


Abstract
Large bowel obstruction is a rare complication of gastrointestinal endometriosis. A 32-year-old female patient presented to the emergency department with complaints of diffuse abdominal pain and constipation for 10 days with progressive abdominal distention and vomiting. Plain abdominal x-ray showed grossly dilated large bowel up to the sigmoid colon with no gas in the rectum. Abdominal computed tomography revealed hugely dilated large bowel up to the sigmoid colon, with sigmoid soft tissue mass. Flexible sigmoidoscopy showed a non-ulcerating sigmoid mass, with complete obstruction of the sigmoid colon, which impeded the further advancement of the scope. She underwent exploratory laparotomy with provisional diagnosis of complete large bowel obstruction due to sigmoid tumor. Sigmiodectomy with end colostomy was performed. Histopathology revealed endometrial glands with stroma in muscularis properia of the sigmoid colon mass. Endometriosis should be considered in women of reproductive age presenting with symptoms of large bowel obstruction.
Endometriosis is the presence of functional endometrial tissue outside the uterus, which affects up to 15% of childbearing age woman.1 It is an uncommon cause of large bowel obstruction.2 If large bowel obstruction occurs, it may be caused by luminal compression from a pelvic organ endometrioma, a fibrotic reaction resulting in stricture and adhesions, or swelling of endometriotic implants in the intestinal wall or a combination of these 3 mechanisms.3 Herein, a rare case of complete large bowel obstruction due to sigmoid colon endometriotic mass is presented in which the treatment was sigmoidectomy with end colostomy. A brief review of the literature pertaining to this condition is also presented. Our objective in presenting this case is to increase the awareness of physicians to the possibility of endometriosis as a differential diagnosis when assessing females of reproductive age who present with manifestations of intestinal obstruction.
Case Report
A 32-year-old female patient, gravida 4, para 4, presented to the emergency department (ER) with complaints of diffuse abdominal pain and constipation for 10 days with progressive abdominal distention and vomiting. She had no history of per-rectal bleeding, appetite, or weight loss. She had no significant gynecological history (menorrhagia, amenorrhea, dysmenorrhea, irregular menstrual cycle, dyspareunia, and miscarriages). All births were by spontaneous vaginal delivery. She gave a history of change in bowel habits with alternating diarrhea and constipation for the last 9 months, which was unrelated to menstruation. On physical examination, she looked unwell, in pain, and dehydrated, with blood pressure of 105/75 mm Hg, and pulse rate of 92 beats/min. She had a distended, tense, diffusely tender abdomen with no rigidity. Digital and proctoscopic examination revealed empty rectum with no evidence of anorectal pathology. Immediate resuscitation in the ER was started with infusion of crystalloid fluids through 2 large intravenous cannulas with potassium replacement as the patient was having hypokalemia. A nasogastric tube was inserted, which showed clear gastric fluids, and an insertion of foley’s catheter was performed with drainage of a small amount of concentrated urine. A sample of blood was extracted and sent for complete blood count, coagulation profile, electrolytes, creatinine, and urea. She then underwent plain abdominal x-ray, which showed grossly dilated large bowel up to the sigmoid colon with no gas in the rectum (Figure 1). Abdominal CT revealed hugely dilated large bowel up to the sigmoid colon, where there was a soft tissue mass measuring 6.5 × 4 cm (Figure 2). Flexible sigmoidoscopy showed non-ulcerating sigmoid mass, with complete obstruction of the sigmoid colon, which impeded the further advancement of the scope. She underwent exploratory laparotomy with provisional diagnosis of large bowel obstruction due to sigmoid tumor. Abdominal exploration revealed obstructing sigmoid mass with no evidence of abdominal metastasis and multiple cystic lesions, which contained chocolate like fluid in the Douglas pouch. Sigmiodectomy with left iliac fossa end colostomy (Hartmann’s procedure) was performed with an uneventful postoperative recovery. Histopathology of the sigmoid mass revealed the presence of endometrial glands with stroma in muscularis properia of the sigmoid colon mass (Figure 3). On the ninth postoperative day, she was discharged on danazol, which was changed to Gonadotropin-releasing hormone agonists (Goserelin) during the follow up in the outpatient clinic. She was followed up in the surgical and gynecology outpatient clinic. She underwent closure of colostomy 3 months after the index surgery.

Grossly distended large bowel up to the sigmoid colon with no gas in the rectum (arrows).
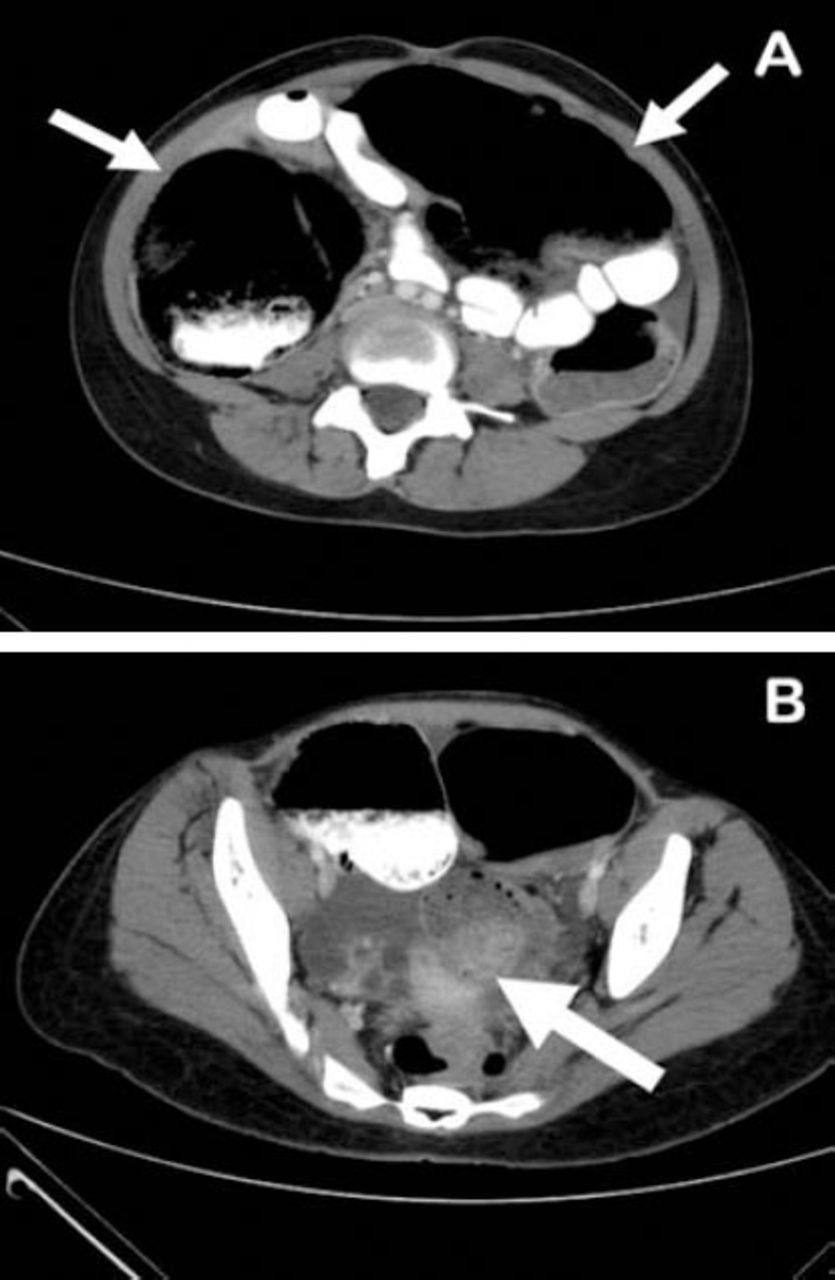
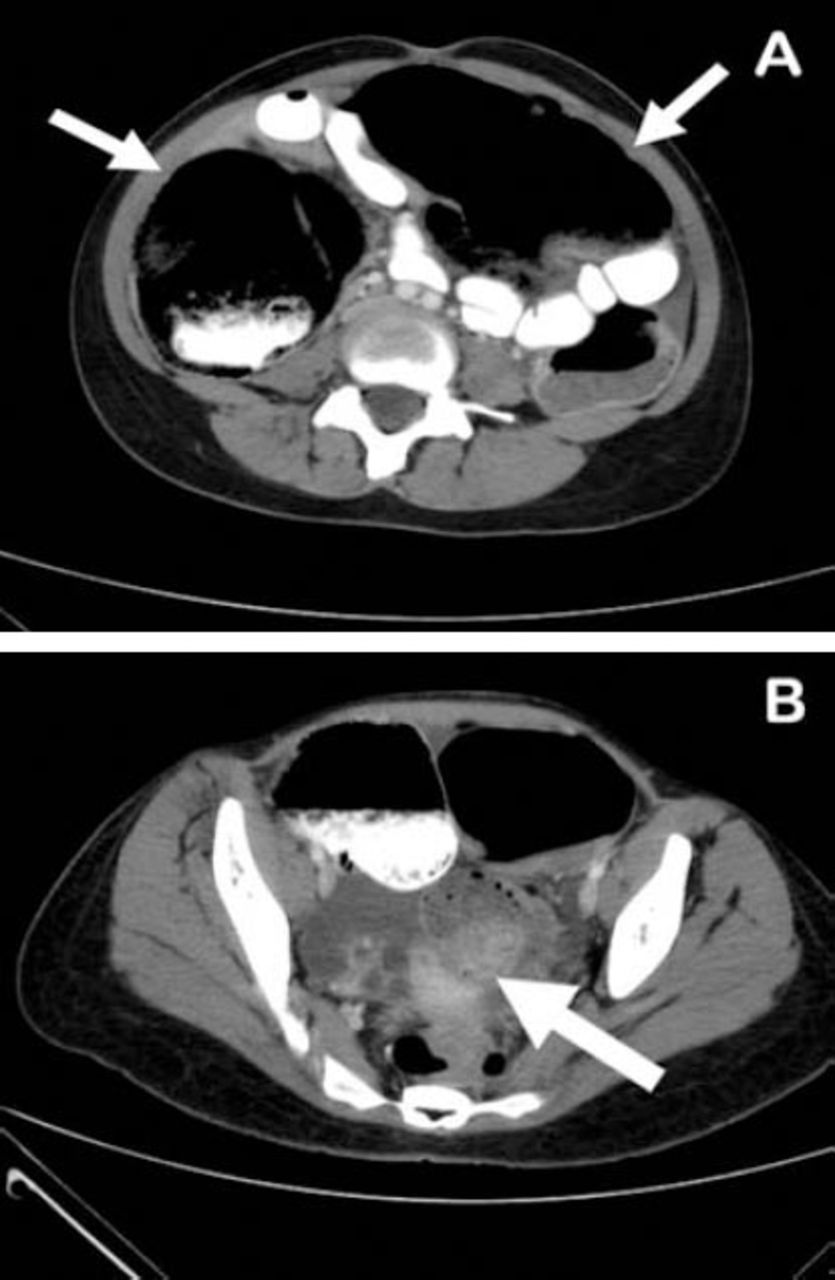
Abdominal computed tomography showing A) hugely distended large bowel (arrows). B) Soft tissue mass in the sigmoid colon (arrow).
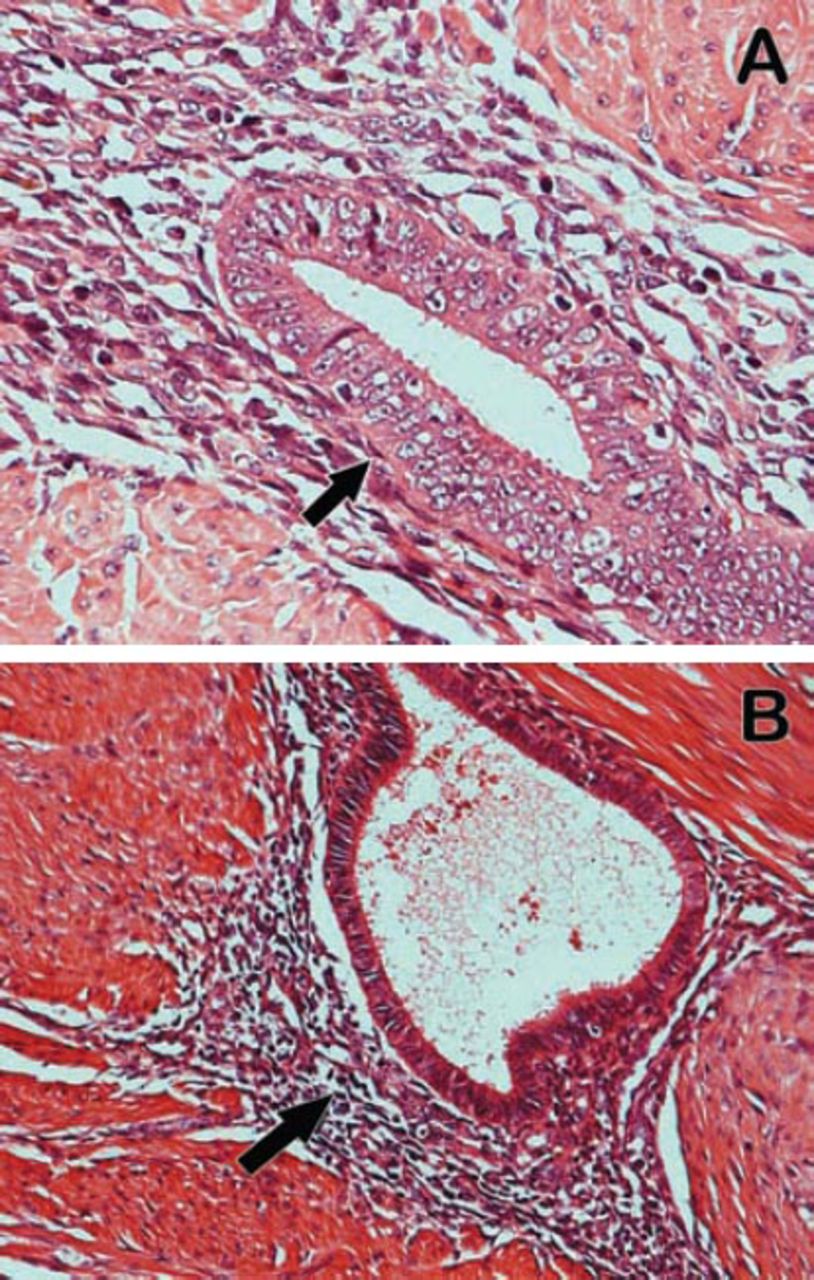
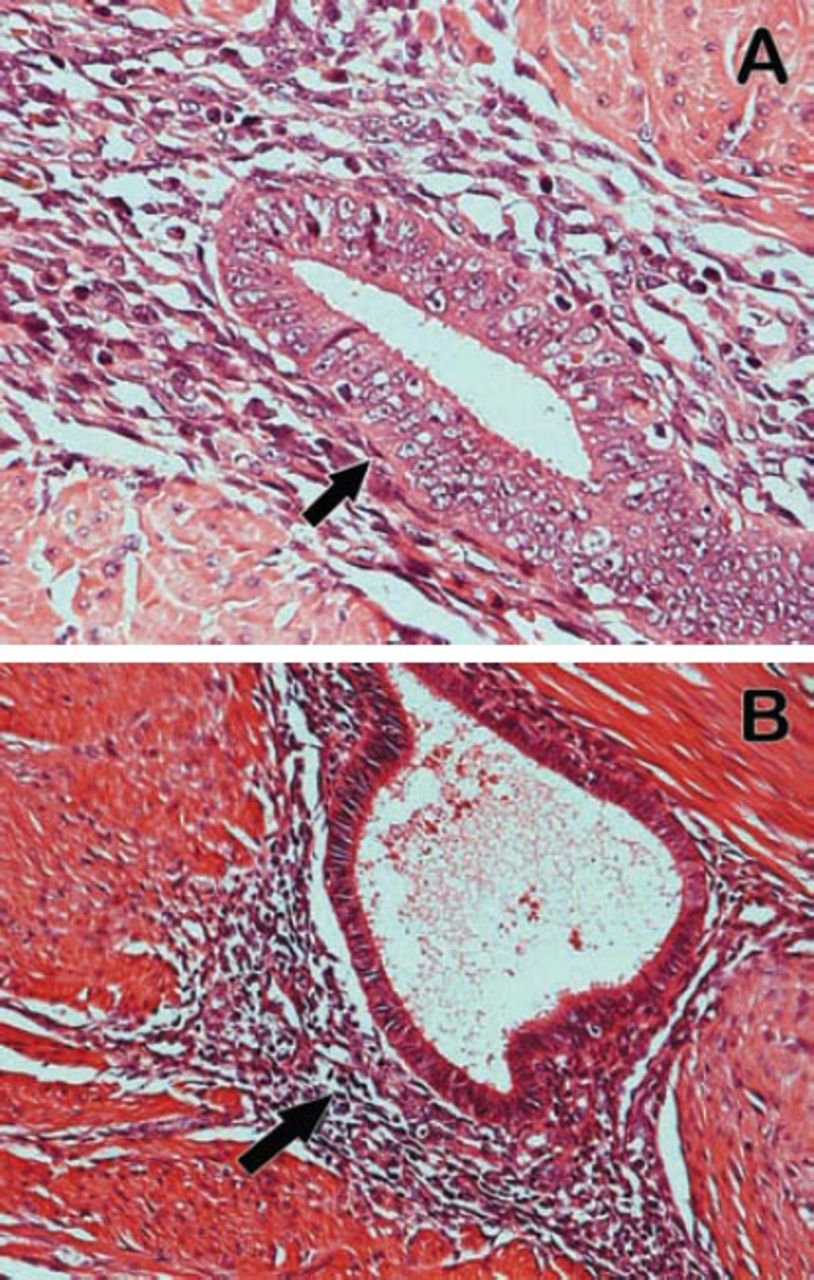
High power microscopic view of A) intramuscular endometriosis within the B) bowel wall. Note the presence of both endometrial glands and stroma (hematoxylin and eosin stain ×400).
Discussion
Endometriosis is a common disease that can be intra or extraperitoneal, depending on the location of the metastatic endometrial tissues.4 Intraperitoneal disease is mainly genital or pelvic, with the ovaries, fallopian tubes, uterine ligaments, pelvic peritoneum, and Douglas pouch, as the most commonly involved sites.1,5 The gastrointestinal tract (GIT), is the most common site of extra-genital endometriosis; however, other intra-abdominal organs can occasionally be involved. Extraperitoneal endometriosis is uncommon, and it may involve the vagina, cervix, abdominal scars, and sacs of hernias. The GIT is affected in 3-37% of women with endometriosis. Although the rectosigmoid colon is the most commonly involved, it can affect any part of the GIT.6 In the present case, it involved the sigmoid colon as an obstructing mass with multiple cystic lesions containing chocolate like fluid in the Douglas pouch. On English literature review, only 11 reported cases of sigmoid colon endometriosis causing large bowel obstruction were found. Bowel endometriosis begins by implantation on the serosa followed by invasion of the muscularis properia, but the mucosa is rarely involved.1,6 In this case, flexible sigmoidoscopy revealed an obstructing mass in the sigmoid colon with non-ulcerating mucosa. The clinical features of bowel endometriosis vary depending on the extent and site of involvement, and it can be difficult to distinguish endometriosis of the GIT from other gastrointestinal pathology due to the lack of pathognomonic clinical features of the disease.1,2,4,6,7 Large endometriotic lesions may cause thickening and fibrosis of the wall of the bowel resulting in stricture formation and mechanical bowel obstruction. It can also cause infiltration and damage to the nervous plexus or the interstitial Cajal cells as well as intestinal sympathetic nerve fibers attrition.6 Endometriosis of the GIT can be asymptomatic, but most patients presents with symptoms that are usually cyclical and occurring at the time of menstruation. These symptoms include nausea, bloating, diarrhea, constipation, painful defecation, tenesmus, rectal bleeding, bowel perforation, lower abdominal, and pelvic pain.1,4,6-8 Our patient complained of non-cyclical alternating diarrhea and constipation for 9 months, which resulted in the clinical features of complete large bowel obstruction. The diagnosis of large bowel endometriosis remains difficult to be established preoperatively; however, it can be suspected on the basis of the cyclical clinical history.1-7 A variety of investigative tools has been used, which include barium enema, colonoscopy, CT and MRI, transrectal, and transvaginal ultrasound with variable results.1,4,6 Currently, MRI is considered as the best imaging tool for detection and evaluation of intestinal endometriosis.3 Laparoscopic evaluation along with lesion excision for histological examination remains the gold standard for the diagnosis.1,6 In the present case, CT scan was carried out, which did not help in the differential diagnosis of the sigmoid colon mass, and the laparoscopy was not an option in the presence of grossly distended large bowel.
Treatment of large bowel endometriosis depends on the severity of the disease.1,8 Medical treatment in the form of danazol, gonadotrophin-releasing hormone analogues, or progestins are indicated when the disease is detected before there are complications.6,9 Surgical treatment in the form of laparoscopic or open surgery is indicated when the patient presents with changes in bowel habits, bleeding, intestinal obstruction, and when the malignant tumor cannot be ruled out.6,7,9 Recently, the laparoscopic approach has been evaluated, with significant postoperative improvement of digestive and gynecological symptoms as well as quality of life, and should be the first surgical approach.10 In this patient who was presented with complete large bowel obstruction, the treatment was open surgical intervention, resection of the sigmoid colon with the sigmoid mass, and end colostomy. The laparoscopic approach was not chosen due to the massive distension of the abdomen. The final histopathology of the sigmoid mass revealed intramuscular endometriosis within the bowel wall.
In conclusion, sigmoid colon endometriosis can form a mass, leading to complete large bowel obstruction. Despite the low frequency of sigmoid colon endometriotic mass as an underlying cause of complete large bowel obstruction, it should be considered in the deferential diagnosis in women of reproductive age presenting with any symptoms of large bowel obstruction.
Copyright
Whenever a manuscript contains material (tables, figures, etc.) which is protected by copyright (previously published), it is the obligation of the author to obtain written permission from the holder of the copyright (usually the publisher) to reproduce the material in Saudi Medical Journal. This also applies if the material is the authors own work. Please submit copies of the material from the source in which it was first published.
Acknowledgment
We would like to thank Dr. Rumian Alrumian, Consultant Radiologist, for his help in reporting of imaging. We are also grateful to Dr. Mohammed Al-Aiyaf, Consultant Pathologist, for providing the photomicrographs for the patient.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received January 18, 2015.
- Accepted March 16, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.