


Abstract
Wandering spleen is a rare condition that accounts for less than 0.25% of all indications for splenectomy. It is characterized by ectopic localization of the spleen owing to the lack or weakening of its ligaments. Torsion is the most common complication due to its long pedicle and high mobility, which may result in acute abdomen. We report a case of torsion in a wandering spleen in a 28-year-old male presenting with an acute abdomen that was treated by splenectomy.
Wandering spleen is a rare condition, which may be incidentally detected as an abdominal mass or can present with torsion of its pedicle causing an acute abdomen. Alternative names are: ectopic spleen, displaced spleen, floating spleen, or pelvic spleen. It is characterized by the absence or underdevelopment of one or all ligaments that hold the spleen in its normal anatomical position in the left upper quadrant of the abdomen.1 It mainly affects children (one-third of cases), with a female predominance after age one.2 Among adults, it most frequently affects women of reproductive age, in whom acquired laxity of the splenic ligaments is usually the cause.2 Due to lack of specific symptoms, diagnosis is difficult, unless there is torsion, presenting as acute abdomen. Radiological imaging is required to make diagnosis; treatment is either splenopexy or splenectomy. We report a case of torsion of wandering spleen in a 28-year-old male presenting with an acute abdomen, which was treated by splenectomy.
Case Report
A 28-year-old undergraduate student was admitted to the emergency department with a 2-day history of generalized abdominal pain. He had been having recurrent, central abdominal pain for 20 years. He vomited shortly before presentation; vomit contained recently-ingested meals, and was non-bilious and without evidence of blood. There was associated anorexia and abdominal distension. There was no history of weight loss, change in bowel habit, blood in the stool or previous abdominal surgery. A review of other systems was normal.
On physical examination, he was acutely ill-looking, in pain distress, febrile, dehydrated, pale, anicteric with neither pedal edema nor peripheral lymph node enlargement. Blood pressure was 120/70 mm Hg (normal range: 120/80 mm Hg), pulse rate was 124/min (normal range: 60-100/min), regular; respiratory rate was 40 cycles/min (normal range: 12-20 cycles per min). The abdomen was distended with multiple scarification marks (Figure 1) as a traditional treatment for enlarged spleen. He had generalized tenderness and guarding, but there was no rebound tenderness or abdominal rigidity. There was a firm, tender, palpable mass extending from the left costal margin into the pelvis. Intra-abdominal fluid was demonstrable by shifting dullness; bowel sounds were present. The remainder of the examination was normal. The complete blood count showed a low hematocrit (34%) (normal range: 42-54%), elevated total white blood cell count (17,000/mm3) (normal range: 4,000 to 11,000/mm3), and thrombocytopaenia (85,000/mm3) (150,000-450,000/microliter). Electrolytes, urea and creatinine and urinalysis were normal. Abdominal ultrasound revealed a massively-enlarged spleen (30 cm in its long axis) with pericapsular fluid collection extending from the inferior margin of the left sub-costal region to the right iliac fossa, and fluid collection in the left paracolic gutter. There was left hydronephrosis. Abdominal computed tomography scan demonstrated absence of spleen in the normal splenic area, soft tissue structure with well-defined borders extending into the pelvis and intra-abdominal fluid, with a conclusion of ectopic spleen.

Distended abdomen with multiple scarifications.
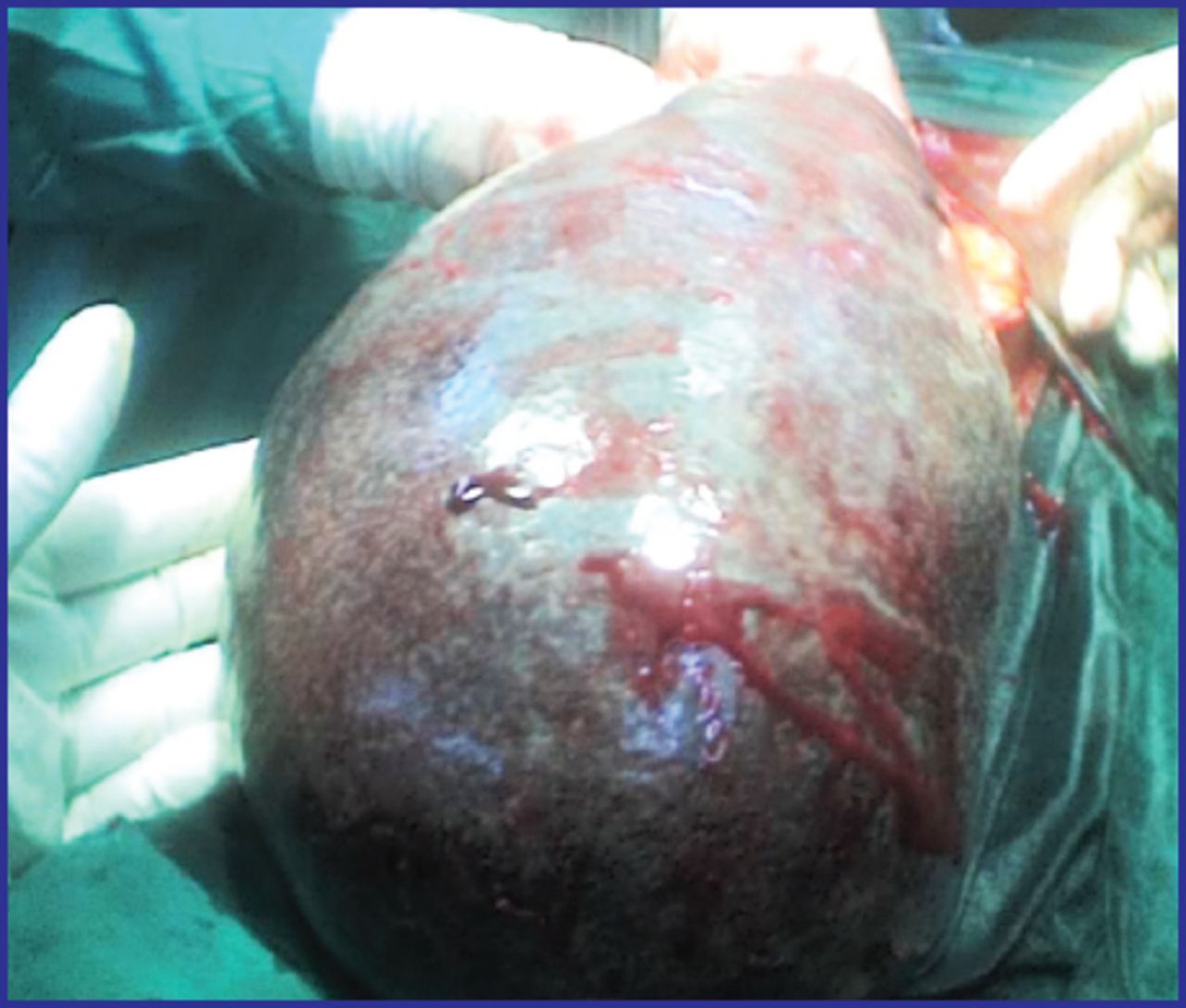
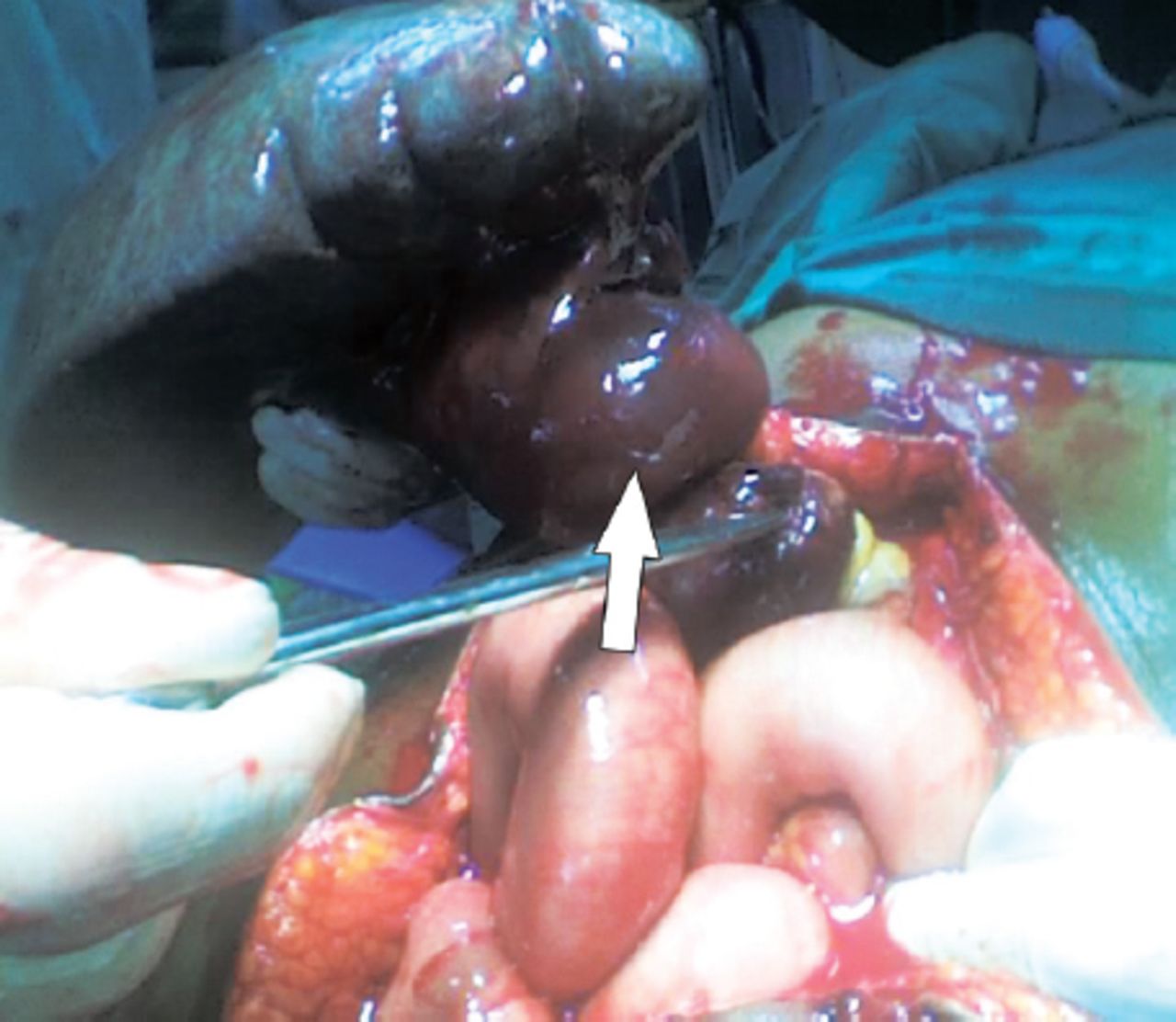
At operation, there was a 1200 ml of hemoperitoneum; a massively-enlarged, pale spleen, with a 20 cm-long pedicle extending into the pelvis, twisted on its pedicle, with dilated vessels (Figures 2 & 3). Splenectomy was performed; the spleen measured 20 × 30 cm and weighed 2300 g. The normal weight of spleen in an adult is 150-200 g. Other organs were normal. Post-operative period was uneventful, and he received vaccination against Neisseria meningitidis, Haemophilus influenzae, and Streptococcus pneumoniae. He was discharged on the tenth day of admission. Histology of the removed spleen showed a severely-congested spleen without evidence of malignancy.

Massively-enlarged spleen observed at operation.

Massively enlarged spleen showing the twisted pedicle.
Discussion
Acute torsion of wandering spleen is a rare cause of acute abdomen. Wandering spleen is most-commonly diagnosed in young children,2 as well as women between the ages of 20 and 40 years.3 This case was unusual in that it occurred in an adult male. Wandering spleen is very rare, with fewer than 500 occurrences of the disease reported on 2005.4 The most common complication of wandering spleen is torsion,5 which was the complication noted in this case presentation. Other complications are splenic infarction, splenic abscess, variceal hemorrhage, and pancreatic tail necrosis.3 The symptoms of wandering spleen may vary from an asymptomatic intra-abdominal mass to acute abdominal signs secondary to splenic torsion. Patients may have intermittent abdominal pain resulting from torsion and de-torsion, which may be similar to the case presented, as the patient had been having recurrent central abdominal pain for 20 years.
Medical imaging is very important in the diagnosis of wandering spleen. Ultrasonography and computed tomography scan of the abdomen are the most useful diagnostic methods and demonstrate absence of spleen in its normal anatomical position, with a comma-shaped structure located elsewhere in the abdomen or pelvis,6 as was observed in the reported case. Treatment of wandering spleen is either splenopexy or splenectomy. Splenopexy is preferred for a viable wandering spleen to prevent any future complications, especially in children.7 In the event of acute torsion with splenic infarction, splenectomy is indicated. Splenectomy was carried out for the patient presented because of splenic infarction and a massively enlarged spleen. The pericapsular fluid collection may be due to inflammatory fluid following splenic infarction while the hemoperitoneum may have been due to splenic vessel rupture following torsion. Other indications for splenectomy in wandering spleen are secondary hypersplenism, functional asplenia, and any suspicion of malignancy.7
In conclusion, torsion of wandering spleen should be considered as a possible cause of acute abdomen in a patient with an acute abdomen whose spleen is absent from its anatomical position on abdominal ultrasound or computed tomography scan with a demonstration of a mass elsewhere in the abdomen or in the pelvis. Increased awareness of this medical condition may help in reducing the incidence of complications.
Student Corner
We invite students from a variety of medical disciplines to submit original contributions based on their supervised research.
The Student Corner of Saudi Med J aims to help students explore research opportunities and network with other peers and mentors in the same field.
Submission Guidelines
Submitted Abstracts should include the following:
Title should be descriptive
Author’s names and affiliation(specify college level/year, academic degree of Senior >Author)
Abstract must be structured and not more than 300 words
The following are the typical headings:
Objectives (background, why the study was done, specific aims)
Methods (setting, date of study, design, subjects, intervention and analysis)
Results (findings, data and statistical tests) and
Conclusion (general interpretation of results)
General Information on Abstract Submission
Submitted Abstracts should be co-authored by a Senior Supervisor
Abstracts will be reviewed by Student’s Corner Section Editor
There is no fee to submit an Abstract
Ethical Approval should be provided
Non-indexed materials
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received June 11, 2015.
- Accepted September 10, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}
{kind=link}