


Abstract
Objectives: To study which factors increase the risk of persistent disease in differentiated and poorly differentiated thyroid carcinoma.
Methods: A retrospective chart review of all consecutive differentiated and poorly differentiated thyroid cancer patients from King Abdulaziz University Hospital, Jeddah, Kingdom of Saudi Arabia, a tertiary care center, between 2004 and 2018. Logistic regression analysis was performed to predict factors associated with less than excellent response to treatment.
Results: We included 186 patients with complete data records; 81.1% were females. Papillary thyroid carcinoma comprised 88.1% of the neoplasms. In total, 55.9% of patients attained an excellent response to treatment by the end of the first year following treatment. All patients with distant metastasis had persistent disease. On univariate analysis, female gender was associated with excellent response (p=0.002). Lymph node metastasis, extrathyroidal extension, vascular invasion, and cancer multifocality were all found to be inversely related to excellent response (p<0.05 for all). On multivariate analysis only lymph node metastasis was associated with a decreased adjusted odds of an excellent response (p=0.007).
Conclusion: Patients with lymph node metastasis are at high risk for persistent disease following initial thyroid cancer management. Careful monitoring of these patients is warranted.
The global incidence of well-differentiated thyroid carcinoma (WDTC) has risen over the past few years.1 In the Kingdom of Saudi Arabia, WDTC is ranked as the third most reported malignancy among adults based on the most updated Saudi Cancer Registry data.2 Despite the increasing frequency of diagnosis, WDTC mortality has remained fairly stable over the years.3 Therefore, the main concern with WDCT is detecting and managing persistent disease (PD) and recurrent disease (RD), manifested either clinically or biochemically. The distinction between RD and PD after initial therapy was introduced to the literature in recent years. Not attaining excellent response outcomes in the early follow-up period after treatment might indicate PD rather than RD. Sappupo et al4 identified RD as evidence of disease after one year of being disease-free, while PD denotes never reaching a disease-free state after the initial therapy.
While thyroid cancer’s specific pathology is a good initial predictor of recurrence or a disease-free state, a better estimation can be obtained by the patient’s response to initial therapy, especially considering the currently available, highly sensitive thyroglobulin (TG) assays.5 The 2015 American Thyroid Association (ATA) guidelines have defined 4 possible response outcomes to WDTC treatment.6 An excellent response (ER) is considered the best outcome following therapy, with the risk of recurrence as low as 1-4% over 5-10 years of follow-up.7,8 The majority of low- and intermediate-risk WDCT patients achieve an ER post-treatment. However, some patients do not achieve an ER.8
In this research, we aimed to identify the epidemiological, histological, and therapeutic factors that influence the odds of PD and failure to achieve an ER to therapy within the first year following thyroid cancer management.
Methods
We performed a retrospective electronic chart review of all WDTC patients who were followed up at King Abdulaziz University Hospital, a tertiary care center, from 2004 to 2018. Inclusion criteria included all patients 12 years or older with adequate histological and staging data. Exclusion criteria included anaplastic or medullary thyroid carcinoma patients and patients with incomplete documentation of data in their files. Only patients with complete data records and sufficient follow-up and investigations at one year following definite management comprised the final study group. The Biomedical Ethics Committee at King Abdulaziz University approved the study.
Two hundred and eighty five thyroid cancer patients were found in our registry. After applying the inclusion and exclusion criteria, a total of 186 thyroid cancer patients with valid outcomes one year following therapy were included in the final study cohort. The remaining 99 patients were lost follow-up or did not reach the one-year mark after treatment and were excluded. Most of the excluded patients (86.9%) were low to intermediate risk, and the remaining 13.1% were high-risk patients. Two died, one secondary to advanced WDTC, and the other was low risk, and the cause of death was not related to thyroid cancer.
For each patient, age, gender, histopathological details, and stage of thyroid cancer were collected along with the utilized lines of management. The stage of thyroid cancer was categorized based on the 8th edition of the American Joint Committee on Cancer/Tumor-Node-Metastasis (AJCC/TNM) Staging System for Differentiated and Anaplastic Thyroid Carcinoma.10
The treatment outcomes at the end of one-year post-therapy were assessed based on the most updated ATA guidelines on response to treatment classification published in 2015. For patients who underwent total thyroidectomy with radioactive iodine (RAI) ablation, an ER to therapy was defined as a suppressed TG less than 0.2 ng/ml and stimulated TG less than 1.0 ng/ml with confirmatory neck ultrasounds and negative TG antibodies or decreasing titers. For patients who underwent total thyroidectomy but did not receive RAI, an ER was similarly defined. For patients who underwent lobectomy, an ER was identified as a postoperative TG of less than 30 ng/ml, with either stable or declining levels during follow-up in addition to confirmatory postoperative neck ultrasounds. Patients were considered to have PD if they had never achieved an ER to therapy in the first year following treatment.
Statistical analysis
Statistical analysis using IBM SPSS Statistics for Windows, version 20 (IBM Corp., Armonk, N.Y., USA) was applied to assess and test the hypothesis. All p-values are 2-sided, and a p<0.05 was considered statistically significant. Binomial logistic regression analysis was utilized to predict the probability of an excellent response associated with a dependent clinical or histological factor based on one or more independent factors. The results of the study are expressed as odds ratios (ORs) and 95% confidence intervals.
Results
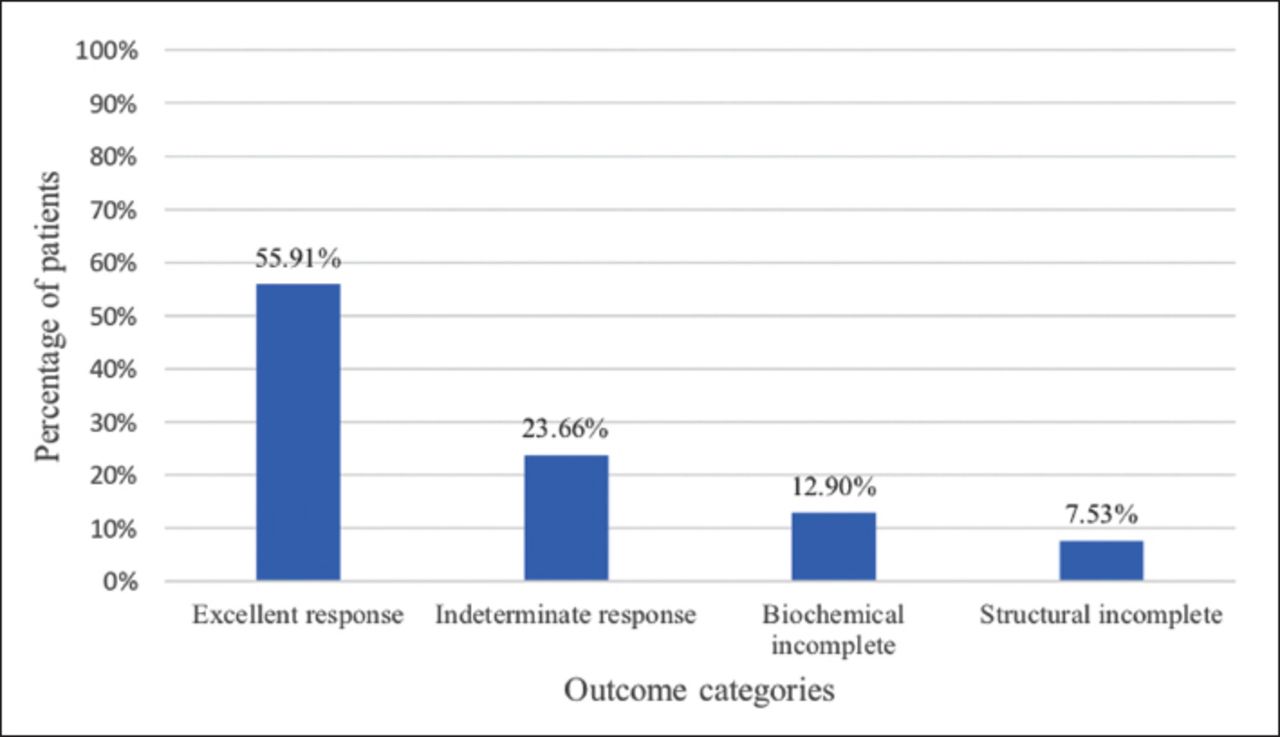
Table 1 demonstrates the baseline demographics and characteristics of the study patients. Of the final study cohort, 104 (55.9%) patients had an ER to therapy after one year. Of the remaining 82 patients, 44 (23.7%) patients had an indeterminate response; 24 (12.9%) had biochemically incomplete response and 14 (7.5%) patients had structurally incomplete response to therapy (Figure 1).
Patient’s characteristics of 186 participants.

Thyroid cancer response to therapy at one year after treatment
We had 48 patients (25.8%) with positive lymph node (LN) metastasis. Of those, 26 (54.2%) had central LN metastasis (N1a), and 22 (45.8%) had lateral LN metastasis (N1b). None of the patients with distant metastasis attained an ER to treatment. In univariate analysis, female was found to be associated with an early ER (p=0.002). Extrathyroidal extension (p=0.002), LN metastasis (p<0.0001), vascular invasion (p=0.014), and tumor multifocality (p=0.009) were all found to be negatively associated with an ER in univariate analysis (Table 2).
Univariate analysis of predictors of excellent response at one year following therapy.
In multivariate analysis, LN metastasis was the only factor that reached statistical significance with decreased adjusted odds of an ER (p=0.007). Patients with LN metastasis had a 76% higher chance of having PD (Table 3).
Multivariate analysis of predictors of excellent response at one year following therapy.
Discussion
In the present study, we found that the majority of thyroid carcinoma patients achieved an ER to therapy in the early follow-up period. Regional LN metastasis significantly reduced the probability of an early ER to therapy and thus increased the risk of postoperative PD for WDTC patients. All patients with distant metastasis had PD and did not achieve an ER to treatment at the end of the one-year surveillance period. In a similar earlier study from Saudi Arabia, 44.8% of patients attained an ER to treatment by 6-12 months after RAI therapy, while the corresponding percentage was 55.9% in the current study.11 The lower rates of ERs in their study might be related to the larger number of patients who had more aggressive pathologies, such as LN metastasis and distant metastasis, extrathyroidal extension, and vascular invasion.
Lymph node involvement is linked to an increased likelihood of PD, as evidenced by many studies. The risk of PD is particularly heightened with the presence of large LNs, specifically those more than 3 cm in size or detected clinically preoperatively.12,13 The presence of more than 5 metastatic LN or extranodal extension was also identified as a predictor of PD, mainly if present in more than 3 LNs.14,15 Therefore, preoperative imaging is of great importance to assess the tumor as well as all the possible involved LNs and plan the extent of the neck surgery. Ultrasound of the neck is the chief imaging tool used for preoperative evaluation of thyroid carcinoma and should include all the surrounding LN groups with an additional fine-needle aspiration biopsy for the suspicious LNs. The Surgical Affairs Committee of the ATA also recommends cross-sectional imaging modalities such as contrast- enhance neck CT or MRI in cases of apparent extrathyroidal extension, bulky LNs, or LNs located in areas that are more challenging to be assessed by neck ultrasound such as the ones found posteriorly or inferiorly.16
Hence, the 2015 ATA guidelines on the management of adult patients with thyroid nodules and WDTC recommends “compartmental” neck dissection of the neck levels in case of clinically involved central LN or biopsy-proven lateral LN involvement.6 The goal of neck dissection surgery in WDTC is to remove all the LNs within at risk compartments to better stage the patient, guide adjuvant treatment, and avoid leaving PD or acquiring locoregional recurrence postoperatively.17
In addition, RAI therapy was also favored in patients with a large number of metastatic LNs, particularly more than 5, larger size LNs or with extranodal extension to reduce the risk of both PD and RD.6 This therapy is characteristically advocated in older patients with lateral neck LN involvement, for whom RAI and mainly high doses were associated with a reduced incidence of structural PD.18
Similar to our findings, multiple other studies found associations between specific WDTC histological findings and the risk of postoperative PD. In a retrospective study involving patients from the Canadian Thyroid Cancer Consortium Registry, microscopic positive tumor margins were found to be associated with an increased risk for PD but not RD in the early stages of WDTC.19 However, a conclusion regarding RAI therapy in such cases cannot be made based only on these data, and further prospective studies are needed. Vascular invasion was also found in a meta-analysis to be associated with PD,20 supporting the findings from our univariate analysis.
Study limitations
The limitations of our study are the retrospective and single-center nature of this research. Furthermore, we were limited to studying variables collected in our electronic medical system.
In conclusion, patients with lymph node metastasis are at high risk for PD following initial thyroid cancer management. Proper preoperative and surgical planning, as well as careful clinical, biochemical, and radiological monitoring of these patients are warranted.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received April 6, 2020.
- Accepted June 24, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}