


Abstract
We present an uncommon case of a 48-year-old female patient with symptomatic presentation of a severe aortic regurgitation with aneurysm of the ascending aorta and progressive dyspnea. Detailed investigation of laboratory tests and imaging identified Takayasu’s arteritis (TA) as the underlying etiology. Computed tomography scan revealed complete occlusion of the right carotid artery as well as stenosis at the origins of left subclavian and vertebral arteries. In addition, cardiac magnetic resonance angiogram showed aneurysm at the proximal segment of right subclavian artery. Intervention with corticosteroids effectively diminished the need for immediate surgical intervention. Treating physicians should always consider differential diagnosis of TA in the presence of atypical clinical findings in all patients with cardiac problems especially when there is valve involvement.
Takayasu’s arteritis (TA) is a rare chronic largevessel vasculitis, affecting mainly the aorta and its proximal branches.1 Women under the age of 40 years are predominantly affected by TA with the highest prevalence reported in East Asia, especially Japan and Korea.1 Takayasu’s arteritis may cause aortic stenosis, aortic aneurysm and to a much lesser frequency aortic regurgitation (AR). The diagnosis of TA is based on clinical findings, relevant serological tests, and imaging studies. Prognosis is dependent mainly on the disease activity and complications with cardiac involvement.1 Immunosuppressive therapy is the mainstay of TA management. Normally corticosteroids are used to induce remission followed by the introduction of steroid sparing drugs. Some severe cases may require surgical repair, but complications commonly occur due to the fragility of the valves because of the inflammation. Therefore, to improve the success rate of repair, surgical intervention is often best deferred until the inflammation has become well under control.2 We report here an atypical case of severe AR with aortic aneurysms a complication of TA to further increase awareness of the broad spectrum of TA presentation and varied ethnicity.
Case Report
Patient information
We present the case of a 48-year-old female patient from the southern part of Saudi Arabia, diagnosed 2 years earlier with dilated cardiomyopathy (DCM) and severe AR. She presented acutely with intractable cough, worsening of breathlessness on exertion along with orthopnea and occasional paroxysmal nocturnal dyspnea. Her New York Heart Association (NYHA) HF classification progressed from class II at the time of the diagnosis 2 years ago to class IV on her latest presentation. She reported few self-limited episodes of hemoptysis. She had no chest pain, palpitations or attacks of syncope. She reported fatigue, dizziness, weight loss, multiple first and second trimester abortions. In the most recent presentation, she reported recurring claudication of the upper limbs with previous history of painless bluish discoloration of left leg.
Clinical findings
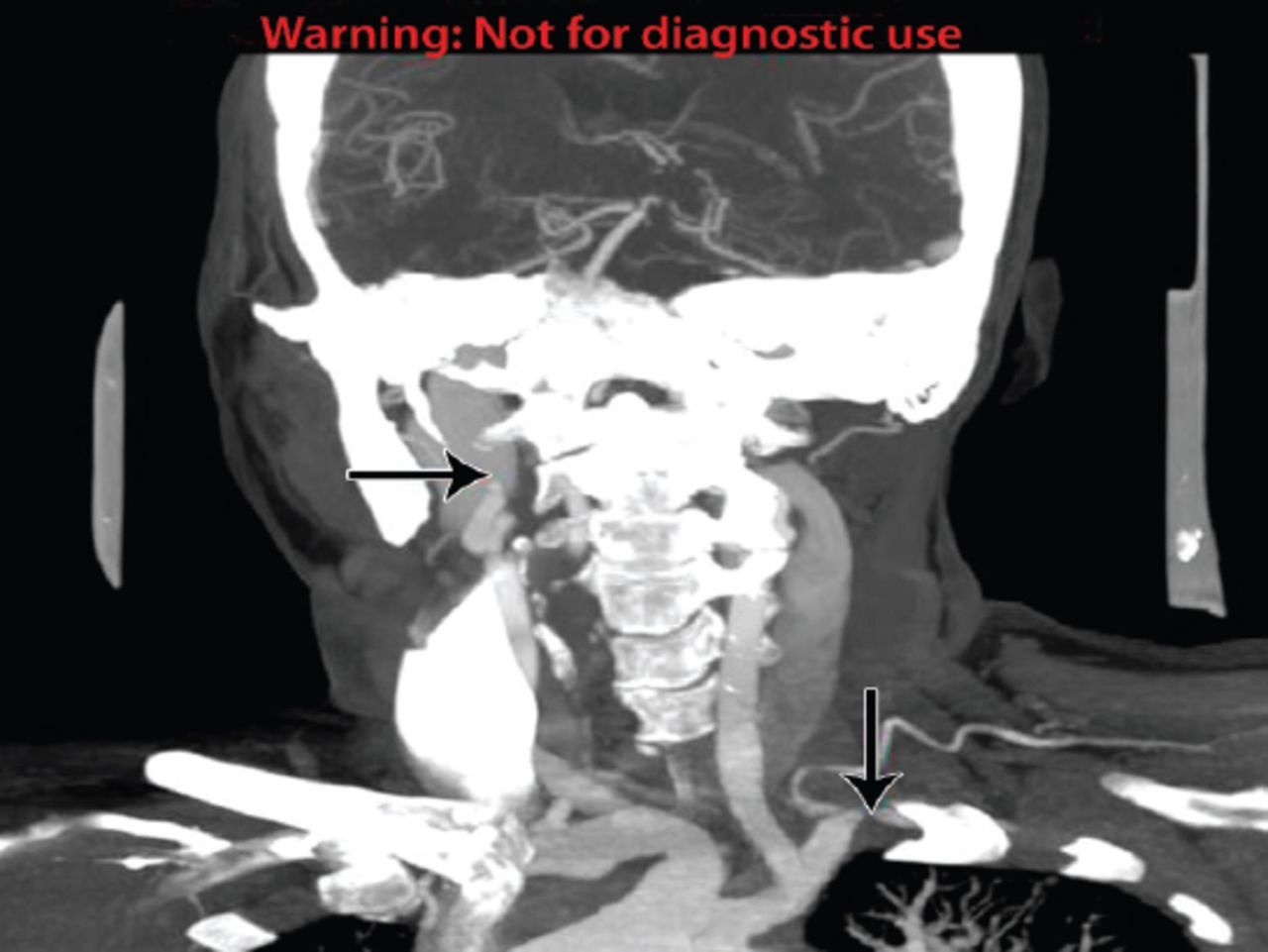
The patient was hypertensive and reported difficulty with measuring her blood pressure in the left arm. Clinical examination revealed a heart rate of 105/min, regular and collapsing. Radial pulse of left arm was feeble and of normal volume in the right arm. The blood pressure was recorded as 90/50 mmHg in the left arm and 130/53 mmHg in the right arm. On auscultation, there was an early ejection murmur at the left coastal margin consistent with AR. A bruit was heard over both carotid and the left subclavian artery. Angio-arteriography showed complete right carotid stenosis and less than 50% stenosis of the left carotid artery (Figure 1). Both left vertebral and subclavian arteries had segmental stenosis at the respective origins (Figure 2). There were no signs of weakness in the upper limbs noted, while the lower limbs exhibited ostinflammatory hypopigmented erythema nodosum like rash.

Complete occlusion of the right internal carotid artery and irregular outline of left subclavian artery with narrowed segment.

Severe narrowing at the origin of left vertebral artery. Segmental stenosis of the left subclavian artery is noted.
Timeline
Laboratory and serology test results demonstrated: white blood cells count (WBC) of 4.3 10 ^9/L, hemoglobin: 11.6 g/dl, platelets: 308, erythrocyte sedimentation rate (ESR): 42 mm/hour and a C-reactive protein (CRP) of 18 mg/L. The liver function tests, urea, creatinine, serum sodium and potassium were all within the normal range. The anti-nuclear antibodies (ANA) titer was 1/80 but the other auto antibodies tested, namely the anti-danti-double stranded DNA, cytoplasmic antineutrophil cytoplasmic antibodies, and perinuclear anti-neutrophil cytoplasmic antibodies did not show any rise in their respective titers. The imaging results of the CT scan revealed an old ischemic insult in the left basal ganglia. The echocardiogram exhibited 25% ejection fraction (EF), tricuspid aortic valve, mildly thickened leaflets, malcoapting cusps, opening well, and dilated aortic root. The angiography result was consistent with complete right side carotid stenosis, less than 50% stenosis in the left carotid, vertebral and subclavian arteries which had segmental stenosis at the origins. The renal magnetic resonance angiogram (MRA) showed dilation of infra and supra renal aorta (Table 1).
Time line including follow up visits diagnostic tests and interventions.
Diagnostic assessment
Following the cardiac MRA which showed right subclavian aneurysm, the patient was diagnosed with TA. She exhibited 5 out of the 6 major clinical diagnostic criteria developed for TA classification.1
Therapeutic intervention
Due to the fragile and inflamed vascular tissues, the planned aortic and mitral valve replacement surgery was postponed and immunosuppressive treatment initiated promptly. She was commenced on pulse therapy with 500 mg dose of methyl prednisolone daily for 3 days followed by 60 mg of oral prednisolone for 4 weeks. The dosage of prednisolone was tapered down by 5 mg weekly until reached the maintenance dose of 5 mg a day. She was also given regular low dose aspirin (81 mg).
Follow-up and outcomes
She improved clinically in response to the above measures. She reported minimum claudications and dyspnea during the follow up. The CRP was less than 1 and the ESR was 5 mm/h. The EF was 55% (Table 1).
Discussion
Takayasu’s arteritis often referred to as the “pulseless disease” is a chronic disease with variable severity and clinical manifestations, progression of which may cause damage to the arterial walls resulting in adverse outcomes such as rupture of the arteries.3 Such vascular complications in untreated patients with TA are the leading causes of morbidity and mortality.3 Initiating aggressive treatment for severe cases improves outcomes with a reportedly close to 90% 5-year survival rates.4 The diagnosis of TA is often made later when complications become evident posing a formidable challenge for early management and treatment of the disease. The difficulty for accurate TA diagnosis is compounded by the lack of specific diagnostic serologic tests; traditional biomarkers such as CRP and ESR levels are indicative of clinical inflammation but not all cases of active TA disease present with changes in ESR and CRP levels.5,6 Therefore, high index of suspicion is warranted in patients presenting with angina without any other identifiable risk factors or young adults diagnosed with hypertension and arterial bruits.
We have reported an uncommon case of a middle-aged female patient presenting with severe AR associated with aortic aneurysm as a secondary complication of TA. The carotid, subclavian, and vertebral arteries were all involved. The clinical diagnosis of TA in this patient was only established following the AR symptomatic presentation. The definitive diagnosis of TA was supported by the above findings together with the asymmetrical arm blood pressures, claudication symptoms, hypertension and the classical radiological changes. Over the past decade, the time frame from disease onset to clinical diagnosis has gradually diminished thanks to the advent in improved imaging modalities and medical treatment options. The classical characteristics of TA were not apparent in our patient at the time of diagnosis with AR and DCM. However, at later presentation the clinical features of TA were salient and it is plausible that a flare up was the reason for the worsening of her cardiac condition and the appearance of the diagnostic TA indications. Although the patient was diagnosed with TA at a relatively later stage, the condition; however, was amenable to immunosuppressive therapy and symptoms improved adequately to allow for the postponement of the surgical intervention. Despite improvement following surgery, valve detachment after anastomotic aneurysm may still occur due to the fragility of aortic wall or annular tissue because of TA.4 Previous studies5,7 found that immunosuppressive agents achieved remission in patients with TA anywhere from 46% to 84% success rate. Similarly, early medical intervention for TA management prior to surgery even with complication of severe forms of AR has been further demonstrated with implementation of effective treatment using newer biological agents.6 Surgical intervention with valve or root replacement in patients with active disease can be very challenging and carries high complications rate due to the fragility of the inflamed tissue, which may lead to valve detachment or anastomotic aneurysm formation. Surgical intervention is therefore best delayed for the vascular inflammation to be sufficiently treated with immunosuppressive therapy.
Aortic valve regurgitation has been reported as a complication of up to 25% of TA cases.8,9 However, AR associated with aneurysm of the ascending aorta is a relatively rare complication of TA with few cases published in more than 3 decades.6,9 The clinical presentation, treatment approaches and outcomes have been variable in these case reports with the differences primarily due to the changes in treatment modalities. It is now generally accepted to only consider surgical intervention after the medical therapy is instigated in order to reduce inflammation to manageable levels.5 McGraw et al9 also suggested a delay in the surgical intervention was deemed necessary as it complicated the need to manipulate the inflamed tissue leading to worsening of the outcome such as valve detachment or dilatation of the residual aorta. Previously, Matsuura et al8 reviewed the late outcome of surgical treatment for aortic valve regurgitation due to TA and its relation with inflammation over 24 years in 90 patients and found an overall survival rate of 76.1% after 15 years follow up. The authors findings further showed presence of active inflammation in 10 pathological specimens 4 of which showed detachment of the valve or graft confirming that active inflammation is a major risk factor for detachment.8
Previous studies have reported significantly increased survival rates following aortic valve replacement in patients with AR complication secondary to TA condition.4,10 Kaku et al4 review of cardiac operations over 30 years in 20 patients with AR associated with TA revealed a 5-year survival rate of 90.9% after surgery with no case of valve or composite graft detachment evident.4 In our findings, 2 patients required a repeat of aortic root replacement while 2 other patients developed late dilatation of the residual thoraco-abdominal aorta.4 Similarly, Li et al10 found satisfactory outcomes with no case of valve detachment in patients with TA and surgical treatment of AR.10 Despite the rare association of AR with TA, physicians should be alert to the possible diagnosis of TA given the high incidence of coronary artery diseases among these patients.
In conclusion, this case demonstrates a rare presentation of severe AR with aortic aneurysm secondary to TA in a middle-aged female patient of Arabian origin. High index of suspicion is necessary for early diagnosis of patients with TA to reduce or prevent further complications and adverse outcomes. The immunosuppressive therapy has proven as an effective perioperative measure in this case study and may benefit other patients with established cardiac complications by reducing or delaying the need for surgical intervention.
- Received March 12, 2017.
- Accepted June 22, 2017.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.