


Abstract
Objectives: To investigate whether magnetic resonance imaging (MRI) best detects early malignancy in high-risk women.
Methods: A retrospective, cross-sectional study, carried out at King Abdulaziz University Hospital, Jeddah, Saudi Arabia, included 419 female breast cancer patients aged 16-84 years (mean age of 49). Data were collected from the radiological department’s database to compare the MRI, ultrasound (US), and mammography results, with or without tissue biopsy.
Results: In diagnosing benign versus malignant lesions, MRI showed significant agreement with tissue biopsy, with high sensitivity (70%) and specificity (87%); its positive predictive value (PPV) was 92% and negative predictive value (NPV) was 56%. While US has a PPV of 84% and NPV of 63%; with a sensitivity (79%) and specificity (71%). In patients without tissue biopsy, there was little difference between mammography and US compared with MRI results.
Conclusion: Magnetic resonance imaging is more effective than US and mammography for early detection of BC. It showed high sensitivity in detecting breast lesions and high specificity in characterizing their nature when correlated with pathological results. Ultrasound screening followed by MRI is suggested for undetected or suspected lesions. This will increase the breast lesion detection rate, reduce unneeded tissue biopsies, and enhance the disease’s survival rate.
Breast cancer (BC) is a perilous and well-known cancer among women. The uncontrolled changes or growth of the breast tissue cells create a mass (tumor). It can spread (metastasize) across the breast to lymph nodes (LN) or other body parts.1 In women, BC symptoms include breast lumps, size changes, pain, and nipple fluid discharge, whereas, in men, the hard painless breast lump is the most common sign.2 Women’s BC is affecting approximately 2 million women in 2020, associated with considerable health morbidity and mortality.3
In Saudi Arabia, BC mortality is highly prevalent among women, and even though morbidity in men is lower than in women, the mortality risk is higher in men. Moreover, the socioeconomic and health-related status and menstruation history variables are considered risk factors for BC in Saudi Arabia. Furthermore, education, financial state, sedentary lifestyle, smoking, cancer knowledge, contraceptive intake, and precocious puberty must be added to culturally reasonable prevention programs.4 However, more than 50% of BC cases are discovered in Saudi Arabia at an advanced stage versus 20% in more developed countries. Early recognition is crucial for curing the illness, increasing the possibility of treatment to over 95% and decreasing the mortality rate by 30%.5 Fortunately, there have been remarkable advancements in diagnostic imaging for BC in recent years, with mammography being the most widely used diagnostic test worldwide. However, its clinical use only emerged in the early 20th century, leading to diagnostic delays and unfavorable short-term prognoses. Organized mammography screening has significantly reduced mortality rates by enabling early BC detection.6
Many countries have adopted targeted mammography screening programs, effectively lowering cancer-related mortality rates. However, BC burden varies significantly across different human development indices (HDIs), with a higher incidence in HDI-higher countries compared to HDI-intermediate or HDI-lower countries.7 The screening of BC is broadly recognized for decreasing BC mortality, and the screening’s primary purpose is to diagnose the disease early-stage of asymptomatic patients to enhance treatment efficacy. Even though the compromise regarding the screening advantages, disagreement persists as regards the ideal screening frequency and age to begin and end screening.8
Breast magnetic resonance imaging (MRI) techniques hold promise as a supplementary method to mammography for BC identification and diagnosis, as they offer overall faster examination times.9 Breast MRI has extended indications as preoperative staging, where several studies show its effectiveness in estimating tumor size and detecting foci of tumors in ipsilateral and contralateral breasts compared to other imaging modalities.10 Furthermore, in the early stage, MRI can detect minor tumors at greater resolution.11
Numerous studies have demonstrated the superiority of MRI over other imaging modalities. Also, according to Bakker et al12 mammography has a restriction in identifying cancer in highly dense breast tissue; using a supplemental MRI screening proved to have superior value over normal results mammography. In addition, MRI is necessary to determine tumor growth and verify the need for biopsy, with a sensitivity of 94-100% and the capability to illustrate minor invasive cancers up to 5 mm that occasionally fail to be detected by mammographic screening.13,14 In 2014, Kuhl et al15 pioneered the condensed breast MRI protocol for BC screening, involving a single maximum intensity projection picture, a single contrast-enhanced T1-weighted sequence, and 2 unenhanced T1-weighted sequences. In women with high-risk and possibly average-risk BC development, contrast-enhanced MRI for BC outperforms non-contrast-based options such as mammography and ultrasound (US). Mammography supplemental utilization can improve cancer recognition on breast MRI only but lowers specificity. While supplementary utilization of the US only reduces specificity and should be prevented. In women who participated in the initial MRI screening studies with MRI, the earlier finding of cancers seems to interpret survival profits, which is entirely in line with the BC screening hypothesis and will likely be viewed accurately for all indications. Magnetic resonance imaging has a greater sensitivity for all forms of BC, such as low-grade ductal carcinoma in situ (DCIS), which may raise overdiagnosis.10,15 In our study, we assessed the indications of MRI as a screening test for BC, including high-risk women. Therefore, this study aimed to investigate whether MRI delivers the best detection of early malignancy among high-risk women.
Methods
This study was a retrospective, cross-sectional study carried out at King Abdulaziz University Hospital in Jeddah, Saudi Arabia. The research ethical committee at the Faculty of Applied Medical Sciences approved this study. Data were collected from patients who underwent an MRI between January 2021 and December 2022. All selected data were from female BC patients.
The study included 419 women aged between 16-84 (mean age 49). The data obtained from the radiological department of King Abdulaziz University Hospital in Jeddah, included MRI, US, mammography, and histopathology results, and Excel sheets were used to record patient histories. A secure hard drive was used to store patient data without disclosing personal information or names to maintain patient privacy. All our data were extracted from the PACS system of King Abdulaziz University Hospital. The radiologists who wrote MRI, US, and mammography reports have subspecialty training or fellowship experience in breast imaging with extensive training and expertise in addition to advancing medical knowledge. They have professional standards to provide unbiased and accurate interpretations. They often participate in peer review processes, both as authors and reviewers, to maintain the integrity and accuracy of published research.
Breast MRI investigations were carried out with the Magnetom Skyra, a 3T MRI system. The breast coils produce a total of 18 channels; 4 frontal elements, 4 elements around the breast, and one axillary element create 9 elements for each breast. Additionally, the unit includes an MR injection system.
Criteria for inclusion in the study were high-risk, young, asymptomatic female patients with a strong family history of breast, ovarian, or prostate cancer or any cancer related to the BRCA1 and BRCA2 genes who visited the clinic for a physical examination of the breast, with subsequent MRI screening requested. Other high-risk conditions included augmentation implants, previous history of BC post-chemotherapy, post-excisional biopsy, and BC mastectomy.
The study also included symptomatic patients with a palpable or suspicious mass; abnormal nipple discharge, especially mucinous (clear and watery), sanguineous (bloody), or serosanguineous (pink); or abnormal axillary LN who were recommended for breast MRI.
Further, any mammogram or US screening results that showed a suspicious mass or findings, especially in patients with high-risk factors, were also included.
After data collection, we discussed agreement with the gold standard, which was histopathology findings in tissue biopsy cases, and the results of MRI, US, and mammography were compared with those of tissue biopsy. In patients who received mammography, US, and MRI only without tissue biopsy, we considered MRI the gold standard, which we compared to the US and mammography findings.
We thoroughly reviewed all reports throughout the data collection process to determine which patients were eligible for our research. We carried out additional revisions on reports written by the MRI breast radiologists and consulted with them for any missed reports, including mammograms, US, MRI, and biopsy reports, as we carried out a correlation analysis.
Statistical analysis
Data from patients were collected in a Microsoft Office 2020© Excel sheet and then exported to the Statistical Package for the Social Sciences Statistics for Windows, version 27.0 (IBM Corp., Armonk, NY, USA). Categorical variables were presented as numbers and percentages (%). The Chi-square test was used to assess the agreement with the gold standard results. A p-value of <0.05 was considered significant to assess the association between rows and columns. The kappa value was calculated to assess the agreement between the 2 procedures. In addition, this study used the Chi-square test to evaluate the relationship between age groups and histopathology results.
Results
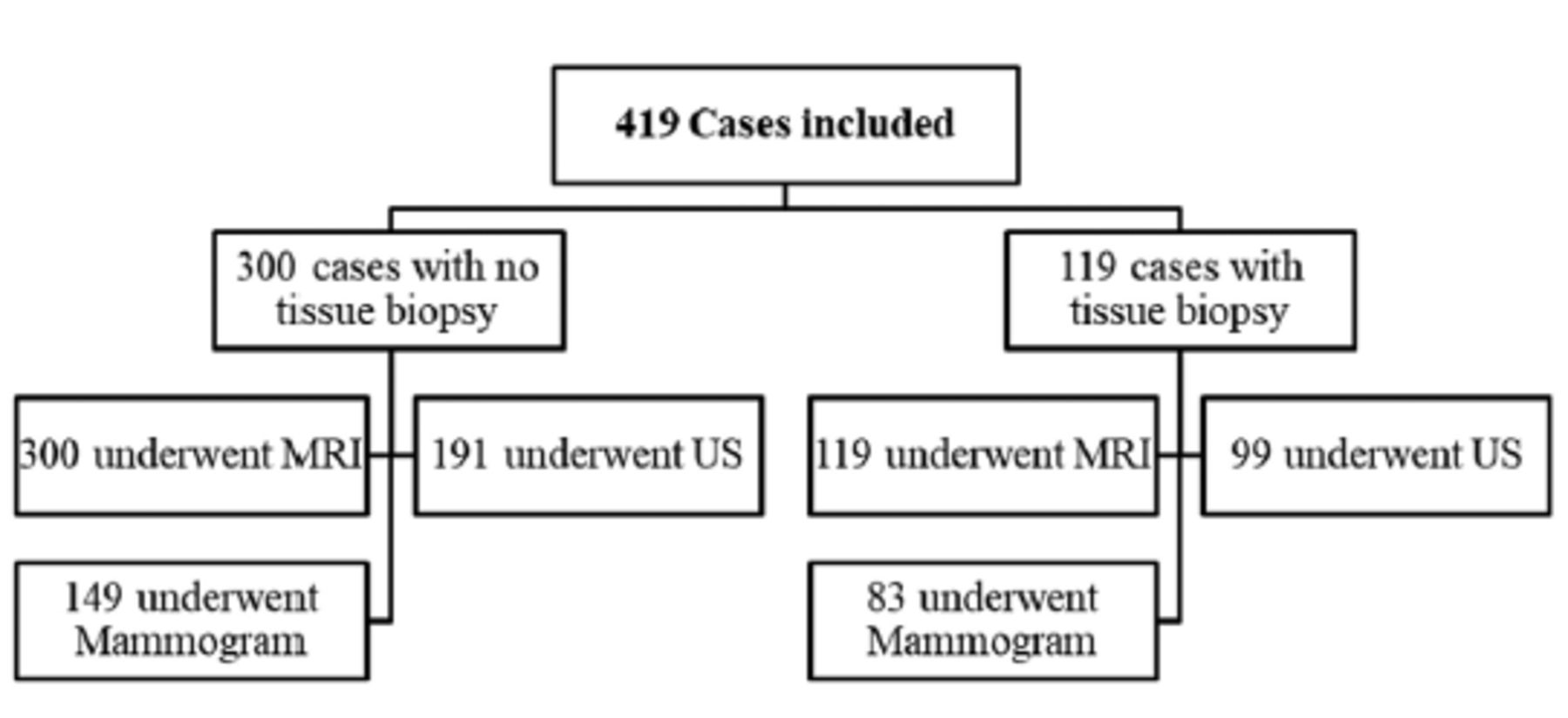
This study included 419 female subjects who underwent an examination for BC including multiple procedures. Patients were divided into 2 groups based on undergoing tissue biopsies. The first group constituted female patients (n=119) who underwent tissue biopsy (the gold standard for suspected lesions in this group) as well as other procedures, as indicated by the algorithm below in Figure 1. In the second group (n=300), patients were not subjected to tissue biopsy. However, they underwent MRI (n=300) together with US (n=191) or mammography (n=149). In this group, MRI was considered the gold standard.

- Algorithm showing the procedures carried out in all studied patients. MRI: magnetic resonance imaging, US: ultrasound
In the group of patients who underwent tissue biopsy as the gold standard, the incidence of BC was 69%. After obtaining the results of other procedures (mammography, MRI, or US), we compared the results of each procedure with the results of the tissue biopsy. A comparison of the tissue biopsy results with the mammogram results as shown in Table 1 revealed no significant agreement between the 2 procedures, as shown by a kappa value of 0.16 and a p-value of 0.14. The initial mammogram indicated 25 cases of benign tumors, but after histopathology results were available, only 11 were deemed benign and 14 were malignant. Additionally, the initial mammogram showed 58 cases of malignant tumors, but after histopathology results were available, 16 were considered benign and 42 malignant. The diagnostic analysis of mammography is illustrated in Figure 2a.
- Mammogram, magnetic resonance imaging, and ultrasound results compared with tissue biopsy results.

- Comparisons of the tissue biopsy results. a) Diagnostic performance of mammogram vs tissue biopsy. b) Diagnostic performance of magnetic resonance imaging vs tissue biopsy. c) Diagnostic performance of ultrasound vs tissue biopsy. Mammo: mammogram, PPV: positive predictive value, NPV: negative predictive value, MRI: magnetic resonance imaging, US: ultrasound
Table 1 also displays the comparison between MRI and tissue biopsy results, revealing significant agreement. The kappa value for agreement is 0.49, with a significant p-value of <0.01. With MRI, 57 cases were classified as benign. However, after analysis of the histopathology results, 32 were confirmed as benign and 25 were diagnosed as malignant. On the other hand, 62 MRI results were identified as malignant. After analysis of the histopathology results, it was determined that 5 were benign and 57 were malignant. The diagnostic performance of MRI versus tissue biopsy is depicted in Figure 2b.
The results of the US and tissue biopsy procedures were compared and found to have a notable level of agreement, as indicated in Table 1. The agreement was determined to have a kappa value of 0.48 and a significance of p<0.01. Specifically, US showed 38 cases as benign, but further examination through histopathology revealed that 24 were indeed benign and 14 were malignant. On the other hand, US identified 61 cases as malignant, but after histopathology results were available, it was determined that 10 were benign and 51 were malignant. Similarly, the diagnostic performance of US versus tissue biopsy is shown in Figure 2c.
Assuming tissue biopsy as the gold standard, we compared the results of the 3 procedures with those of tissue biopsy. A 79% sensitivity for US and an 87% specificity for MRI were found. In terms of predictive value, MRI had a 92% PPV, while US had a 63% NPV. In terms of overall accuracy, US (76%) and MRI (75%) had similar results, while mammography had 64%. The kappa for agreement was significant for both MRI and US, indicating strong agreement between the tests. However, it was non-significant for mammography.
In the absence of tissue biopsy, MRI was considered the gold standard for the diagnosis of BC, and mammography, MRI, and US results were compared. The incidence of BC in this group was 20%, with 39 out of 191 cases being BC on MRI.
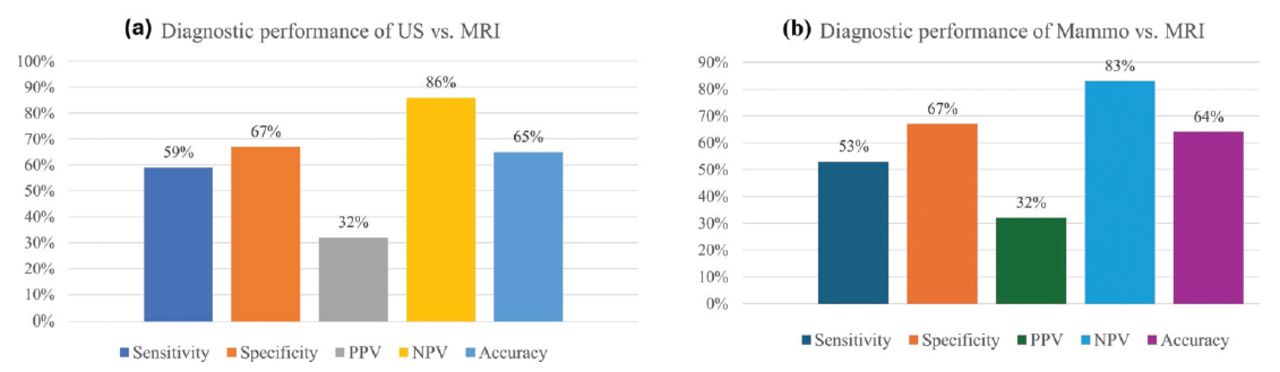
Table 2 shows significant agreement between US results and MRI results, with a kappa value of 0.20 (p=0.01). Out of the 118 cases initially diagnosed as benign on US, 102 were confirmed benign on MRI, while 16 were found to be malignant. Likewise, out of the 73 cases initially diagnosed as malignant on US, 50 were confirmed benign on MRI, while 23 were found to be malignant. Figure 3a shows the diagnostic performance of US compared with MRI.
- Comparison of ultrasound and mammography results with magnetic resonance imaging results.

- Comparisons of ultrasound (US) and mammography results with magnetic resonance imaging (MRI). a) Diagnostic performance of US vs. MRI. b) Diagnostic performance of mammography vs. MRI. Mammo: mammogram, PPV: positive predictive value, NPV: negative predictive value, MRI: magnetic resonance imaging, US: ultrasound
The results of mammography and MRI are also compared in Table 2, with MRI considered the gold standard. The kappa value for agreement between the 2 procedures was 0.16, which was significant with a p-value of 0.04. The initial mammogram analysis showed 93 benign results. According to the MRI results, there were 77 benign and 16 malignant tumors. Similarly, for the 56 malignant results that the mammogram showed initially, the MRI identified 38 benign and 18 malignant results. Figure 3b presents the diagnostic performance of mammography compared with MRI.
Table 3 shows that MRI had the highest specificity and PPV. Ultrasound was the most sensitive test for detecting BC and was the best test for NPV. Mammography and US, however, did not differ significantly when a tissue biopsy was not carried out.
- Summary of performance for all procedures with or without tissue biopsy.
Additionally, we categorized patients into 2 age groups: patients aged ≤30 years and patients aged >30 years. The incidence of BC was compared between the groups. In the young group (≤30 years), BC incidence was 50% (n=4/8) malignant, with no statistical significance (p=0.23).
Most mammography reports lacked comments on the presence of pathologically enlarged LN. However, LN abnormalities are important for US and MRI breast examinations. Magnetic resonance imaging and US showed no significant differences (p=0.39) regarding LN presence, and 258 patients showed enlarged axillary LN in both procedures. However, the presence of LN infiltration in the 258 patients differed significantly between the 2 procedures (US and MRI, p=0.04).
Discussion
Breast cancer has a global presence, and effective management, including examination and diagnosis, is essential to establish an effective treatment plan.16
Screening might not prevent BC, but it may assist in early detection, leading to beneficial treatment. Diagnostic methods have advantages and disadvantages, so it is essential to consult a specialist before undergoing any medical test.17 In the current study, we observed BC patients who underwent multiple screening procedures. We tried to limit the participants selection bias by using broad inclusion criteria of patients who have the same diagnostic procedures, and due to the inability to collect all patients’ data regarding histopathology, we classified them into 2 groups. We avoided the possibility of observer bias in the interpretation of images. Multiple radiologists independently reviewed the images. In addition, we have taken several steps to avoid bias in the interpretation of our research findings in general by providing detailed methodology and results to allow for critical assessment by reviewers.
As part of our study population, 119 patients underwent tissue biopsy, considered the gold standard modality. Malignant BC was diagnosed in 69% of cases and benign in 31% of cases in the all-age group with a mean age of 49. The MRI results were found to agree significantly with the compared tissue biopsy results. In identifying benign/malignant lesions, MRI had a sensitivity of 70% and specificity of 87%, along with PPV of 92% and NPV of 56%. Our results are supported by many previous studies, such as Lee et al18 who proved that MRI showed a 70-90% higher sensitivity in diagnosing BC patients with a familial or genetic tendency than mammograph.
Our study found that US sensitivity was 79% and specificity was 71%, and its PPV was of 84% and NPV of 63%. Conversely, mammography did not show significant agreement with tissue biopsy; its sensitivity was 75% and specificity was 41%, and its PPV was of 72% and NPV of 44%.
According to the current study, cystic lesions, intraductal masses, and microcalcifications could be detected with US, but abnormal breast density was better detected with mammography. It is to be mentioned that in the current study, US was able to identify calcifications in 10.2% of instances. Earlier studies found that US is a valuable noninvasive technique in detecting breast masses and distinguishing cystic from solid lesions, particularly in young or pregnant women, in whom mammography is non-advisable. In comparison, mammography is appropriate for detecting patients with non-mass breast lesions and microcalcifications.19
Ultrasound is an effective modality with high sensitivity (80%) and specificity (88%) in detecting BC, mainly in low-supply settings where mammography is inaccessible.20 Several investigations reported high sensitivity and NPV to 100% if US is utilized to recognize focal breast lesions.21 Mammography was found to be preferred in routine BC screening that starts in women at the age of 40-50 years, with a sensitivity of 73% and specificity of 55% in detecting BC.22 In addition, it was proved that the sensitivity of mammography (87%) is higher among older women and fatty breasts than dense breasts.23
Magnetic resonance imaging was considered the gold standard in cases without tissue biopsy, and there was little difference between mammography and US results compared with MRI results in these patients. Ultrasound had a PPV of 32% and a NPV of 86%, with a sensitivity of 59% and specificity of 67%, while the sensitivity of mammography was 53% and specificity was 67%, with a PPV of 32% and a NPV of 83%. These findings are explained by the unique characteristics of MRI as an advanced imaging modality, such as its ability to characterize tissue well, use multisequence imaging, and utilize contrast media. Magnetic resonance imaging could detect multiple enlarged axillary LN, suspected DCIS, invasive carcinoma, non-mass enhancement, multiple enhancing nodules, morphologically benign masses, and abnormal intramammary LN in our study.
Recent studies on breast screening modalities have revealed that MRI is more sensitive than mammography and US, regardless of tumor type, breast density, or personal history, and MRI alone carries out better than mammography and US combined. Moreover, specificity appeared to be affected by tumor size, type, and patient history, and US alone was observed to have the highest specificity when correlated to breast density.24 Furthermore, MRI-guided biopsy can be used without mammography or sonographic correlation to verify precise testing and develop an effective treatment plan. Biopsy is suggested for lesions categorized as BIRADS 3 lesions in high-risk patients and BIRADS 4 or 5.25
In sum, breast MRI should be encouraged as a screening method for targeted female subjects with high-risk factors owing to its high sensitivity and specificity and its advantages as a safe, noninvasive technique with the possibility of obtaining a tissue biopsy guided by MRI images. Hence, among the screening modalities, MRI stands out as the most sensitive method unaffected by breast density. It can be particularly beneficial for women with dense breasts, offering advantages over mammography.6,26,27 In our research, lesions in young women (≤30 years) were 50.0% malignant and 50.0% benign, and included malignant solid masses, morphologically benign masses, multiple enhancing nodules, and ductal enhancement.
In our study, MRI showed high sensitivity and specificity in detecting abnormalities in 15.5% of female patients with breast augmentation, implant reconstruction, and breast reduction. Mammography could not detect any abnormalities, while US results were equivocal. This agrees with Langman et al28 who stated that in patients considering breast conservation, MRI could detect disorders that could not be viewed on US or mammography and assist in clinical decisions.
According to our findings, the risk factors showed by MRI screening were implants, previous history of BC, post-chemotherapy, post-excisional biopsy, and BC mastectomy. This agrees with the risk factors of BC incidence globally, which also include the following: early menarche (delayed menopause), late marriage age, birth control medications, sedentary lifestyle, obesity, and bad consumption habits (smoking and drinking alcohol.16 However, we did not find a significant correlation between risk factors and age; lesions incidence was 50.0% malignant and 50.0% benign among young women (≤30 years), and 70.3% malignant and 29.7% benign among older women (>30 years). Consequently, we proved that age was not a predictive factor of lesions in this current study.
Although mammography can detect enlarged axillary LN, it cannot determine whether they are benign or malignant. Many patients may present with enlarged axillary LN without palpable breast masses or with microcalcification detected by mammography. Ultrasound and MRI have a significant role in such cases. They can detect and specify the nature of pathologically enlarged LN, which aids in cancer grading and avoids further metastasis. Our results showed that MRI detected suspicious LN in 69.7% and US detected suspicious LN in 44.2% of cases.
From our study protocol, we found that axial short tau inversion recovery images are important sequences to differentiate between mass lesions and cystic lesions. In addition, we used dynamic contrast enhancement T1 (fat saturation) multiple measurements; this technique is used to identify the characterized enhancement of masses in the breast and to catch the arterial, venous, and delayed phases. It is sensitive for detecting abnormal ducts and describing malignant masses versus benign masses. Further, subtraction images can be obtained from pre- and post-contrast images of T1 fat-saturated measurements, which is very useful for detecting any abnormalities. The diffusion sequence is also very significant; it can differentiate the type of lesion, such as malignant or benign, compared with the apparent diffusion coefficient.
Study limitations
Because the hospital’s PACS system was undergoing upgrades and changes, we could not collect all the data related to the histopathology and biopsy of all patients. As a result, we divided our participants into 2 groups: those who had biopsy results and those without. The data were collected from a single hospital, which might introduce selection bias. Multi-center studies could provide a more representative sample and enhance the generalizability of the findings.
In conclusion, MRI is a good positive test for diagnosing BC owing to its high PPV (92%) compared with mammography and US, while US is a good negative test, meaning diagnostic for not having BC, with a high NPV (63%) compared with MRI and mammography. In addition, MRI showed high sensitivity in detecting breast lesions and high specificity in characterizing their nature when correlated with pathological results. Therefore, owing to the high prevalence of BC among Saudi women and the multiple risk factors encountered in this community, we recommend that women with a high risk of BC start screening using US, with MRI as the next step if no lesions are detected or in the presence of suspected lesions. This will increase the detection rate of breast lesions among this group of women, reduce unneeded tissue biopsies, and enhance the disease’s survival rate.
Acknowledgment
The authors gratefully acknowledge Cambridge Proofreading LLC (www.proofreading.org) for their English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received October 6, 2023.
- Accepted July 4, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.