


Abstract
Alkaptonuria (AKU) is a rare inborn metabolic disease characterized by accumulation of homogentisic acid (HGA). Excretion of HGA in urine causes darkening of urine and its deposition in connective tissues causes dark pigmentation (ochronosis), early degeneration of articular cartilage, weakening of the tendons, and subsequent rupture. In this case report, we present a rare case of a patient presented with unilateral spontaneous rupture of Achilles tendon due to AKU. The patient developed most of the orthopedic manifestations of the disease earlier than typical presentations. Alkaptonuria patients should avoid strenuous exercises and foot straining especially in patients developing early orthopedic manifestations.
Alkaptonuria (AKU) is a rare genetic metabolic disorder with an incidence of 1:250,000 in most populations. It is due to deficiency of homogentisate 1,2-dioxygenase (HGD), which is an enzyme involved in the phenylalanine and tyrosine degradation pathway.1,2 Homogentisate 1,2-dioxygenase deficiency results in accumulation of homogentisic acid (HGA), which is oxidized to benzoquinones that polymerize and form a dark pigment. The excess HGA binds to the connective tissues and cartilage. Ochronotic osteoarthropathy is used to refer to the musculoskeletal manifestation of AKU. Ochronosis is the darkening of connective tissues due to the deposition of HGA and/or its polymer in connective tissue. Over time this causes ochronotic osteoarthropathy.3 On microscopic examination yellowish (ocher-like) discoloration of the tissue is seen, but macroscopically the affected tissues appear bluish grey. This leads to weakness and early degeneration of articular cartilage and arthritis.2 Large quantities of HGA excreted in urine causes urine to darken upon standing due to oxidation or after exposure to alkaline agents.1 Rupture of Achilles tendon is an important clinical manifestation of AKU. There are few reports in the literature of spontaneous rupture of the Achilles tendon caused by AKU.4-6 We report a case of an AKU patient presented with a unilateral spontaneous rupture of Achilles tendon. The objective of this case report is to highlight the rare Achilles tendon rupture due to AKU, which can be a reference for physicians and surgeons in the prevention and/or delay of such a complication.
Case Report
A 39-year-old male presented to the Accident and Emergency Department, 7 hours after he developed sudden onset of pain behind the left ankle while climbing stairs quickly. On examination, he had a palpable defect over the left Achilles tendon proximal to its insertion. Clinical examination revealed dark pigmentation of the sclera of both eyes and bluish-grey pigmentation of ears. He had history of severe low back pain, morning stiffness, and pain in his both knees and hips 15 years ago. He had history of renal stones. He had dark urine since birth. His urine turned dark-black in color upon standing for 24 hours (Figure 1). Ferric chloride (FeCl3) test was performed, one drop of ferric chloride solution was added to the urine sample and a transient blue color was observed, this indicated a positive test and suggested the presence of HGA. Confirmation of diagnosis was carried out by quantitative measurement of HGA in 24 hour urine sample using gas chromatography mass spectrometry (GC-MS), which revealed a high level of HGA (0.79 g/24 hour). He has no history of direct injury, no history of fluoroquinolone, or steroid used recently.

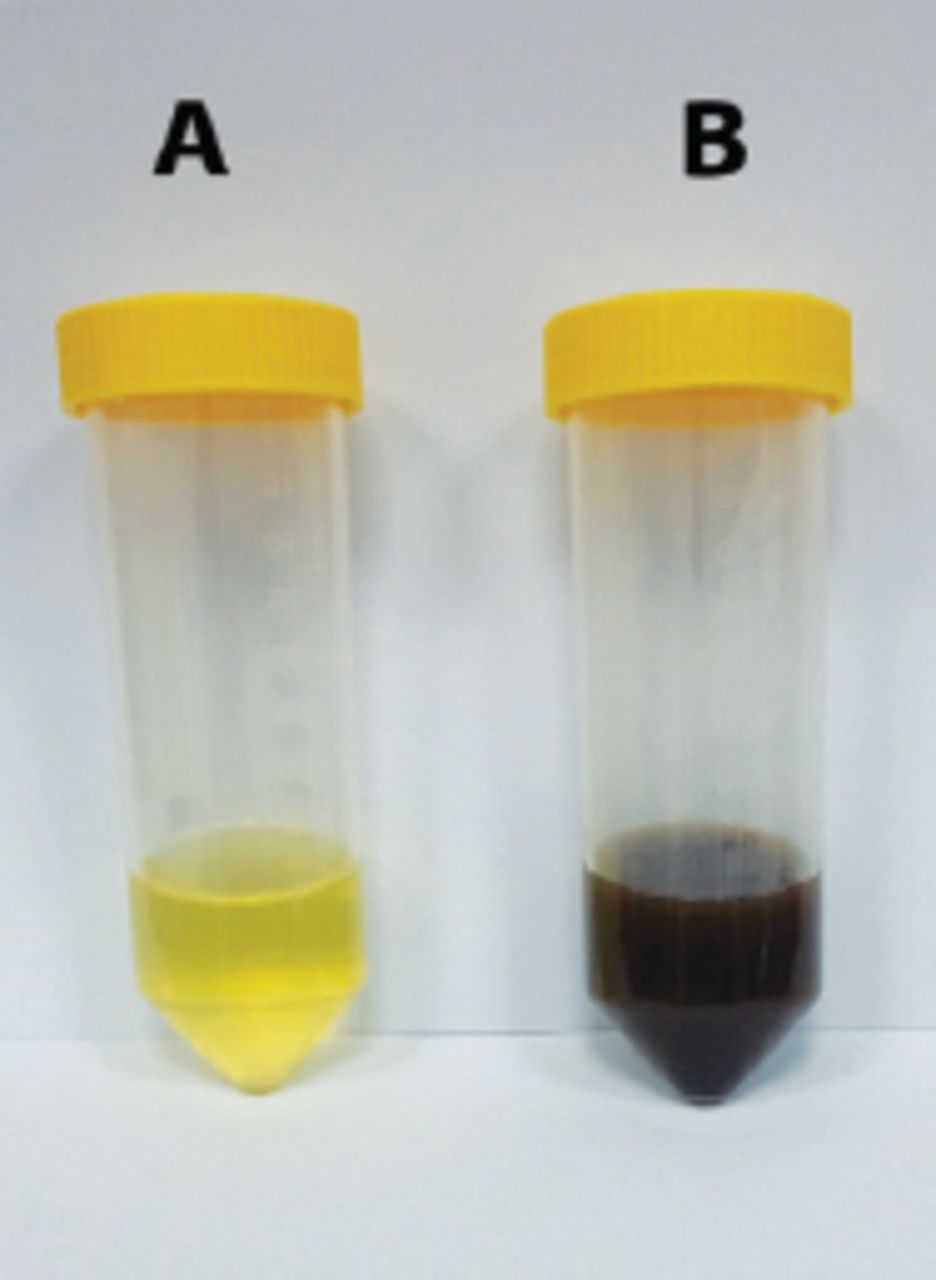
Urine samples from alkaptonuria patient A) fresh sample (left) and B) upon standing for 24 hours (right).
The x-ray of the lumbar spine showed narrowing of disc spaces with calcification and degenerative changes of intervertebral discs (Figure 2). Magnetic resonance imaging demonstrated a complete rupture of the left Achilles tendon, foci of relatively increased signal intensity were observed within the hypointense tendon due to hemorrhage and edema (Figure 3).

Lumbar spine x-ray/lateral view showing significant narrowing of disc spaces at all levels, calcification of disc material at T11-T12 and T12-L1, and diffuse degenerative changes with vacuum phenomenon at L1-L2.

Sagittal T1 fat suppressed A) and T1 TIRM B) MRI sequences showing a complete disruption of Achilles tendon, approximately 2 cm proximal to its insertion with buckling of the proximal part.
Surgical exploration revealed dark pigmentation at the rupture site, which was 4 cm from its bony insertion. The pigmentation was extensive and reaching the calcaneal tuberosity, the frayed ends were pigmented with dark-black color (Figure 4). The gap, as reported by the MRI, was 2 cm and after excision of the frayed ends of the tendon, the gap measured approximately 5 cm. We performed an inverted V-Y technique to restore the length of the tendon and to achieve stable plantar and dorsiflexion of the ankle (Figure 5). He was discharged from the hospital 2 days after surgery with a cast fitted in slight plantarflexion. At 6 weeks follow-up, the cast was removed and he was sent home for gentle ankle motion physiotherapy. He was followed up 12 weeks postoperatively, and presented to the clinic walking without any aid. Physical examination revealed 0-25 of plantarflexion and 0-20 of dorsiflexion. After 6 months, he was able to fully perform his daily activities.

Surgical exploration showing complete left Achilles tendon rupture approximately 4 cm from the calcaneal attachment with dark-black pigmentation of the frayed ends.

Intraoperative test showing A) plantarflexion and B) dorsiflexion of the ankle after repair.
Discussion
Alkaptonuria is an autosomal recessive disorder characterized by darkening of urine, ochronosis (bluish black pigmentation of connective tissue), and arthritis of weight-bearing joints and spine. The hip and knees are most commonly affected. Darkening of urine is often the first clinical sign of the disease, and rarely reported by patients. Patients are usually asymptomatic until the fourth decade of life.4 Complications of AKU involve stones formation (renal, prostatic, and salivary glands) and cardiovascular manifestations (heart valves calcification, aortic stenosis, and coronary artery calcification).2,7 Rupture of muscle, ligaments, and tendons are important features of AKU.4 Deposits of pigmented polymers of HGA in the collagenous tissues affect the structural integrity of collagen.1 This probably increases the possibility of tendon rupture due to their high collagen content. Radiographic and MRI findings in ochronosis have been only extensively studied in spine and other joints. However, there is a limited data on MRI appearance of tendons in ochronosis. Ultrasound examination of Achilles tendon showed loss of fibrillary pattern, increased thickness, small focus of calcification, and increase in size of retrocalcaneal bursa.5 In our patient, we could not identify any peculiar characteristic features of ochronosis by MRI. Large tendons in the body are more frequently affected; rupture of Achilles and patellar tendons has been reported in few case reports in the literature.4,8 Reviewing the international literature, only 11 cases of spontaneous Achilles tendon rupture due to AKU have been reported. Most cases were reported from India.4-6 To the present, no case of similar occurrence has been reported in Middle East.
Although AKU is a rare genetic disease worldwide, our previous studies have shown an increased incidence of AKU in Jordan. Seventy-three cases have been identified so far, two-third of patients were under the age of 25 years, and in many cases more than one patient were affected with AKU in the same family.9 Our patient had a positive family history of AKU. His mother and 8 brothers and sisters have been diagnosed with AKU 6 years ago, and his parents were related prior to their marriage (consanguineous marriage).10 It must be emphasized that the patient developed most of the orthopedic manifestations of the disease much earlier than typical presentations; he developed back pain and arthritis of both hip and knee joints that progressed rapidly after the age of 25. Such early manifestations are rarely reported. He had characteristic radiological changes, particularly of the spine and large joints.
There is no specific treatment for AKU. The only available approach is directed toward symptomatic treatment and timely identification to prompt management of complications. Dietary restriction intake of phenylalanine and tyrosine has been proposed; however, compliance is a problem. Vitamin C is an antioxidant believed to retard the oxidation of HGA. However, the benefits of vitamin C in patients with AKU remain doubtful. Caution must be exercised with supplementation; vitamin C serves as a cofactor for 4-hydroxyphenylpyruvate dioxygenase (HPPD), which causes increased HGA production. The elevated HGA levels could exacerbate the pigmentation process and increase the possibility of developing renal oxalate stones in AKU patients who are already at increased risk for kidney stones.3 A supplementation of vitamin C in doses of 1 g/day represents a rational treatment in older children and adults with AKU. Nitisinone (orfadin) inhibits HPPD, the enzyme that produces HGA. It is used to slow the effects of hereditary tyrosinemia type 1 disease. It has been also shown to reduce urinary HGA excretion by 95% in AKU patients.2 In our patient the tendon healed well after primary repair. It must be emphasized that the above suggested strategies were not followed by our patient. As surgical treatment, repair of ruptured tendons, and joints replacement are required in severe cases, the awareness of AKU patients should be elevated toward the importance of the above suggested strategies and the regular follow up to delay the progression of these complications.
In conclusion, AKU is a rare metabolic disease. Spontaneous Achilles tendon ruptures may occur. Alkaptonuria does not have a specific treatment. A combination of protein restriction diet, vitamin C and nitisinone is suggested to delay the onset and progression of these complications. Therefore, patients of AKU have the responsibility to be aware of their illness and its significant morbidity and potential complications. Avoidance of strenuous exercises and foot straining is the main recommendation especially in patients developing early orthopedic manifestations.
Case Reports
Case reports will only be considered for unusual topics that add something new to the literature. All Case Reports should include at least one figure. Written informed consent for publication must accompany any photograph in which the subject can be identified. Figures should be submitted with a 300 dpi resolution when submitting electronically. The abstract should be unstructured, and the introductory section should always include the objective and reason why the author is presenting this particular case. References should be up to date, preferably not exceeding 15.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received July 13, 2015.
- Accepted August 10, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}