


Abstract
Objectives: To assess the association between body mass index (BMI) and hemoglobin A1c (HbA1c) with serum prostate-specific antigen (PSA) level.
Methods: A retrospective cohort study was carried out at King Faisal Specialist Hospital and Research Centre in Riyadh, Saudi Arabia, from January 2016 to December 2021. Data were collected from the medical records of patients who visited the family medicine clinics, including demographics, smoking status, BMI value, index PSA level, testosterone level, digital rectal exam findings, prostate biopsy status, fasting blood glucose (FBG), HbA1c, diabetes duration, chronic comorbidities (namely, hypertension, dyslipidemia, or chronic kidney disease), and medication history.
Results: The mean PSA level was 1.89±4.02 ng/dL and mean HbA1c was 6.59±2.69%. Of the participants, 41.8% were overweight, 54.3% were non-diabetics, and 85.3% were nonsmokers. Only 11 (1.6%) participants had undergone a prostate biopsy after taking a PSA test. There was a positive correlation between PSA level and age, a negative correlation between PSA level and BMI, and no correlation between PSA level and HbA1c or FBG.
Conclusion: Prostate-specific antigen levels were higher in older people and those with low BMIs. No correlations were found between PSA levels and HbA1c or FBG, even after adjusting for other variables. Moreover, no correlations were found between PSA levels and other comorbidities such as dyslipidemia, chronic kidney disease, and hypertension.
Prostate-specific antigen (PSA) level is usually initially used for prostate cancer screening.1 According to the American Urology Association and the European Association of Urology, a prostate biopsy is warranted when PSA levels exceed 3-4 ng/dL.2,3 However, multiple factors, including age, catheterization, medications, acute prostatitis, and other comorbidities, affect PSA levels, limiting the validity of the test.4 Particular attention has been paid to the effect of obesity and diabetes on PSA level.
The relationship between obesity and PSA level remains controversial. Obese men have a larger plasma volume which might decrease serum concentration of the soluble tumor marker.5 Chia et al,6 Price et al,7 and Kubota et al8 found an inverse relationship between body mass index (BMI) and PSA. On the other hand, several studies showed no statically significant association between PSA and BMI.9-11
A systematic review with compelling evidence concluded that there is an inverse relationship between diabetes and prostate cancer.12 Another meta-analysis found that this inverse association was believed unlikely to affect prostate cancer screening.13 On the other hand, several studies have observed that diabetes increases the risk of more aggressive prostate cancer. An Asian meta-analysis found that having diabetes increases the incidence and risk of death from prostate cancer.14
Overall, the literature offers inconsistent findings on the relationship between PSA level and BMI or hemoglobin A1c (HbA1c). There have also been few local studies on this topic. Therefore, in a primary care setting at the family medicine clinic at King Faisal Specialist Hospital and Research Centre in Riyadh, Saudi Arabia, this study aimed to assess the association between BMI and HbA1c with serum PSA level.
Methods
A retrospective cohort study was carried out at King Faisal Specialist Hospital and Research Centre in Riyadh, Saudi Arabia, from January 2016 to December 2021. All adult patients aged 40 years and older who visited the family medicine clinic for PSA screening for prostate cancer were included in the study. Patients who had conditions that might affect PSA levels, such as cirrhotic liver disease or acute prostatitis, or who had already been diagnosed with prostate cancer were excluded from the study.
Data recorded included demographic information (namely, age and nationality), BMI value, index PSA level (the first PSA reading), testosterone level, digital rectal exam findings, prostate biopsy status, fasting blood glucose (FBG), HbA1c, diabetes duration, and chronic comorbidities (namely, hypertension, dyslipidemia, and chronic kidney disease). Prostate-specific antigen levels of >4 ng/dL were considered abnormal. The American Diabetes Association’s guidelines were used to determine the presence of prediabetes and diabetes.15 Fasting blood glucose and HbA1c results were included if they had been obtained within 3 months before or after the index PSA. If no data were available within 3 months, the reading obtained closest to the index PSA was used. Hypertension and dyslipidemia were defined according to the American Heart Association’s guidelines and based on whether a patient was taking antihypertensive drugs or statins.16,17
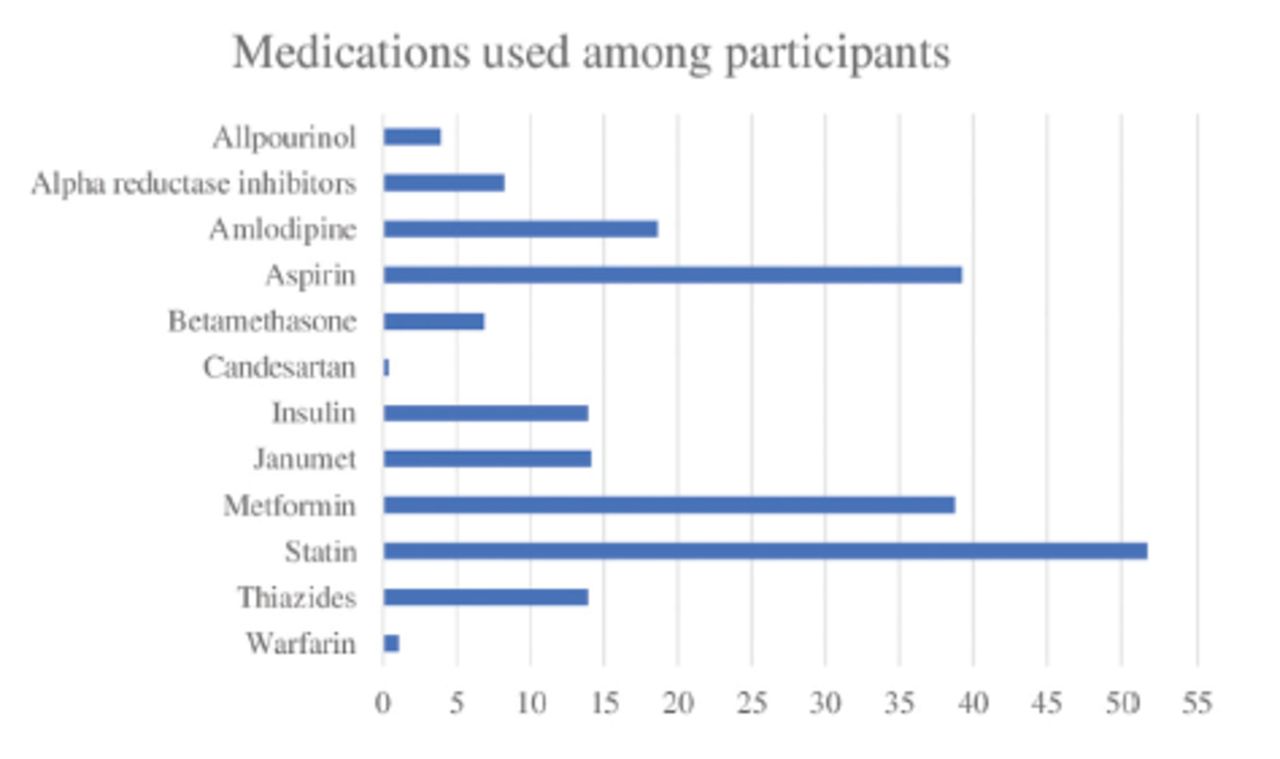
Medications likely to interact with the interpretation of PSA levels, including insulin, metformin, amlodipine, aspirin, warfarin, allopurinol, betamethasone, candesartan, statins, and diuretics, were collected to account for confounding factors.18,19
Data were collected anonymously. Serial numbers and coding were utilized to ensure privacy and confidentiality. Ethical approval was received, and a waiver of informed consent was obtained from the Research Ethics Committee at King Faisal Specialist Hospital and Research Center, Riyadh, Saudi Arabia (RAC# 2221030).
Statistical analysis
Data was analyzed using the Statistical Package for the Social Sciences, version 20.0 (IBM Corp., Armonk, NY, USA). In descriptive statistics, percentages (%) and frequencies (n) were used to summarize categorical variables, and the mean ± standard deviation (SD) was reported for continuous variables. The difference in the distribution between the categorical variables was tested through Chi-square tests. For analyzing the continuous variables, an independent T-test and ANOVA were used, as the main outcome of the study (PSA) was normally distributed. Pearson’s correlation was used to test for collinearity between continuous variables. Linear regression was carried out to assess the role of different variables on PSA level. All statistical analyses were carried out at a p-value of 0.05 with a 95% confidence interval (CI).
Results
A total of 750 participants underwent both PSA and HbA1c tests and were included in this study. Their mean age was 61.36±10.82 years, and the majority of the participants (32.7%) were aged 50-59. The mean PSA level of the participants was 1.88±3.88 ng/dL, and the mean HbA1c (within 6 months of the PSA reading) was 6.58±2.60%. Additionally, 69.2% of the participants were Saudi, 41.6% were overweight, and 83.0% were nonsmokers. Only 11 (1.6%) participants underwent a prostate biopsy after PSA testing. Additional descriptive statistics regarding the study sample are reported in Table 1. Medications used among the participants are shown in Figure 1.

- Frequency of medications used among participants.
- General characteristics of participants (N=750).
No correlation was found between PSA level and HbA1c or FBG, as shown in Table 2. However, the analysis showed that mean PSA levels were significantly higher among patients who were aged 80 years and older (3.41±4.67 ng/dL) or underweight (9.74±27.23 ng/dL; p<0.05). The mean PSA level did not differ significantly among relevant comorbidities (Table 3) or medications used (p>0.05). Linear regression results were not reported because no significant association was found between PSA level and HbA1c, even after adjusting for all included variables.
- Mean prostate-specific antigen levels among different subgroups.
- Correlation between prostate-specific antigen level, hemoglobin A1c, and fasting blood glucose.
Discussion
In this study, the association between BMI, HbA1c, and PSA level, was investigated. Prostate-specific antigen level is correlated with age and as age increases, PSA level also becomes higher.20 This relationship can be explained by the fact that there is age related increase in the prevalence of benign prostatic enlargement.21 Our study found that the mean PSA level increased with age (3.41±4.67 ng/dL), especially in those aged 80 years and older. Obesity increases intravascular volume, which dilutes the amount of PSA in the body. However, it is not clear whether this effect should be adjusted when determining PSA level.22 We found that those with a lower BMI had a higher mean PSA level (9.74±27.23 ng/dL; p<0.05). This finding is in line with that of another study, BMI was found to be inversely associated with PSA level; that is, participants whose BMI was >27 had lower PSA levels than those whose BMI was <27.23
Prostate epithelial cells produce PSA in response to androgens which play an important role in prostate tumorigenesis. Diabetic men tend to have low androgens concentration.24 Our study revealed no correlation or significant association between HbA1c, FBG, and PSA level, even after adjusting for other variables. Similarly, a Moroccan study found that PSA levels were similar between diabetics and non-diabetics.25 However, a study carried out in Japan found that PSA levels were lower among diabetics after adjusting for the ages of the study’s participants.26 Similarly, another study carried out in Germany found that PSA levels were lower in those with high HbA1c results.27 This positive correlation might be explained by the fact that the prevalence of diabetes among the participants was low unlike our study in which the diabetic subjects were 46.7%.28,29
This study found that PSA level is not correlated with other comorbidities (namely, dyslipidemia, chronic kidney disease, and hypertension). A study carried out in the United States of America found that serum triglycerides are negatively correlated with serum PSA levels in those diagnosed with prostate cancer.30 Another prior study showed that patients with chronic kidney disease had higher PSA levels than those in the control group.31 Like our study, one study found that hypertension was not correlated with PSA.26 As presented in Figure 1, we found that the medication used by the participants was not correlated with PSA levels. However, Müller et al27 found that PSA levels were lower in those using oral antidiabetic medications and insulin. Another study concluded that, although statins are associated with lower PSA levels, their presence should not affect screening interpretation.32 Similarly, Chang et al19 found that both statins and thiazide diuretics lower PSA level. Finally, a prospective study found that aspirin use is associated with lower PSA levels and cancer risk.33
Study strengths & limitations
A key strength of this study is that it is a population-based study. In addition, only few local studies have examined the association between PSA level, HbA1c, or BMI. Moreover, most of the potential confounding factors that might have an impact on PSA levels such as other chronic medical conditions and medications were addressed. On the other hand, those subjects who might have early prostate cancer but were missed due to low serum PSA level were not fully excluded through prostate biopsy which could be a limitation in our study. Another potential limitation is the lack of precise data regarding diabetes such as diabetes duration, treatment duration, and level of adherence and control, which might also affect PSA values.
In conclusion, PSA levels were higher in older people and those with low BMIs. Modified PSA thresholds for obese men and considering BMI readings while interpreting age-specific PSA levels is therefore recommended. No correlations were found between PSA levels and HbA1c or FBG, even after adjusting for other variables. Future local studies with a larger sample size and detailed information on diabetes duration and management is recommended. Moreover, no correlations were found between PSA levels and other comorbidities such as dyslipidemia, chronic kidney disease, and hypertension.
Acknowledgment
The authors gratefully acknowledge Scribendi (www.scribendi.com) for their English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 24, 2023.
- Accepted August 1, 2023.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.