


Abstract
Objectives: To investigate the long-term outcomes of differentiated thyroid cancer (DTC) and the predictive factors for excellent and incomplete responses to therapy on long-term follow-up of patients.
Methods: A retrospective chart review and analysis was carried out at King Abdulaziz University Hospital, Jeddah, Saudi Arabia. Demographic, histological, and therapeutic data were collected from patients older than 13 years at the time of diagnosis, with a minimum follow-up of 18 months. Outcomes were divided into excellent, indeterminate, biochemically incomplete, and structurally incomplete responses. Odds ratios (ORs) for predictors of incomplete response at the last visit were determined. We first tested associations univariately with incomplete responses, and then variables with significant associations were included in a multivariable logistic model.
Results: Among 230 patients with DTC, 61.7% had excellent responses to therapy on long-term follow-up, and 24.3% had incomplete biochemical and structural responses. The median follow-up was 4.6 years. Factors significantly associated with incomplete response to therapy in the multivariate analysis (p<0.05) were age >55 years (OR=5) and lymph node (OR=3.4) and distant metastases (OR=29). Older age did not affect the outcome in low-risk patients with DTC but was significantly associated with incomplete responses in those with intermediate risk (p=0.04) and high risk (p=0.003).
Conclusion: We strongly advocate incorporating age into recurrence risk assessment for patients with DTC.
The incidence of differentiated thyroid cancer (DTC) has increased over the last few decades, which can be attributed to incidental detection of occult cancers by imaging or pathology.1 In Saudi Arabia, thyroid cancer cases increased between 1990-2019 by 15-fold in females and 22-fold in males.2 Contrary to the global epidemiology, thyroid cancer is diagnosed at a younger age and with a larger mean tumor size in Saudi Arabia.3
Despite the progressive increase in incidence, disease-specific mortality rates have been internationally stable, with excellent survival rates. In the United States, the 5-year disease-specific survival (DSS) rate is reported to be collectively as high as 98.6%.4
Therefore, DTC management primarily focuses on recurrence risk. This is reflected in the most recent American Thyroid Association (ATA) guidelines and risk stratification system for DTC. The ATA dynamic risk stratification system for DTC is a well-validated tool used to predict the response to therapy and the risk of disease recurrence. Post-therapy, patients are classified into 4 categories based on their thyroglobulin (Tg) levels, thyroid antibodies, and imaging results: excellent, incomplete biochemical, incomplete structural, and indeterminate responses.5
The vast majority of low- and intermediate-risk patients with DTC attain an excellent response after treatment, with a low recurrence risk (1-4%) over 5-10 years of follow-up. However, some patients do not achieve this goal.6 In a previous study, we examined the factors associated with an excellent response to therapy in patients with DTC during short-term follow-up (6-12 months).7 In this study, we explored the long-term outcomes of patients with DTC and the predictive factors for an excellent response to therapy.
Methods
This research was a retrospective cohort study of thyroid cancer patients from 2012-2022 carried out at King Abdulaziz University Hospital, Jeddah, Saudi Arabia. Data were collected between October 2022 and January 2023 from hospital records. We included all patients with DTC aged 13 years and above at the time of diagnosis with sufficient data and a minimum follow-up period of 18 months or more since diagnosis. We excluded pediatric patients (younger than 13 years of age), those with insufficient data, and those with a follow-up duration of less than 18 months.
Ethical approval was obtained from the Biomedical Ethics Committee of King Abdulaziz University, Riyadh, Saudi Arabia (IRB reference no.: 113-2).
For each patient, we identified the following data: age and date of diagnosis, valid follow-up duration, gender, stage based on the 8th edition of the American Joint Committee on Cancer (AJCC) tumor-node-metastasis (TNM) staging system, histopathological data, and applied management lines, such as type of surgery and radioactive iodine therapy. Tumor risk stratification and response to treatment outcomes were determined according to the 2015 ATA guidelines for DTC.
Outcomes were divided into: excellent, indeterminate, biochemically incomplete, and structurally incomplete responses. If the patient had undergone total thyroidectomy but never received radioactive iodine therapy, the outcome was regarded as an excellent response if Tg <0.2 ng/ml, with stimulated Tg <1 ng/ml. The response was considered indeterminate if Tg was between 0.2-5 ng/ml and stimulated Tg was between 2-10 ng/ml. A biochemically incomplete response implied Tg >5.0 ng/ml, with stimulated Tg >10 ng/ml. In patients who underwent a lobectomy, an excellent response was defined as postoperative Tg <30 ng/ml, while an indeterminate response was defined as Tg >30 ng/ml. Mortality was identified and segregated according to thyroid cancer status.
Statistical analysis
All analyses were carried out using SAS 9.4 (SAS Institute, Cary, NC, USA), with the significance level set at 0.05. Means ± standard deviations (SDs) and frequencies with percentages (%) were used to describe continuous and categorical variables. The study sample was categorized into low-, intermediate-, and high-risk groups based on the initial ATA risk stratification. To compare descriptive statistics among risk stratification levels, we used analysis of variance and the Chi-square test for normally distributed variables and frequency distributions of categorical variables. Logistic regression was used to determine the odds ratios (ORs) and 95% confidence intervals (CIs) for the predictors of incomplete responses (biochemical and structural) at the last visit. Initially, we tested the associations individually for incomplete responses, and variables exhibiting significant associations were included in a multivariable logistic model. The Kaplan-Meier survival curve and Log-rank test were used to investigate the cancer-free survival probabilities of different age groups (>55 years and ≤55 years) and initial ATA risk groups (Low, intermediate, and high risks).
Results
We included 230 patients who fulfilled the inclusion criteria, most of whom were female (73.9%). Papillary thyroid cancer (PTC) was the primary cancer subtype, present in 92.6% of DTC cases. Upon diagnosis, most of the patients were classified as low risk based on the ATA risk stratification (45.2%). Approximately one-third of the patients showed evidence of lymph node metastasis (32.2%), and 8.7% showed evidence of distant metastasis. Table 1 presents the detailed histological characteristics of the study sample and the applied management lines based on the initial ATA risk stratification.
- Descriptive characteristics of the study participants overall and by initial risk status (N=230).
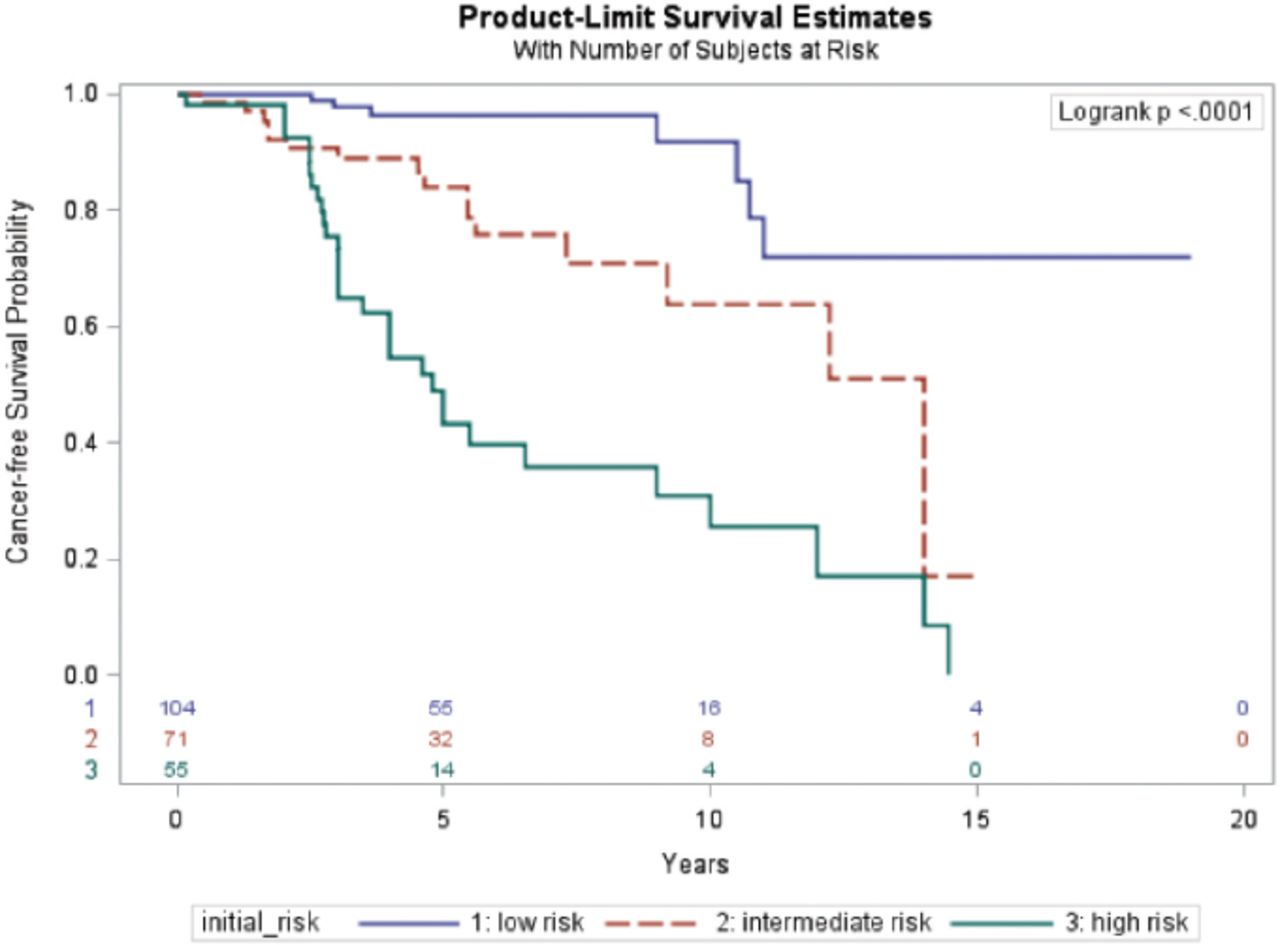
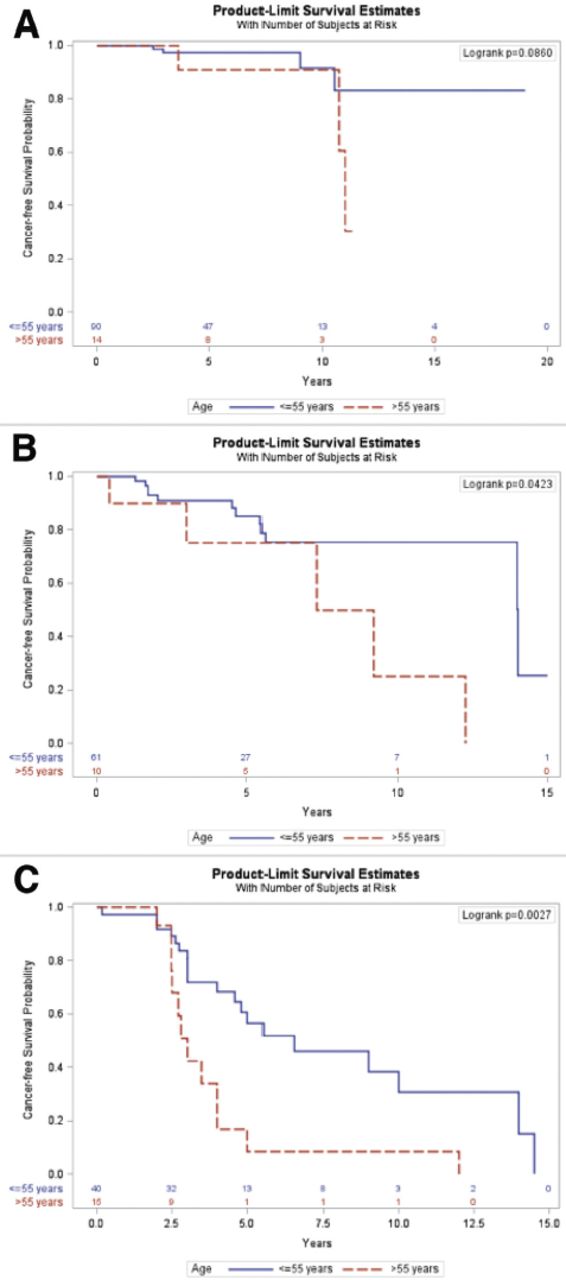
The median follow-up period for the study sample was 4.6 years, and most patients had excellent responses to therapy on long-term follow-up (61.7%). Nevertheless, 24.3% of patients had incomplete biochemical and structural responses. Patients with initial high-risk DTC upon presentation were more likely to have a structurally incomplete response to therapy at the final follow-up period (40%) compared to 9.9% of patients with intermediate risk and 2.9% of patients with low risk. A total of 8 (3.5%) patients died during follow-up. Mortality was directly related to metastatic thyroid cancer in 6 (2.6% of the total) patients, and 2 (0.9%) patients died due to causes unrelated to thyroid cancer (both died secondary to septic shock). Table 2 presents the long-term outcomes of the study cohort, categorized based on initial risk stratification. As the initial risk increased, the probability of cancer-free survival decreased, as illustrated in Figure 1. Our analysis indicated that age did not significantly affect the outcome or probability of an excellent response in patients with a low-risk initial stratification (p=0.135), as shown in Figure 2A. In contrast, older patients (>55 years) with intermediate and high risks had a higher chance of incomplete response and lower cancer-free survival compared to younger patients aged ≤55 years. Similarly, older patients (>55 years) with high risk also had higher chance of incomplete response and lower cancer free survival (p=0.003) as shown in Figures 2B & 2C.
- Long-term outcomes based on initial risk (N=230).
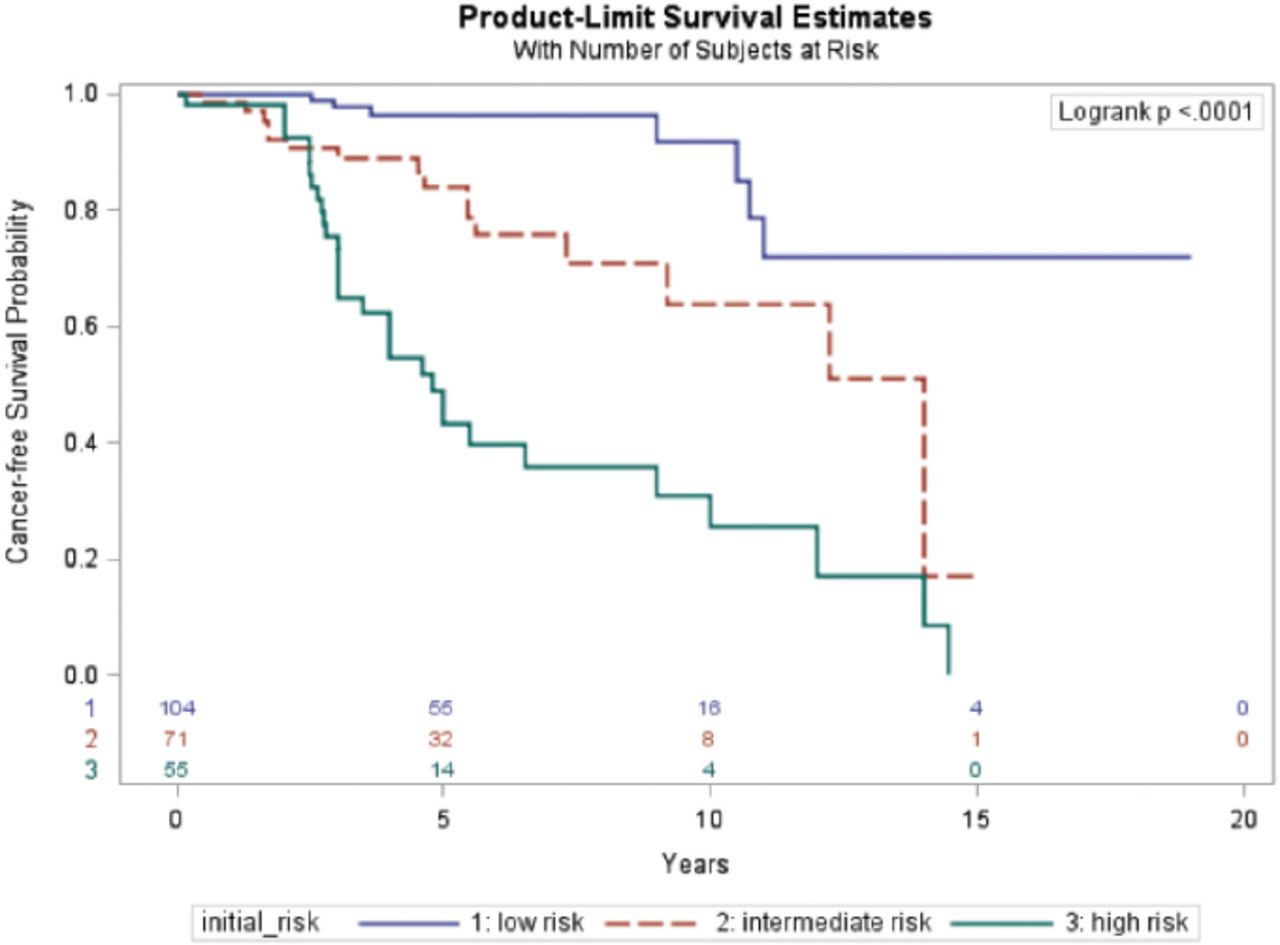
- Cancer-free survival probability among different initial American Thyroid Association risk groups.
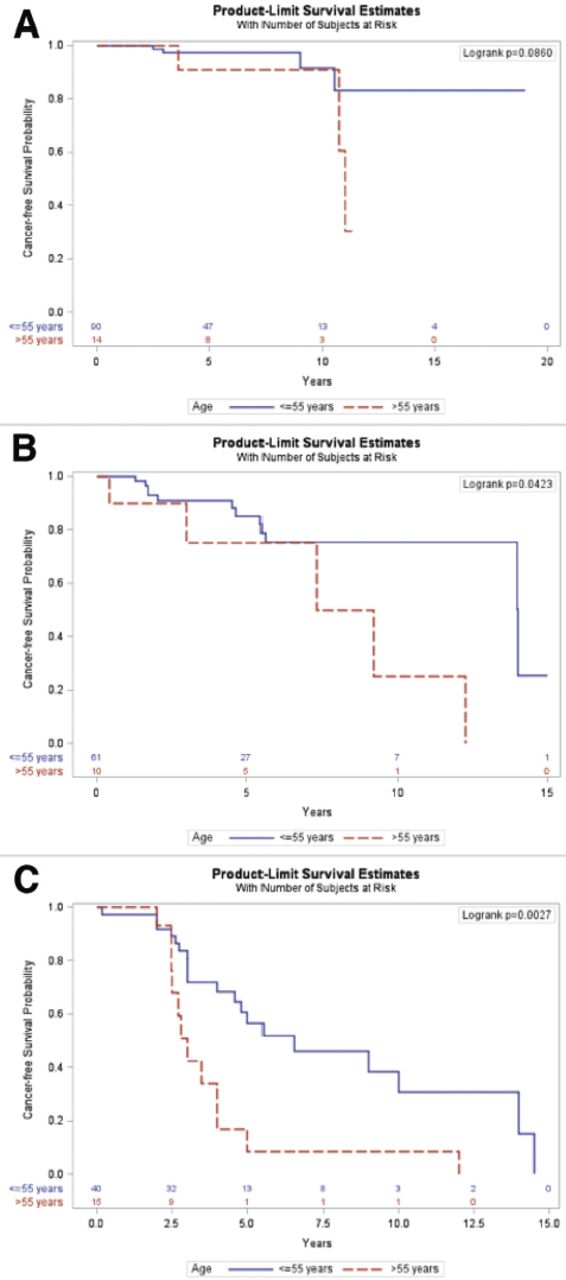
- Probability of cancer-free survival in differentiated thyroid cancer patients based on the risk. A) Low risk; B) intermediate risk; and C) high risk.
When analyzing the factors associated with an incomplete response (both biochemical and structural) to therapy, we found that older age (>55 years) was significantly associated with a higher probability of an incomplete response to therapy (OR=5, p=0.001) in multivariable analysis. Furthermore, using multivariable analysis, incomplete response to the therapy was found to be significantly associated with the presence of lymph node metastasis (OR=3.4, p=0.01) and distant metastasis (OR=29, p≤0.0001). Extrathyroidal extension (ETE), multifocality, vascular invasion, and tumor size, were associated with poor outcomes or response to therapy only in the univariate analysis but did not reach statistical significance in multivariable analysis. Gender, non-papillary tumor type were not associated with incomplete response to therapy. Table 3 presents the full details of the factors affecting the probability of an incomplete response to therapy.
- Odds ratios (95% confidence interval) for predictors of incomplete response (reference value of excellent and indeterminate responses).
Discussion
In our study, most patients with an initial low (77.4%) or intermediate risk (66.7%) of recurrence had an excellent response to therapy on long-term follow-up. Only 25.5% of the patients with an initial high risk had an excellent response to therapy, and 50% had evidence of either biochemical or structural disease on long-term follow-up. In a similar Saudi study carried out in 2022, the excellent response rate among high-risk patients was 27%, which is similar to our findings. However, 81.7% of intermediate-risk patients achieved an excellent response.8 Correspondingly, a study carried out in the Netherlands produced similar results, where 29% of patients with a high risk of developing DTC had an excellent response and 51% had evidence of structural recurrence.9
Regarding the predictors of an excellent versus incomplete response to therapy, our study found that older age (>55 years) was associated with an incomplete response (both biochemical and structural) even after adjusting for other factors. The influence of age was prominent in patients with intermediate- and high-risk DTC. The effect of age was not evident when the initial risk was low. There is a growing evidence that age is a key factor affecting recurrence risk, as discussed recently in multiple local and international studies in which patients aged <55 years had higher rates of overall survival, cancer-free survival, and cancer-specific survival compared to patients aged >55 years.8,10,11 Shah et al12 found that patients younger than 55 years with a high risk (ATA classification) had twice the probability of producing an excellent response to therapy compared to older patients.
Age is not considered as an independent predictor of DTC recurrence in the current ATA risk stratification. It is only included in the TNM staging system to predict mortality. Therefore, Ghaznavi et al13 proposed integrating the TNM classification (8th edition) with the 2015 ATA risk stratification system to enhance risk assessment for patients with DTC and provide a more accurate representation of DSS on long-term follow-up. The authors concluded that regardless of age, if the patient had an initial low-to-intermediate risk, the DSS was close to 100%. In contrast, older patients with an initial high risk at a stage higher than stage I had an estimated DSS of 61%, while young high-risk patients with stage II disease had an estimated DSS of 78%. Additionally, their cohort had a 2.5% thyroid cancer-related mortality rate, which is similar to the 2.6% reported in our cohort.13
Lymph nodes are a common site of DTC metastasis, and the presence of lymph node metastasis has a negative impact on both recurrence risk and survival, especially if the metastatic focus is >3 cm.14,15 We noted in a previous publication that lymph node metastasis is associated with an incomplete response to therapy during short-term follow-up (6-12 months).7 In this study, we extended our statistical analysis to a long-term follow-up (>18 months) and found that lymph node metastasis negatively affected the probability of obtaining an excellent response to therapy. An additional study carried out on 829 PTC cases supports our results, demonstrating that the presence of lymph node metastasis is an independent predictive factor for distant metastasis and recurrence in patients with PTC.16
Despite being significantly associated with an incomplete response to therapy in our univariate analysis, vascular invasion did not reach statistical significance in the multivariate analysis (p=0.18). This is consistent with a study from the Philippines that found no relationship between vascular invasion and an incomplete response to therapy.17 One systematic review carried out in 2017 is not consistent with our results, as it indicated that the presence and extent of vascular invasion should be considered a predictor of adverse outcomes in DTC and is associated with an increased risk of recurrence and mortality.18
The ETE is a well-established risk factor for recurrence and mortality and has been included in several risk stratification and staging systems. In this study, we found that ETE was strongly associated with an incomplete response to therapy in the univariate analysis only (p<0.0001). In a study that included 160 patients with DTC, Weber et al19 found that structural recurrence rate was not significantly different among patients with microscopic ETE compared to tumor confined to thyroid gland. However, this finding is not universal, as other researchers have found that even minimal ETE can impose recurrence risk and produce an incomplete response to therapy.20 In Bortz et al’s21 study, patients with minimal ETE had a worse 10-year survival rate than those with intrathyroidal disease (89.3% vs. 93.1%).
Finally, we found that gender, multifocality, and non-papillary DTC pathology were not associated with poor outcomes or responses to therapy in the multivariate analysis. The impact of gender on DTC recurrence has been extensively investigated, yet it remains a topic of debate. In a study utilizing the National Institute’s Surveillance, Epidemiology, and End Results database to investigate the effect of gender on DTC recurrence risk, the results indicated that DSS for women under the age of 55 years was significantly better than that of men (hazard ratio [HR]=0.33, CI: [0.13-0.81]). However, for women aged 55-69 years, the HR for DSS was comparable to that of men (HR=1.01, CI: [0.42-2.37]).22 In another study from the Canadian Collaborative Network for Cancer of the Thyroid, men had a greater risk of DTC recurrence compared to women (HR=2.31, CI: [1.48-3.60], p<0.001) after adjusting for TNM stage.23
Multiple studies have suggested that multifocality is associated with increased recurrence risk.24,25 In 2019, a published study demonstrated that multifocality is an independent risk factor for recurrence in PTC of >1 cm but not in papillary thyroid microcarcinoma.26 However, in our study, multifocality did not reach statistical significance in the multivariate analysis as an independent risk factor for recurrence (p=0.20). Further, in the most recent ATA guidelines for DTC, multifocality is not considered a factor that increases patient risk stratification.
Concerning tumor size and thyroid cancer outcomes, Tran et al27 studied 574 patients diagnosed with PTC and concluded that a tumor size of >2 cm is associated with unfavorable outcomes and an increased risk of mortality only in patients older than 55 years. In another study from Saudi Arabia, tumor size was significantly associated with an incomplete response to therapy in initial intermediate- and high-risk patients but not in low-risk patients.8,28 In our study, tumor size affected the long-term outcomes in the univariate analysis but did not reach statistical significance in the multivariate analysis (p=0.31). Our sample size is 230 patients, while in the above mentioned studies, the sample size was more than 500 patients. We believe that our smaller number of included patients might explain the discrepancy. Future research can investigate this matter by utilizing a larger sample size and possibly conducting an analysis based on age.
Study limitations
Our study has some limitations, including its retrospective nature and the fact that it was carried out in a single center. On the contrary, this study is strengthened by the fact that it is among the few studies from Saudi Arabia with long-term thyroid cancer outcomes. It also supports the recent literature regarding the influence of age on recurrence/persistent disease in the field of DTC.
In conclusion, DTC is a common malignancy with low mortality, and most patients have an excellent response to therapy at their follow-up, even high-risk patients. However, tumor recurrence is still a significant morbidity concern and a cause of anxiety in patients with DTC. Age is currently not considered to be a factor influencing recurrence risk in patients with DTC. However, based on this research and others, we strongly advocate incorporating age into patient risk assessment to refine the intensity of the management, and properly allocating the expected outcome. Moreover, tumor histological factors, especially lymph node metastasis, significantly impact the risk of persistent and recurrent disease in the short and long term, which should then influence the intensity of follow-up and management.
Acknowledgment
The authors gratefully acknowledge Scribber (www.scribber.com) for English language editing
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received August 15, 2023.
- Accepted January 4, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.