


Abstract
Traumatic female urethral avulsion in the absence of a pelvic fracture is an exceedingly rare entity, with no consensus on its management. Here, we present a 35-year-old pregnant woman with severe anterior vaginal wall laceration and complete urethral avulsion secondary to straddle injury. Management consisted of primary urethral and vaginal repair.
Complete circumferential rupture of the female urethra is extremely rare, and represents a challenging management situation.1 As the entire posterior length of the urethra is closely adherent to the anterior wall of the vagina; it is subsequently prone to simultaneous injury. Most reported cases were associated with pelvic bone fractures, but there is no current consensus on management.2 The diagnosis should be considered in cases of deep vaginal lacerations, with an inability to void with unsuccessful catheterization.3 Our objective in presenting this particular case is to highlight that early recognition and strict adherence to the principles of reconstructive surgery are necessary to maximize the results and prevent subsequent risks of morbidity.
Case Report
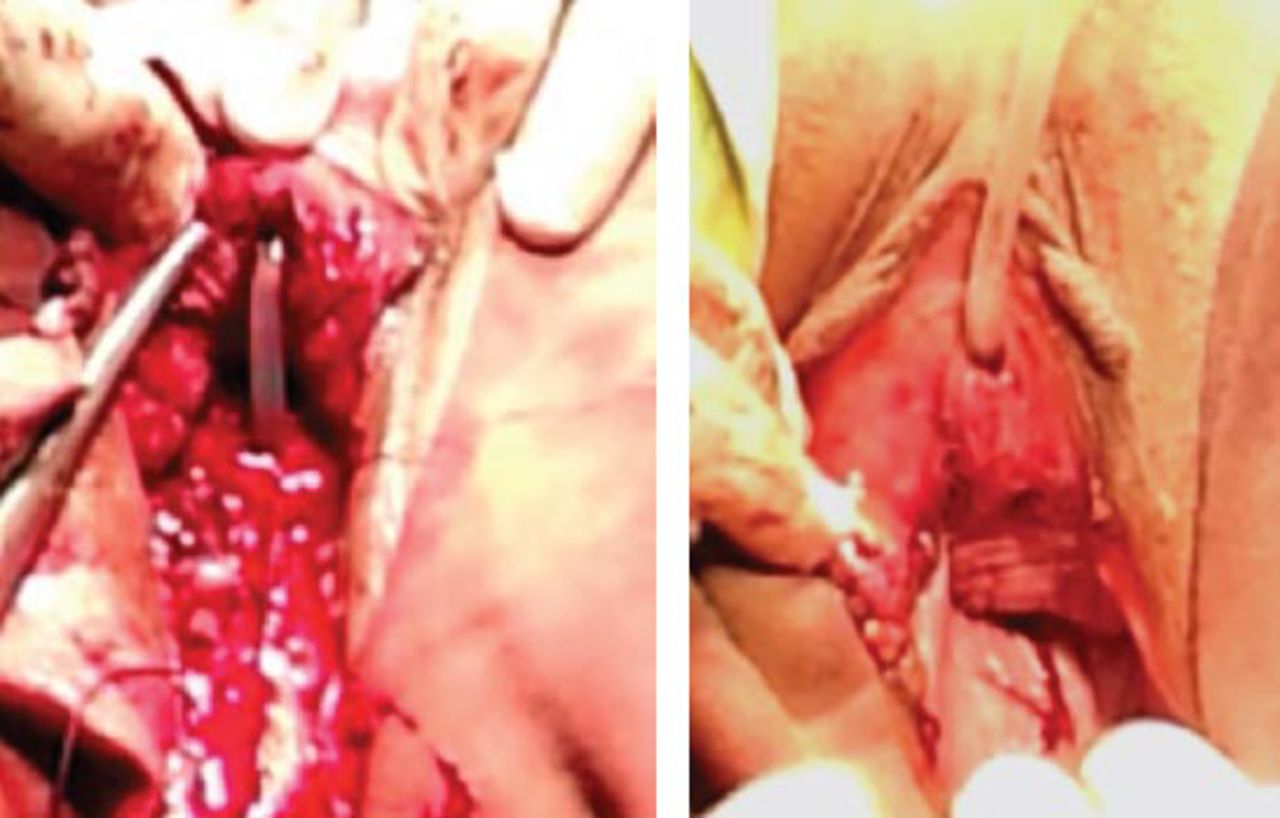
A 35-year-old woman in the sixth month of pregnancy, presented to the emergency department post fall down straddle injury onto a sharp object (rock), during her work as a farmer. Her injuries involved the genitalia. There was profuse vaginal bleeding with an inability to pass urine. Examination revealed severe laceration of the anterior vaginal wall with complete urethral avulsion (Figure 1). Abdominal ultrasound findings showed that the urinary bladder was full and tender, with no intra-abdominal collection. The fetus was alive in the 26th week, with a cephalic presentation. Full informed consent was obtained for the possibility of preterm termination of pregnancy, urinary diversion, urethral stricture or fistula, incontinence, vaginal infection, or stenosis. Emergency surgery under general anesthesia, in the dorsal lithotomy position with hemostasis was carried out. A small catheter was passed from the anteriorly displaced meatus for 2 cm in the intact distal urethra, to the level of the avulsed urethra. Thereafter, the catheter was manipulated back into the bladder, until urine passed through the catheter from the urinary bladder. Primary urethral repair was performed trans-vaginally with end-to-end urethral anastomosis over stenting silicone catheter by interrupting 5/0 vicryl. The muscularis over the urethra was closed in a second layer, and the vaginal mucosa was then closed as a third layer by 2/0 vicryl; with an attempt being made to offset the suture line from the muscular closure (Figures 2a & 2b). The catheter was removed 4 weeks postoperatively, and the repair was intact. She was fully continent and voided satisfactorily with a good stream. At full term, a lower cesarean section was carried out and yielded a well baby of 3 kg. She was followed up every 2 months for 2 years to monitor any lower urinary tract symptoms and sexual dysfunction. Two years post surgery, she is continent with a good stream of urine with a normal sexual life (Figure 3).
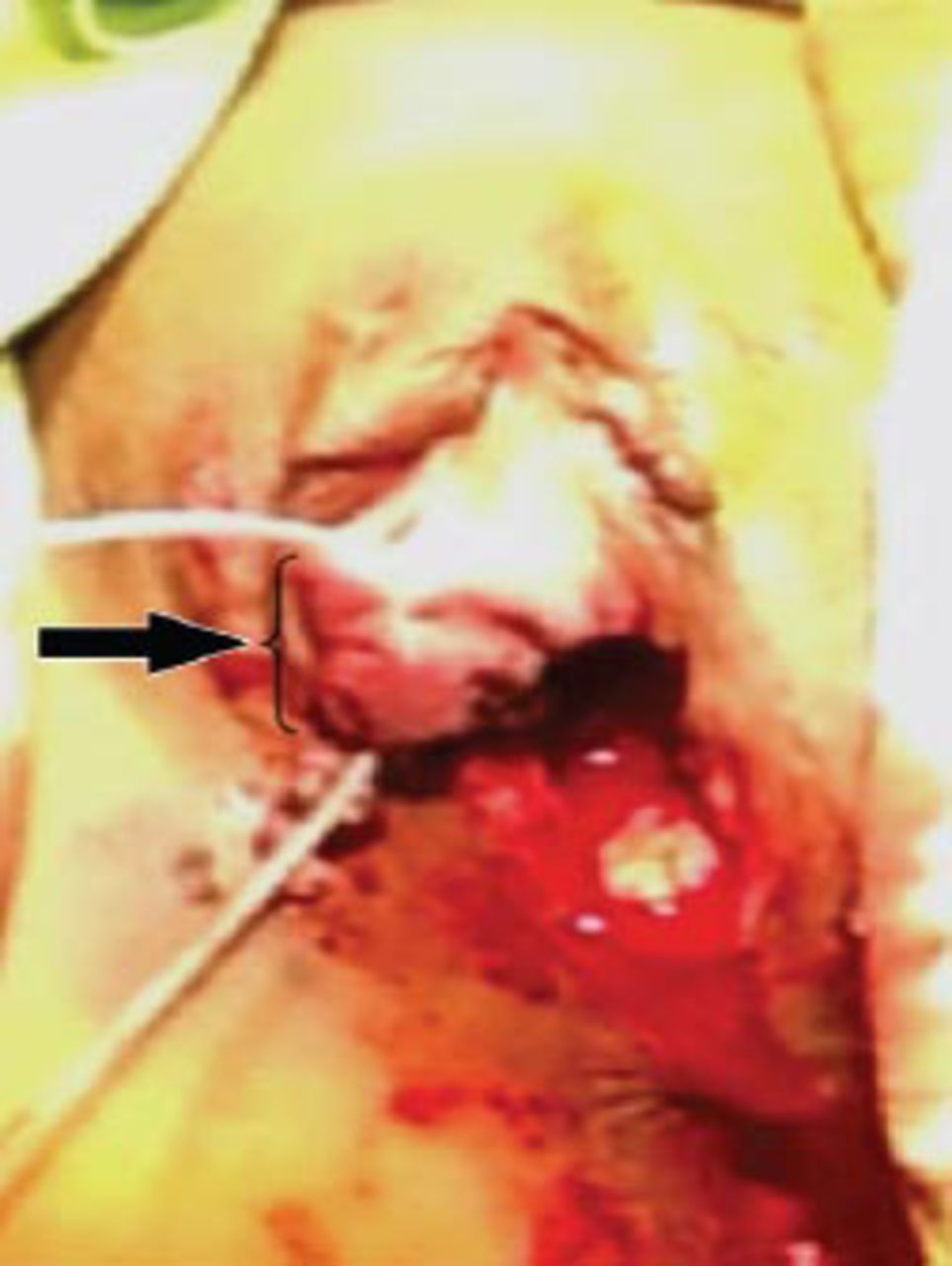
Severe laceration of the anterior vaginal wall with complete urethral avulsion; with the catheter passed through the avulsed distal segment.

Photograph of the A) end-to-end urethral anastomosis over stenting silicone catheter; and B) after final closure.

Urethral calibration after one year, with wide urethral lumen and very healthy vagina.
Discussion
Traumatic female urethral avulsion in the absence of a pelvic fracture is an exceedingly rare occurrence. On literature review, we found only 2 previously reported cases of urethral injury without pelvic fracture. The first, was a complete urethral and bladder neck disruption;1 while the second case was a longitudinal urethral tear with vaginal laceration.2 We report a case of pregnant female traumatic urethral avulsion without an associated pelvic fracture.
The management of female urethral injury is not well established, and most reported cases were associated with pelvic fracture. In some cases, management consisted of suprapubic cystostomy and deferred surgical reconstruction;3 while other authors favored primary repair over delayed repair whenever possible.1,2,4-6 Depending on the extent of urethral injury, repair may be performed vaginally, trans-abdominally, or combined.4 In our patient, the repair was accomplished transvaginally. Anatomically, the female urethra is embedded in to the anterior wall of the vagina. The urethra itself consists of 3 layers: 1) the mucous layer, which is continuous with the bladder epithelium; 2) the thin layer of spongy erectile tissue, which includes the plexus of veins and bundles of smooth muscle fibers located immediately below the mucous layer, with both taken together during end to end anastomosis; and, 3) the muscular layer, which is continuous with the muscular layer of the bladder and closed as a second layer over the anastomosis. In some reports, authors maintain the urethral catheter for 3 weeks,5 while others keep it for 6 weeks.2 In our patient, it was maintained for 4 weeks to allow proper healing and as a diversion for urine.
In conclusion, early recognition and proper management with primary urethral and vaginal repair can prevent the subsequent risk of morbidity.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received September 30, 2014.
- Accepted December 8, 2014.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.