


Abstract
Russell’s viper (RV) envenomation causes local effects, coagulopathy, thrombosis, rhabdomyolysis, acute kidney injury, and neurological manifestations. Although coagulopathy and endothelial destruction causing local and mucosal surface bleeding is known, isolated severe pulmonary hemorrhage is not commonly reported. We report a previously healthy 18-year-old male who had bilateral severe pulmonary hemorrhages, which resulted in a fatal outcome following RV bite. This diagnosis was supported by persistent alveolar shadows, with minimum improvement despite hemodialysis without heparin, mixed acidosis and endotracheal tube bleeding. Other bleeding manifestations were absent. Polyvalent antivenom was administered in lieu of prolonged whole blood clotting time. Thrombocytopenia and mildly deranged clotting parameters were noted. Pulmonary hemorrhages were significant enough to require transfusion. This case highlights the importance of suspecting pulmonary hemorrhages in patients with alveolar shadows and desaturation following RV bite despite the absence of other bleeding manifestations in light of failure of optimum therapy including hemodialysis.
Sri Lanka has one of the highest snakebite rates in the world.1 Although there are around 100 species of snakes found in the country, the highly venomous cobra, Russel’s viper (RV), and kraits contribute to much of the morbidity and approximately 95% of the mortality.1,2 Russell’s viper is one of the most medically important snakes among the tropical countries due to the wide range of clinical manifestations caused by the bites, which include local envenoming, coagulopathy, thrombotic complications, rhabdomyolysis, acute kidney injury, and neurological manifestations.3,4 We describe a case of bilateral pulmonary hemorrhages following an RV bite. Our objective in presenting this particular case is to highlight the importance of suspecting pulmonary hemorrhages in patients with alveolar shadows and desaturation following RV bite despite the absence of other bleeding manifestations in light of failure of optimum therapy including hemodialysis
Case Report
A previously healthy 18-year-old Sri Lankan male from a rural area in the Ratnapura District, Sri Lanka was brought to the medical ward within 2 hours after a snakebite. The dead snake was brought and identified as an RV. He was conscious and rational on examination, and a painful fourth toe of the lower limb demonstrated fang marks. He had features of local envenoming and bedside 20 min whole blood clotting time (WBCT) was found in a non-clotted state indicating evidence of systemic envenoming. He was transferred to a general hospital in the area within the next 2 hours, for administration of Indian polyvalent snake antivenom serum (AVS). His vital parameters were initially normal with pulse of 92/min and blood pressure (BP) of 120/70 mm Hg. The baseline investigations were normal and as follows; hemoglobin (Hb) 12.5 g/dL, white blood cells 6.8 k/uL, neutrophils 50%, lymphocytes 40%, and platelets 160 k/uL. Serum creatinine was 80 umol/L. During the first course of AVS he developed an anaphylactic reaction where his blood pressure dropped to 70/40 mm Hg, which was managed with adrenaline, hydrocortisone, and chlorphenamine. Six hours after the initial dose of AVS still he had prolonged WBCT and AVS was administered twice. Despite vigorous fluid resuscitation, he was oliguric, and with serum creatinine, doubling up to 149 umol/L. On day 3, he was subsequently transferred to the National Hospital for further care. On admission he was dyspneic with a respiratory rate of 28/min, tachycardic (pulse-112/min), and BP was 110/70 mm Hg. There were bilateral basal coarse crepitations more on the left side, but nervous system examination was clinically normal. In the face of deteriorating saturation, he was electively intubated. With oliguria he was found to have a serum creatinine value of 616 umol/L, with severe metabolic and respiratory acidosis in arterial blood gas. Chest x-ray revealed bilateral alveolar shadows (Figure 1). Urgent hemodialysis, without heparin was arranged, which only marginally alleviated the abnormalities. He developed blood stained endotracheal (ET) secretions on the same day and his Hb dropped to 8.3 d/dL, thrombocytopenia (lowest value 84 k/uL). Blood gases showed an increasing trend of CO2 retention, with development of combined respiratory and metabolic acidosis. Despite hemodialysis, respiratory acidosis, pulmonary shadows in the chest x-ray and blood stained ET secretions persisted. He did not have any other systemic bleeding manifestation. A second hemodialysis followed with a blood transfusion, and post dialysis investigation showed an international normalized ratio of 1.6, activated partial thromboplastin time of 34s and thrombocytopenia. He had elevated aspartate aminotransferase (503 IU/L) and alanine transaminase (436 IU/L) with normal bilirubin and alkaline phosphatase. Blood film post hemodialysis showed low-grade micro angiopathic hemolytic anemia (MAHA) although it did not show any fragmented red cells before the dialysis.

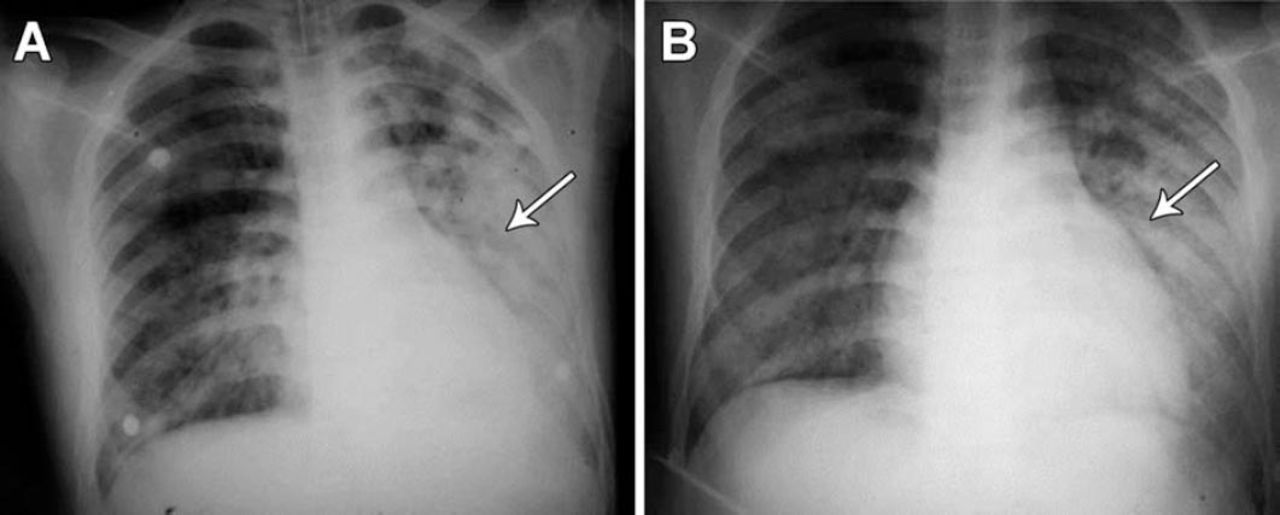
A pre (A) and post (B) hemodialysis chest x-rays showing only a marginal improvement of the alveolar shadowing, which is due to pulmonary hemorrhages (arrows).
On day 4, he was dialyzed once again with fresh frozen plasma 500 ml, and 6 units of platelet rich plasma in view of pulmonary bleeds. But he was persistently oliguric, and his Hb dropped to 8 g/dL with the only bleeding manifestation being blood stained ET secretions. Serum creatinine improved to 617 from 305 umol/L. Despite maximum intervention, hypoxia, acidosis, and hypercarbia continued to manifest. He received the fourth hemodialysis on day 5, which further improved the saturation to approximately 90%, and improvement, albeit slight, in chest x-ray appearance. On day 6, he had a fever, and blood cultures taken revealed a growth of coliforms. Ultrasound scan of the abdomen did not reveal any evidence of intraperitoneal collections. There was no evidence of a pericardial effusion on transthoracic echocardiogram. Computed tomography showed no evidence of intracranial hemorrhage. He was started on antibiotics according to the results of antibiotic sensitivity test. He received one further dialysis, and by this time his liver functions have normalized. On day 9, he developed respiratory arrest and succumbed to death. Table 1 summarizes the laboratory findings.
Summary of the investigation findings, listed chronologically of a patient after an RV bite.
Discussion
Clinical manifestations following RV bite depends on the severity of the envenoming; severe envenoming may lead to pain, swelling, blister formation locally at the site of the bite. Systemic manifestations include coagulopathy, thrombotic complications, rhabdomyolysis, acute kidney injury, and neurological complications.4 Bleeding is a major complication either from the bite site or from mucosal surfaces.5 Hemorrhagins and hemolysins act on the vessel wall causing endothelial destruction together with coagulopathy, and can lead to bleeding, which may be severe enough to require a transfusion as in the case of our patient.5 Early treatment with antivenom is known to control bleeding and clotting disorders, but may not reverse complications like acute renal failure and pulmonary hemorrhages. Reported causes of death include shock, pituitary, and intracranial hemorrhage, massive gastrointestinal hemorrhage, acute tubular necrosis, and bilateral cortical necrosis.4,6,7 Interestingly, pericardial hemorrhage with cardiac tamponade had been reported.2 We could not source any previous reported cases of isolated bilateral pulmonary hemorrhages with fatal outcome following RV bite. However, significant lung injury and hemorrhagic activity has been demonstrated in animal models, especially with regards to factor phospholipase A2.1,8 We came across one case of fatal pulmonary hemorrhage immediately following a bite of Bothrops jararacussu snake, which was proven by autopsy.9 That case was also associated with consumption coagulopathy and disseminated intravascular coagulation.
This case report shows the possibility of fatal outcome due to pulmonary hemorrhages following RV bite. The patient also had acute renal failure, low-grade MAHA and acute respiratory disease syndrome all of which has contributed to the mortality. He did not have any neurological manifestations or thrombotic complications. Despite repeated infusions of AVS, and normalization of WBCT, he continued to have resistant pulmonary hemorrhages. The alternate courses for a pulmonary hemorrhage seem distant too. Hemodialysis was carried out without heparin, and his coagulation parameters were near normal except for thrombocytopenia. We postulate the pulmonary hemorrhages may be due to the snake venom directly damaging alveoli rather than coagulopathy. Micro angiopathic hemolytic anemia is a well-recognized feature of RV bites.6,10 Only minimal improvement of alveolar shadows, even in the face of aggressive hemodialysis, was further suggestive of pulmonary hemorrhages. The opinion of the chest physician and the consultant radiologist was that his clinical picture with alveolar opacities seen, was very much suggestive of pulmonary hemorrhages. We were unable to proceed to necropsy because, on the request of the relatives, we had to release the body after the inquest.
In conclusion, life threatening pulmonary hemorrhage following RV bite is rare. However, small and hence silent, pulmonary hemorrhages may go clinically unnoticed. We emphasize the importance of considering the possibility of pulmonary hemorrhages in hypoxic patients with RV bites, especially if they fail to improve with hemodialysis.
Ethical Consent
All manuscripts reporting the results of experimental investigations involving human subjects should include a statement confirming that informed consent was obtained from each subject or subject’s guardian, after receiving approval of the experimental protocol by a local human ethics committee, or institutional review board. When reporting experiments on animals, authors should indicate whether the institutional and national guide for the care and use of laboratory animals was followed.
Acknowledgment
We acknowledge the patients’ parents for providing written consent for publication of this article. Special thanks goes to Consultant Chest Physician Doctor Keerthi Gunasekara and Consultant Radiologist Doctor Prasad De Silva.
- Received November 2, 2014.
- Accepted February 23, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}