


Abstract
Objectives: To evaluate the accuracy of using routine 2-dimensional (2D) radiographs (panoramic and periapical) when evaluating the position of orthodontic temporary anchorage devices (mini-implants) in the maxilla, and to compare the results to 3-dimensional cone-beam computed tomography (CBCT).
Methods: This cross-sectional study was conducted at King Abdulaziz University, Faculty of Dentistry, Jeddah, Kingdom of Saudi Arabia from February 2014 to January 2015. Panoramic and periapical radiographs were used to examine the position of mini-implants in relation to the adjacent roots. Rating of mini-implants position was performed by 82 dentists from different specialties, using 2 D images according to the following criteria: 1) away from the root; 2) mini-implant tip appears touching the lamina dura; and 3) mini-implant overlays the lamina dura. The results were compared with CBCT findings.
Results: There was no difference between dentists from different specialties when rating the position of the mini-implants (Cronbach’s alpha=0.956). The accuracy of the periapical images was 45.1%, while the panoramic images 33.6%. However, both panoramic and periapical radiographs were significantly inaccurate when assessing the mini-implant position when compared with the CBCT findings (p=0.0001).
Conclusion: Three-dimensional CBCT technology allows better visualization of mini-implant placement. The use of CBCT when assessing the position of mini-implants is recommended.
In recent years, orthodontic skeletal anchorage devices are becoming a mainstream orthodontic technique with significant importance being placed on the mini-implant type.1-8 These mini-implants are relatively small to implant with a simple surgical procedure, and can provide absolute anchorage without patients’ cooperation.1 The success rate of the inserted mini-implants is affected by several factors, including the insertion angle of the screw, insertion procedure, inter-radicular bone thickness, and accurate positioning.9-15 Several methods were introduced to ensure the proper placement of mini-implants to avoid any unwanted injury of the adjacent roots, or vital structures.13,16,17 These methods include several designs of custom-made wire guides/jigs to ensure proper positioning of the mini-implants, however, these wire guides require additional steps involving additional x-rays to evaluate placement position. These surgical guides/jigs are usually evaluated with 2-dimensional (2D) radiographs (for example, periapical, bitewings, and/or panoramic). Panoramic and periapical x-rays have been in use for several decades in dentistry. However, their reliability is limited by how it presents 3 dimensions in 2. Moreover, its reliability is further compromised by the magnification and distortion of the image.18,19 Recently, cone-beam computed tomography (CBCT) has gained considerable acceptance in orthodontic diagnosis and treatment planning, and to assess pre- and post-treatment dento-skeletal relationships.20,21 Moreover, it was suggested that CBCT could be used routinely in orthodontics for diagnosis and treatment planning to reduce the repeated radiation exposures when acquiring conventional 2D images and the amount of clinical information obtainable from 3-dimensional (3D) images.22 Furthermore, CBCT technology facilitates the evaluation of the position of inserted mini-implants in relation to adjacent structures.16,23 However, Garib et al24 in a recent review argued that some still do not consider CBCT as a standard diagnostic tool in orthodontics. Despite the increasing use of mini-implants in orthodontics, limited data are available in the literature to recommend the most appropriate diagnostic tool for determining mini-implant position. Therefore, this study was aimed to compare the accuracy of routine panoramic and periapical versus CBCT when assessing the position of mini-implants. Also, whether specialty background would influence the assessment of mini-implant position in the panoramic and periapical images.
Methods
This cross-sectional study was carried out from February 2014 to January 2015 at King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia. The study was reviewed and approved by the Research Ethics Committee of the Faculty of Dentistry, King Abdulaziz University, and was conducted in accordance with the principles of the Helsinki Declaration. An informed consent was obtained from participants prior to their enrollment. Orthodontic patients (age ranged between 20-30 years) who were undergoing treatment in the Department of Orthodontics, Faculty of Dentistry, King Abdulaziz University were selected based on the following inclusion selection criteria: 1) patients who had mini-implant place distal to the maxillary canine; 2) good quality panoramic and/or periapical radiograph post mini-implant placement; 3) CBCT scans taken after mini-implants were placed; and 4) one type and size of mini-implant used. Exclusion criteria were: 1) age less than 20-years-old; 2) presence of moderate to severe periodontitis; 3) severe crowding, 4) congenitally missing teeth; and 5) congenital abnormality in the maxilla.
All mini-implants (OrthoEasy system, Forestadent, Pforzheim, Germany) were self-tapping self-drilling, 1.7 mm in diameter and 8 mm in length. They were inserted using a hand driver under local anesthesia. Mini-implants were inserted into the buccal attached gingiva just adjacent to the mucogingival junction and midpoint between the roots of the adjacent teeth. Custom-made wire guides were fabricated to ensure proper positioning of the mini-implants.
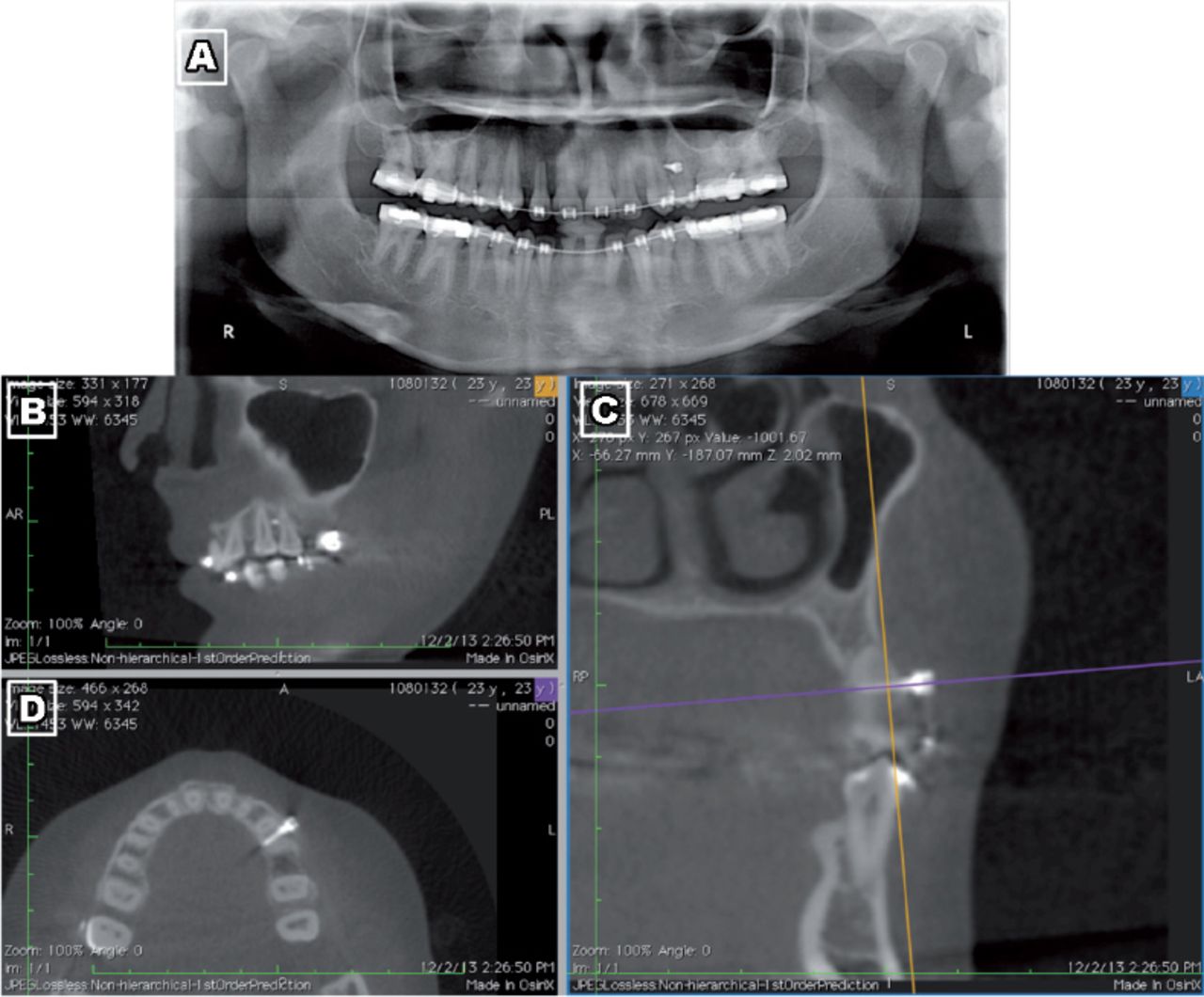
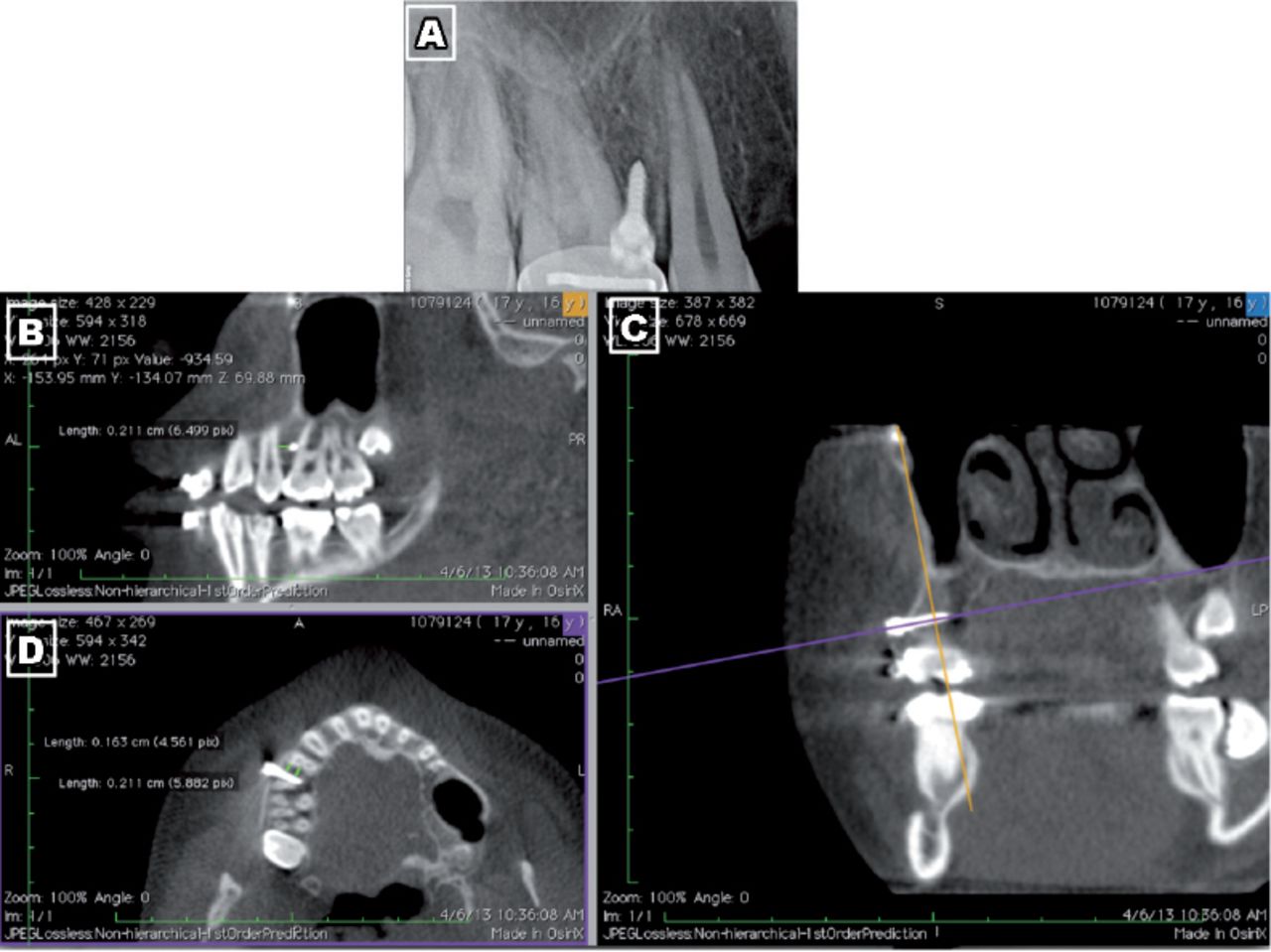
Panoramic images were taken using the Kodak 8000C digital panoramic, and cephalometric system and periapical images using the Kodak Carestream RVG 5000 digital sensor (Kodak-Trophy, Croissy-Beaubourg, Marne-la-Vallée, France). The paralleling technique was used for all periapical x-rays. The CBCT images were obtained using the i-CAT cone-beam 3D dental imaging system and software (Imaging Sciences International, LLC, Hatfield, PA, USA). Figures 1 and 2 show an example of a panoramic/periapical images and their corresponding CBCT images. Dentists from various specialties were asked to assess 13 images (6 panoramic and 7 periapical radiographs). Each dentist was asked to rate the position and proximity of each mini-implant in relation to the adjacent roots, according to the following criteria: 1) away from the root; 2) mini-implant tip appears touching the lamina dura; and 3) mini-implant overlays the lamina dura. The 2D images (panoramic x-rays and periapical x-rays) for the inserted mini-implants were uploaded on an iPad (iPad-2, Apple Inc., Cupertino, CA, USA). The iPad was chosen because of its ease of use and ability to magnify the images to allow the dentists to evaluate and rate the mini-implant position and its relationship to the adjacent roots. All dentists were blinded to the patients’ information and were only requested to evaluate the mini-implant position. All CBCT images were analyzed by one investigator who is a maxillofacial radiologist. This investigator measured the proximity of each mini-implant to the adjacent roots, and the results were used for comparison with the results collected from the other raters.

Panoramic radiograph used to determine the mini-implant position (A). Cone-beam computed tomography images for the same mini-implant where the apex of the mini-implant was determined on the sagittal plane (B), coronal plane (C), and horizontal plane (D).

Periapical radiograph used to determine the mini-implant position (A). Cone-beam computed tomography images for the same mini-implant where the apex of the mini-implant was determined on the sagittal plane (B), coronal plane (C), and horizontal plane (D).
Statistical analysis
Statistical analysis was performed using the IBM Statistical Package for Social Sciences version 20 (IBM Corp., Armonk, NY, USA). Cronbach’s alpha was used to evaluate inter-rater consistency. Chi square and McNemar’s tests were used to evaluate the rating between CBCT and panoramic or periapical images. Raters’ accuracy was also evaluated. P-value of <0.05 was considered significant.
Results
A total of 82 dentists from 6 specialties participated in this study (Table 1). Thirteen images, 6 panoramic and 7 periapical x-rays were used to assess the location of mini-implants after insertion. There was a significant agreement between dentist when rating the position of the mini-implant to the adjacent roots, Cronbach’s alpha=0.956. Therefore, the accuracy of the assessment is relatively the same with respect to the specialty of the raters. Table 2 shows the comparisons between the accuracy of each discipline when rating the proximity of the mini-implant to the roots and the results of the CBCT readings. These results showed that the accuracy to detect the correct position of the mini-implant by the raters was between 58% to 64% when using both panoramic and periapical radiographs. As shown in Table 3, the accuracy of the periapical images was 45.1% compared with the panoramic images (33.6%). However, the McNemar test showed that there were significant differences between the CBCT and both the panoramic and periapical ratings, p=0.0001, therefore, both panoramic and periapical radiographs were not significantly accurate when assessing the position of mini-implants.
Summary of raters and their disciplines.
Results of each discipline when compared with the cone-beam computed tomography (CBCT) readings.
Comparison between the accuracy of periapical and panoramic images.
Discussion
During the last 2 decades, numerous studies have reported the success and acceptance of mini-implants in facilitating orthodontic mechanics.5,6,25 In this respect, orthodontic treatment has been increasingly affected by the success, or failure of orthodontic mini-implants due to the increasing frequency of their use.26,27 In a clinical situation, during mini-implant placement, a patient under minimum infiltration anesthesia could still feel discomfort during insertion of mini-implant, if it contacts the adjacent root surface, and the practitioner can easily change the placement direction to minimize root contact. Even though contact between mini-implant and root may cause injury, after discontinuation of the contact, repair does occur.28 However, mini-implant overlapping or touching of the lamina dura of roots is considered a risk factor for mini-implant failure.13 This study evaluated the accuracy of using conventional periapical or panoramic radiographs for the assessment of mini-implant placement in the posterior maxilla. The findings of the current study showed that conventional 2D radiographs were inferior in detecting the accurate positions of mini-implants after its insertion when compared with the CBCT method.
The radiographs used in the current study were for mini-implants inserted distal to the maxillary canine because this is considered a preferable site and ease of accessibility for various orthodontic mechanics.5,6,8,29,30 Moreover, the current study assessed the actual final position of mini-implants in relation to the root proximity using CBCT, which previously could not be carried out using conventional 2D, radiographs.16 The CBCT data allowed for accurate localization of the mini-implant position and assessment with regard to bone contact, bone penetration, and iatrogenic consequences.31,32 This accuracy of the CBCT method was attributed to its precise 0.15-mm3 voxel-size 3D images. In this study, 7 of the cases had the apex of the mini-implant touching the lamina dura and 6 of the cases were diagnosed as the mini-implant body overlaying the lamina dura. Therefore, all cases had their mini-implants diagnosed by the CBCT as having high risk of failure due to their proximity to the teeth lamina dura. Interestingly, patients did not report any pain or discomfort during the placement of the mini-implant, and therefore tooth root proximity was not suspected. Moreover, almost 40% of the raters failed to accurately diagnose the position of the mini-implant, hence the possible high risk failure. This indicates that there is great difficulty in diagnosing the position of the mini-implant from the 2D imaging. This study suggests that although there is apparently enough space, still mini-implants can cause damage to root structures, and possible failure might occur. This is in agreement with previous studies,33,34 even when the amount of space between roots was increased by 100%, contact with periodontal ligament was still high at 65.7%. Therefore, despite all the good intentions and care by clinicians, a more robust delivery system incorporating the 3D anatomy of the tooth might be needed.33,34
In previous studies,13,17,35 it was demonstrated that root contact with mini-implants was extremely difficult to be diagnosed using 2D radiography, and suggested that the use of CBCT method is of greater value for determining the accurate positioning of mini-implants after its insertion.13,35 This is also in agreement with Bennemann et al36 who concluded that panoramic x-ray enabled poor evaluation of mini-implant position and CBCT was more advantageous before surgical placement particularly if there is risk of root damage. When comparing the 2 types of 2D radiographs obtained in our study, the periapical x-ray showed more accuracy in determining the mini-implant position when compared with the panoramic x-ray, which emphasizes the importance of using the periapical x-rays for evaluating the mini-implant’s position when the CBCT method is not available. The findings of the current study demonstrated that specialty of the rater was of minor significance when determining the mini-implant location on the panoramic and periapical images.
One limitation to this study is that the periapical and panoramic images were not for the same mini-implant. Also, only buccally inserted mini-implants in the maxillia were evaluated. Therefore, further longitudinal studies are necessary to assess the position of mini-implants using both 2D and CBCT in different locations, such as the mandible and the palate.
In conclusion, 3D CBCT technology allows for better visualization of mini-implant placement. Both panoramic and periapical images are not accurate enough when assessing the location of mini-implants. The use of CBCT when assessing the position of mini-implants is recommended to avoid potential injury to vital structures and prevent possible mini-implant failure.
Acknowledgment
The authors would like to acknowledge the Deanship of Scientific Research, King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia for their technical and financial support.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company. The project was funded by the Deanship of Scientific Research, King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia (Grant no. 339/165/1433).
- Received May 20, 2015.
- Accepted September 16, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}