently become more acceptable to both the general public and practitioners.13 Broadly, there are 2 types of honey: non-peroxide-based and peroxide-based honey. The first type is the most desired for use in medical applications because it has the ability to inhibit microorganisms in the presence of catalase (an enzyme that breaks down hydrogen peroxide, which is produced by some types of bacteria, notably S. aureus), whereas the second type lacks this capability.14 Jelly bush honey from Australia and Manuka honey from New Zealand are 2 examples of non-peroxide honeys. The unique factor in Manuka honey is methylglyoxal (MGO), which is responsible for the honey’s efficacy against bacteria.15 Furthermore, the unique Manuka factor (UMF) is a standard for the level of antibacterial agent possessed by Manuka honey which is ranged between +5 up to +34 so far.
The overall objective of the present study was to evaluate the effectiveness of Manuka honey against different strains of CRE in-vitro. This resulted in the discovery of new and natural alternatives to conventional therapy.
Methods
This experimental study was carried out in the regional laboratory of Makkah city, where Manuka honey UMF +15 (Comvita®, New Zealand) was tested for its efficacy against 20 samples of highly resistant bacteria. Experiments were repeated with different batches of manuka honey UMF +15 to rule out effects of potential ingredient variations in the experimental observations. Manuka honey UMF +15 was tested on Luria broth (LB) agar plates to determine its sterility. The samples of bacteria were collected from patients from hospitals in Makkah Al Mukaramah during the 3-month period of the study from 1st of September 2023 up to 1st of December 2023.
Bacterial identification and minimum inhibitory concentration (MIC) determination
Bacterial species were identified using polymerase chain reaction-based kits. Klebsiella pneumoniae ATCC 25218 and Escherichia coli ATCC 700603 were used as control strains. Ethical approval was obtained from Ethics Committee of the Ministry of Health, Saudi Arabia.
Each individual isolate of bacteria was tested for its minimum inhibitory concentration (MIC) using Vitek2® (bioMerieux, USA), which defines sensitivity to antibiotics, such as those of the penicillin, cephalosporin, aminoglycoside and Carbapenem groups. Highly resistant Enterobacterales, especially those resistant to Carbapenems (Ertapenem, Imipenem, and Meropenem, as stated in the CLSI 2022 guide), were obtained and reserved on slant agar until final testing against honey.16
Carbapenemase detection
All isolates were tested for the presence of Carbapenemase hydrolytic enzymes using a system obtained from NG-BIOTECH® that can rapidly detect the presence of all 3 classes of Carbapenemase hydrolytic enzymes expressed by Carbapenemase producing bacteria. The NG-TEST®/CARBA-5 was used as a confirmation test for carbapenemases possession. The test is a swift in-vitro multiplex immunochromatographic for the phenotypic differentiation and detection of 5 common carbapenemase families (OXA-48-like, IMP, KPC, VIM and NDM) directly from bacterial colonies.
Well diffusion assay
A well diffusion assay was performed as described by Qamar et al.17 In brief, sterile Muller–Hinton agar (20 ml) plates were inoculated with previously calibrated inoculum of bacteria adjusted to 0.5 McFarland before each test using DensiCHEK Plus®. Concentrations of 100%, 80%, 50%, and 30% of Manuka honey were prepared by dissolving the honey in sterile peptone water at 40 degrees (°) C for 30 minutes. Three wells of 8.0 mm in diameter were cut and filled with the previously mentioned concentrations of honey and placed in an incubator for 24 hours at 37°C. The plates were examined after the incubation period for circular, clear inhibition zones around the wells, which were then measured (Figure 1).

- Zones of inhibited bacterial growth due to the presence of Manuka honey in different concentrations 50%, 80% and C (concentrated - 100%).
Minimum bactericidal concentrations (MBC)
This was performed as a bacterial suspension prepared for each isolate of bacteria in sterile peptone water and calibrated to equalize it to 0.5 McFarland turbidity standards. Then, it was mixed with diluted Manuka honey with a concentration of 80% to obtain final concentrations of 40%, 30%, 20%, 18%, 15%, 13% and 10%. The mixtures were incubated at 37°C with shaking at 250 rpm for 24 hrs. All tubes were streaked out on MacConky agar, taking a loopfull (approximately 10 µl) of the mixture and leaving it overnight at 37°C. The lowest concentration, which showed no growth on the agar plate, was defined as the minimum bactericidal concentration.
All experiments were performed in triplicate by different technicians to get reliable (mean and Standard deviation). Collected data were plotted on Excel sheets to display the results and graphs. A descriptive statistical analysis was performed using Excel software. The results are presented as mean values and standard deviations.
Results
A total of 20 Carbapenemase-producing isolates of Enterobacterlaes, including Escherichia coli (n=4), Klebsiella pneumoniae (n=14), and Klebsiella ozaenae (n=2), were isolated from hospitalized patients in hospitals of Makkah city, and number of isolates were reduced because there are restrictions by the Ministry of Health on highly resistant bacteria, reduce expenses and duration of research. Testing revealed that all of the tested isolates (n=20) produced Carbapenemase hydrolytic enzymes. This was verified by the minimum inhibitory concentration (MIC) tests for ertapenem, imipenem and meropenem, as shown in Table 1.
- Summary of used strains of Enterobacterales, enzyme possession and minimum inhibitory concentration (MIC) of those bacteria.
In addition to the antibiotics mentioned in the table, the isolates were resistant to β-lactam antibiotics, including cephalosporins, Carbapenems, β-lactam inhibitors, macrolides and quinolones.
Well diffusion assay
Manuka honey UMF +15 remarkably inhibited the growth of Carbapenem-resistant Enterobacterales (Table 2). A concentration of 30% had no efficacy on any of the isolates or control strains, whereas the other concentrations of honey had gradual effects on the isolates, from the lowest of 50% up to 100%, which is logically accepted.
- Zones of inhibition in mm (mean ± standard deviation) in response to different concentrations of Manuka honey UMF +15.
Minimum bactericidal concentration (MBC)
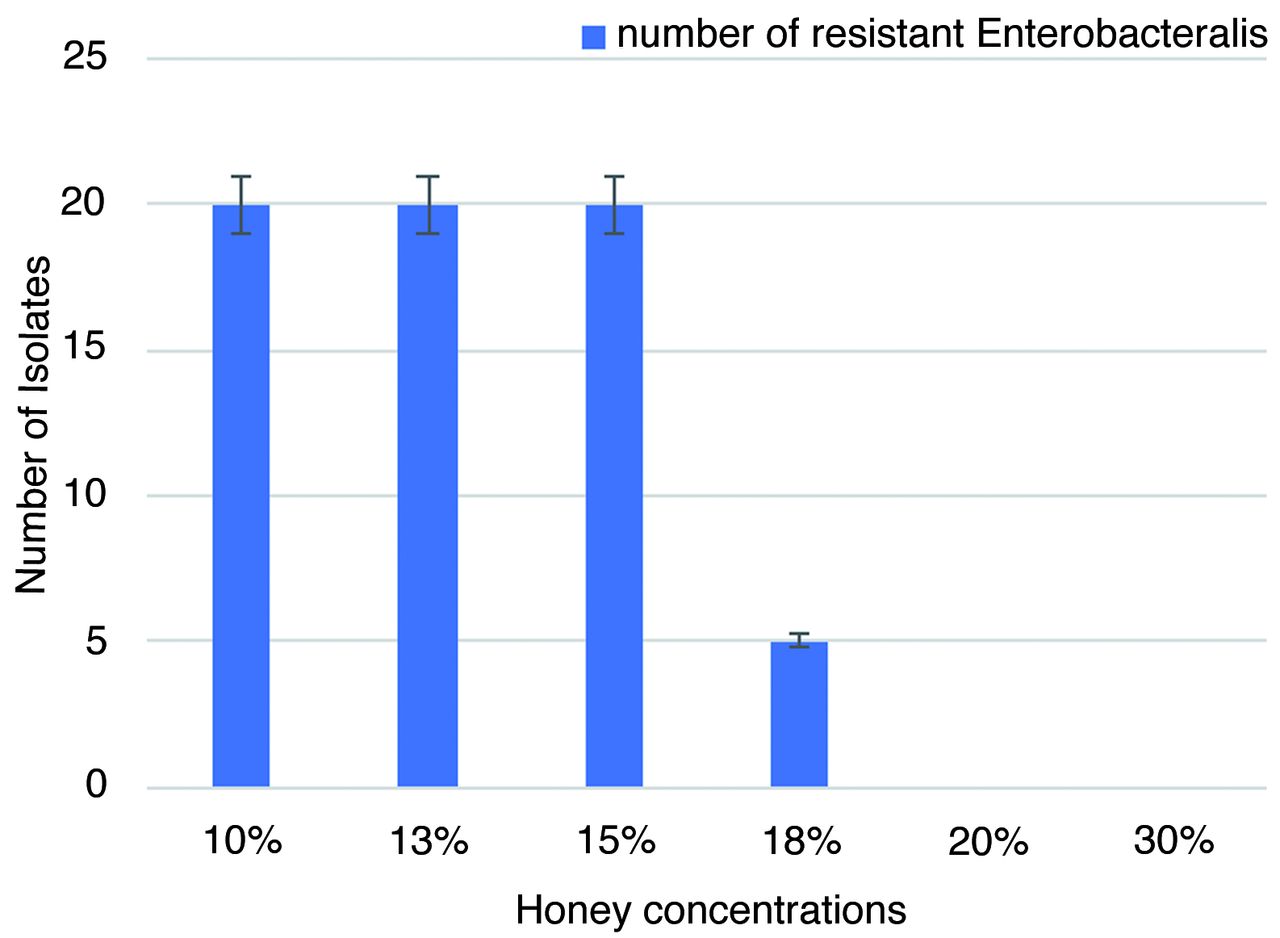
Studies of the minimum bactericidal concentration (MBC) of the Manuka honey for the tested isolates revealed that all isolates were affected at a concentration of at least 20%, but not at 15% (Figure 2). The effect on growth at a concentration of 18% Manuka honey varied among isolates, although most of the isolates (n=15) were highly affected.

- Susceptibility of Carbapenem-resistant Enterobacteralis to different concentrations of Manuka unique Manuka factor +15 honey.
Discussion
Currently, only some types of honey are considered medical-grade and therefore suitable for medical applications; one of these is Manuka honey. Many studies have confirmed the ability of different types of honey, including Manuka honey, to affect a range of pathogenic bacteria including Carbapenemase-producing bacteria.17-19 Based on previous studies, this research was designed to consolidate the use of medical honeys in medical therapy. This study shows that Manuka honey has remarkable antimicrobial activity against different isolates of Enterobacteralis, whose presence was verified by their ability to produce Carbapenemases. This result is in agreement with that of Stavropoulou et al,20 who found that, among many types of honey, Manuka honey has the highest efficacy against highly resistant Gram-negative bacteria, including Carbapenem-resistant Enterobacterales (CRE). These results might be due to various factors: the osmotic effect, the acidic nature of honey, the sensitivity of these organisms to hydrogen peroxide and the activity of the unique factor methylglyoxal. Manuka honey UMF +15 was chosen in this research as some researchers indicated that honey graded UMF +15 and above has the best antimicrobial activity against highly resistant bacteria (Girma et al.18 2019, & Nolan et al.19 2020)
A 100% concentration of Manuka UMF +15 honey was found to be the most effective against all isolates of Carbapenem-resistant Enterobacteralis, and the lowest concentration that affected the growth of the tested bacteria was 50%; these results are similar to those of a study conducted by Adeleke et al,21 who observed 100% inhibition of P. aeruginosa and 96.4% inhibition of E. coli. However, some studies found a high efficacy against bacteria at lower concentrations (less than 100%) due to the excessive production of hydrogen peroxide.22 Furthermore, the variation in zone diameter for the strains might be attributable to the ability of the bacteria to resist the honey or its components, as some isolates showed resistance when a 50% concentration of honey was used, while most isolates were similarly inhibited at the same concentration.
The Manuka honey UMF +15 was evaluated using the minimum bactericidal concentration (MBC) instead of the minimum inhibitory concentration (MIC) because the results for the latter could not be clearly observed. In addition, the minimum bactericidal concentration (MBC) reflects the ability of honey’s killing factors to eradicate all bacterial cells. The findings of the present research show the remarkable activity of Manuka honey UMF +15 at low concentrations of 18% (n=15) and 20% (n=20) against CRE. However, Nolan et al,16 demonstrated different findings, as they obtained a minimum inhibitory concentration (MIC) range of 21% (w/v) to 39% (w/v) for Comvita Manuka honey 15+. In a study by Girma et al,10 different grades of Comvita Manuka honey (UMF +5, +10 and +15) were tested against different types of CRE, such as Klebsiella pneumonia and Escherichia coli, and it was found that Manuka 15+ had the lowest MIC among the grades. In addition, it appears that the drug resistance status of the isolates does not affect the killing activity of Manuka honey, which is in agreement with the results obtained when control strains of the same species of Enterobacteralis were tested in this research. Different concentrations of Manuka honey had the same effects on both the control strains and the tested CRE strains.
In conclusion, many studies have examined Manuka honey in the last decade, and their results support the use of Manuka honey in medical approaches in the future. This study will help in evaluating the antibacterial activity of Manuka honeys against various resistant pathogenic bacteria in-vitro. Moreover, more in-vivo studies should be performed to further the use of Manuka honey in medical therapy.
Acknowledgment
The authors gratefully acknowledge Multidisciplinary Digital Publishing Institute (MDPI) for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received February 26, 2024.
- Accepted August 12, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.



{kind=link}
{kind=link}