


Abstract
Wernicke’s encephalopathy (WE) is a serious neurological disorder characterized by a classical triad of acute mental confusion, ataxia, and opthalmoplegia due to thiamine deficiency. It was initially described in chronic alcoholics; however, any condition resulting in poor nutritional status places the patient at risk of WE. Bariatric surgery is now considered as an emergent cause of WE. The number of bariatric surgery is increasing for morbid obesity. We present a case of a 40-year-old male who presented with confusion and difficulty in maintaining the balance while walking 3 months after Roux en Y gastric bypass surgery. Diagnosis of WE was made on clinical ground and confirmed by magnetic resonance imaging of the brain, which showed bilateral hyperintense signals in paramedian thalami. Parenteral thiamine replacement was started, and patient showed complete recovery.
Wernicke’s encephalopathy (WE) is a clinically acquired condition characterized by mental confusion, ataxia, and opthalmoplegia. If WE is left untreated or diagnosed lately, it may lead to a state of chronic mental dysfunction known as Korsakoff’s syndrome in 85% of survivors.1 Literature review identified 104 reported cases of WE after bariatric surgical procedures and in 80 (95%) cases, gastric bypass was the performed procedure.2 Gastric bypass surgery is one of the most commonly performed bariatric surgical procedures. The operation is prescribed to treat morbid obesity defined as a body mass index (BMI) greater than >40 kg/m2 with no obesity related comorbidities and BMI > 35 kg/m2 with obesity related complications as hypertension, type 2 diabetes mellitus, dyslipidemia, and/or obstructive sleep apnea (who failed conservative treatment).3 Aside from weight loss, these procedures are associated with improvement in obesity related co morbidities as well. However, these procedures are associated with a number of complications, among which neurological complications are not uncommon. We present a case of WE who presented 3 months after Roux en Y gastric bypass. The aim of reporting this case is to increase the awareness on this rare and often underdiagnosed complication of gastric bypass.
Case Reports
Forty-year-old right handed male, shopkeeper with no previously known comorbidities and insignificant past history was admitted with complaints of gradually increasing confusion, disorientation, and difficulty in maintaining balance for past 2 months. He had Roux en y gastric bypass surgery 3 months prior to his presentation. He remained well postoperatively apart from recurrent episodes of vomiting. After about one month, the family noticed that he was not replying relevantly to questions and had difficulty in concentration and recognizing the family members. He remained independent for his basic activities of daily living. Initially, the episodes were short, but gradually over time his symptoms deteriorated and he became disoriented to time, place, and person. Subsequently, he developed difficulty in walking due to inability to maintain his balance. There was no history of fever, seizures, hallucination, and impairment of conscious level. He had no history of recent travel abroad and exposure to tuberculosis. There was no history of alcoholism, or other substance abuse, and family history was unremarkable.
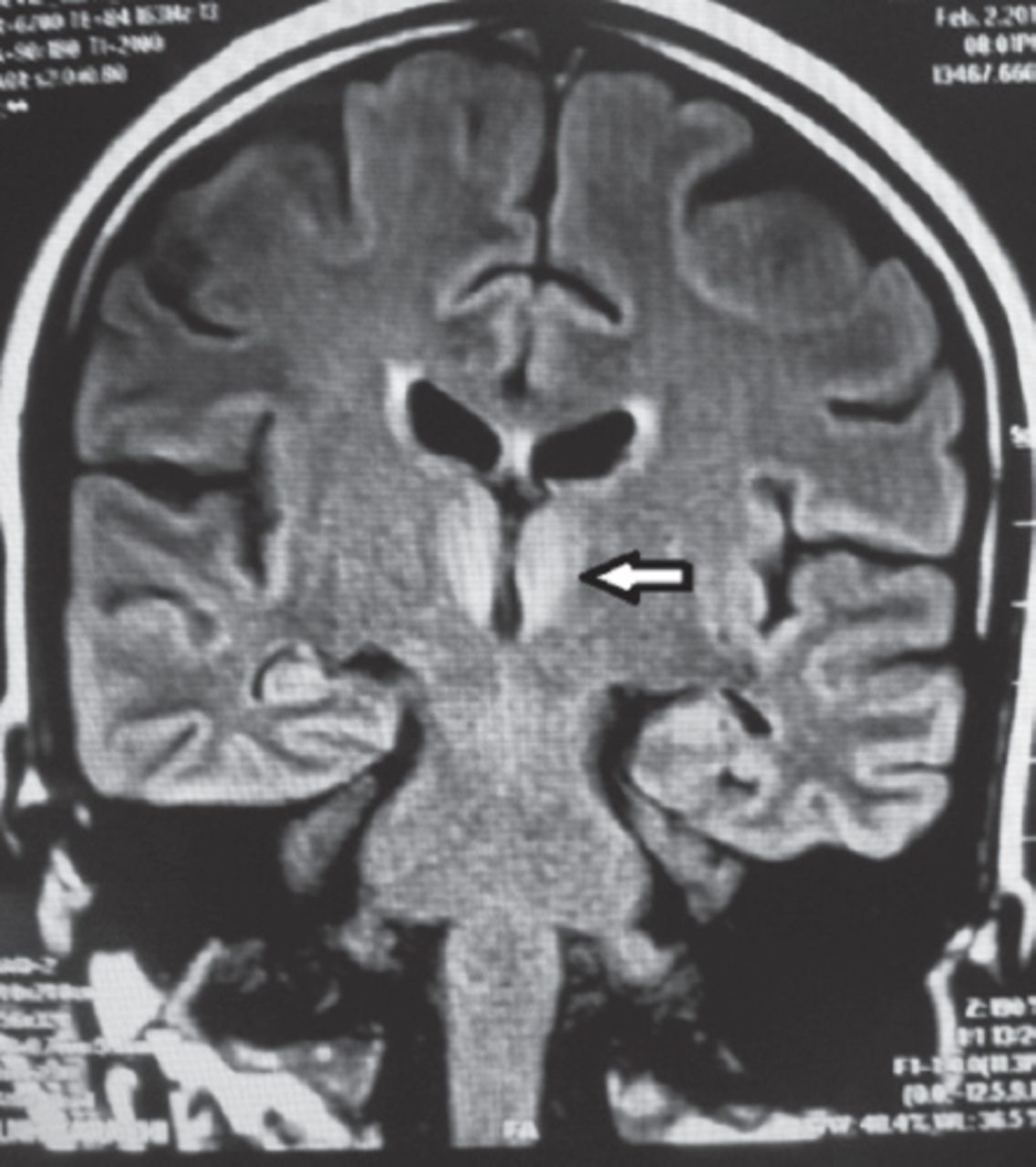
On examination, he had normal blood pressure, pulse and temperature. He was fully conscious, but disoriented to time, place, and person. Cranial nerves were intact, and fundus examination was normal. Tone, power, deep tendon reflexes were normal in all 4 limbs. He had bilateral horizontal nystagmus; mild finger nose incoordination and broad based ataxic gait. Diagnosis of WE was made on clinical grounds, and he was admitted for further workup and management. His routine investigations (complete blood count, blood glucose level, renal function tests, liver function tests, erythrocyte sedimentation rate, urine analysis, and chest x-ray) were normal. Thyroid function tests and vitamin B12 level were also normal. Magnetic resonance imaging of the brain was carried out and it showed bilateral hyperintense and swollen paramedian thalami on fluid attenuated inversion recovery (FLAIR) image, characteristics of WE (Figure 1).

Fluid attenuated inversion recovery (FLAIR) image showing bilateral hyper intense medial thalami in periventricular region.
Cerebrospinal fluid was carried out to rule out central nervous system infection, and it was also normal. On the basis of history, physical signs, and MRI findings he was finally diagnosed as case of WE. He was started on intravenous thiamine replacement, initially 500 mg 3 times a day then 250 mg daily. Within 3 days, his symptoms started to recover and he was discharged after one week. His replacement therapy was continued, and on follow-up visit after 3 months he was almost completely normal. Wernicke’s encephalopathy is a rare and often under diagnosed complication of gastric bypass surgery. It carries an important prognostic value as if diagnosed and treated timely; patient’s symptoms may recover completely without any neurological deficits. However, delay in diagnosis and treatment leads to adverse outcomes including persistent severe neurological deficits and even death.
Discussion
Wernicke’s encephalopathy is a serious neurological disorder. In 1881, Dr. Carl Wernicke, a Polish neurologist described a syndrome termed polyencephalitis hemorrhagica superioris as an acute encephalopathy characterized by a classical triad of acute mental confusion, ataxia, and opthalmoplegia with autopsy finding of punctate hemorrhage around the third and fourth ventricles, and the aqueduct.4 The disorder has classically been described in chronic alcoholics; however, has also been identified in patients with malnutrition, malabsorption, prolonged fasting, gastrointestinal malignancies, dialysis, hyperemesis gravidarum, AIDS, and bariatric surgery.5
The diagnostic criteria for WE requires 2 of the following 4 features: 1) dietary deficiency, 2) oculomotor abnormalities, 3) cerebellar dysfunction, and 4) confusion or mild memory impairment. This criteria has a very high inter-rater reliability.6
Our patient had all clinical features, which were nystagmus, ataxia, and confusion, and he was at risk of dietary deficiency due to Roux en Y gastric bypass surgery and repeated vomiting. Therefore, the diagnosis of WE was made on clinical ground and thiamine replacement therapy was started immediately. As delay in treatment may lead to development of irreversible chronic amnestic syndrome, Korsakoff psychosis1 in 85% of survivors and even death. Thiamine pyrophosphate is a co-factor in oxidative decarboxylation of carbohydrates. Thiamine deficiency alters mitochondrial function, impairs oxidative metabolism, and causes selective neuronal death by diminishing thiamine dependent enzymes, these changes are predominantly seen in brainstem, which correlates clinically with clinical presentation of WE.7
Thiamine deficiency can be confirmed by assessing the serum thiamine concentration and thiamine pyrophosphate effect in erythrocyte transketolase studies. However, these measurements are limited by a lack of specificity, technical difficulty, and non-availability at many centers.8 Magnetic resonance imaging of the brain is the most valuable method to confirm the diagnosis of WE with the sensitivity of 53% and specificity of 93%. The findings typically seen are bilateral and symmetrical increased T2 signal, in the para ventricular region of thalamus, hypothalamus, mammillary bodies, and periaqueductal region.9 These lesions can show hyperintensity on diffusion weighted images and reduced, normal, or increased ADC (apparent diffusion coefficient) values. The typical pattern of lesions on MRI was observed in 58% of patients with WE.10
Magnetic resonance imaging showed bilaterally, symmetrical hyperintense signals in para ventricular regions of thalami on fluid-attenuated inversion recovery (FLAIR) images, best visualized on coronal sections. Diffusion weighted imaging also showed bilateral and symmetrical high signals at the level of medial portions of both thalami, the findings which are typically seen in WE. Our patient was started on parenteral thiamine replacement and showed good recovery. Every patient undergoing gastric bypass surgery or other surgical procedures putting the patient at risk of malnutrition should have a preoperative counseling regarding the possible complications including the neurological ones, regular follow up and adequate nutritional replacement therapy.
In conclusion, patients having bariatric surgery are at risk of developing WE because of inadequate nutritional replacement. If diagnosed timely and treated adequately, WE carries good prognosis.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received July 1, 2015.
- Accepted September 5, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.