


Abstract
This report describes a case of recurrent pseudosarcomatous myofibroblastic proliferation (PMP) of the bladder with a satisfactory clinical course after a 3.5-year follow-up. There is a lack of reports of successful treatment experiences on recurrent PMP of the bladder in adults. For the primary lesion, a transurethral resection of the bladder tumor (TUR-BT) was performed; for the recurrent lesion, a combination regime of TUR-BT and intravesical mitomycin C proved effective treatment. The patient did not suffer local recurrence or distal metastasis during the 3.5-year follow-up. Our experience may serve as treatment reference to urologists who encounter similar cases.
Inflammatory myofibroblastic tumor (IMT) and pseudosarcomatous myofibroblastic proliferation (PMP) of the bladder are rare entities that were first described by Roth in 1980.1 Recently, it is not clear if PMP is a “true tumor” or “benign proliferative mesenchymal lesion.” Although an overwhelming majority of reported PMP cases have been benign in nature, some researchers still consider that close surveillance is necessary owing to its histological similarity to some malignant tumors.2-5 Rosai6 found a non-random chromosomal translocation in chromosome 2p23, supporting the theory that PMPs are true neoplasms. In this study, we illustrated a locally recurrent PMP to support its clonal origin in a patient who underwent treatment with transurethral resection of the bladder tumor (TUR-BT) and chemotherapy with mitomycin C and presented a satisfactory clinical course during a 3.5-year follow-up.
Case Report
A 22-year-old male with severe anemia was transferred by ambulance to the Emergency Department at the West China Hospital, Chengdu, China. He had a 10-day history of painless gross hematuria with blood clots, which was associated with dizziness and facial pallor of onset a week prior to the initial visit. He initially visited a local hospital, but the prescribed drug therapy did not relieve his symptoms.
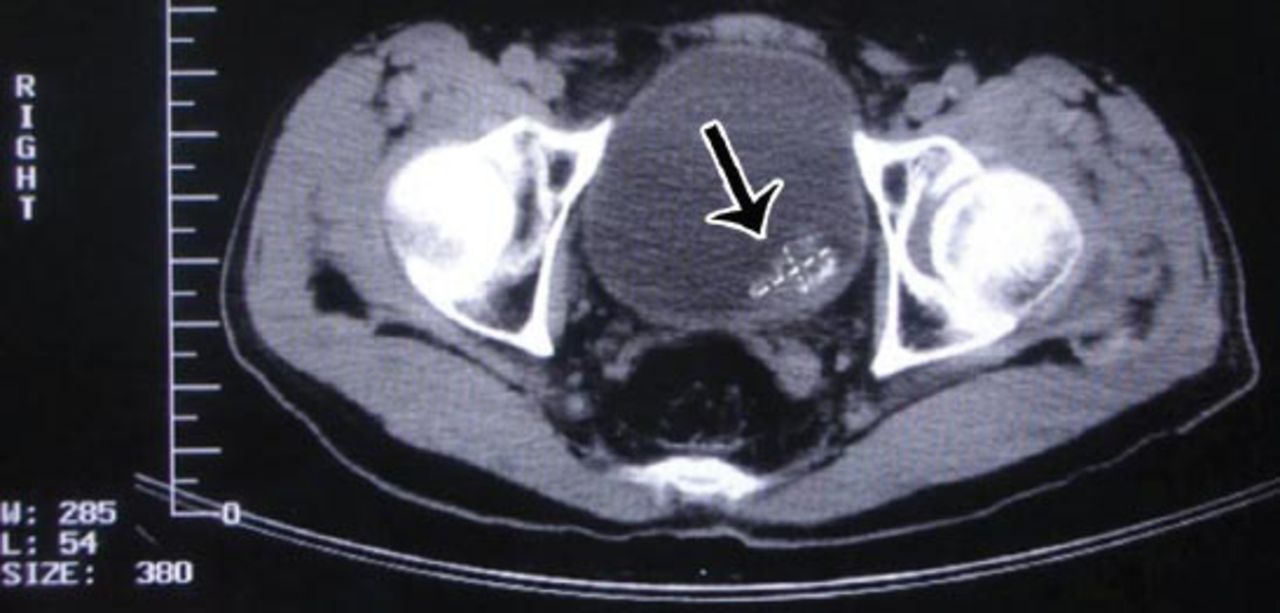
After admission, laboratory test results yielded a hemoglobin level of 42 g/L. Hemostasis, transfusion, and fluids were administered to achieve rehydration and increase hemoglobin levels as quickly as possible. An emergent CT scan was performed and reviewed. A 3.5 × 2.0-cm, slightly enhanced mass was observed, occupying parts of the left and superior walls of the bladder (Figure 1). Because of the diagnosis of bladder-occupying lesion with the suspicion of cancer, cystoscopy, and TUR-BT were performed. Cystoscopy demonstrated a necrotic tumor tissue and significant bleeding. During TUR-BT, we found that the tumor did not invade beyond the serosa of the bladder and that the trigone was not involved. The tumor tissue was transported to the Department of Pathology at the West China Hospital of Sichuan University for pathological diagnosis. The evaluation of the paraffin-embedded tissue indicated PMP, which was obtained one week after the patient was discharged from the hospital. Under microscopy, the field was filled with spindle myofibroblasts characterized by abundant eosinophilic cytoplasm and large nuclei (Figure 2). On immunohistochemical (IHC) evaluation, the cells were strongly positive for anaplastic lymphoma kinase-1 and vimentin, focally positive for epithelial membrane antigen, muscle-specific actin, and negative for smooth muscle actin, H-caldesmon, desmin, myogenin, human melanoma, black-45, and S-100.
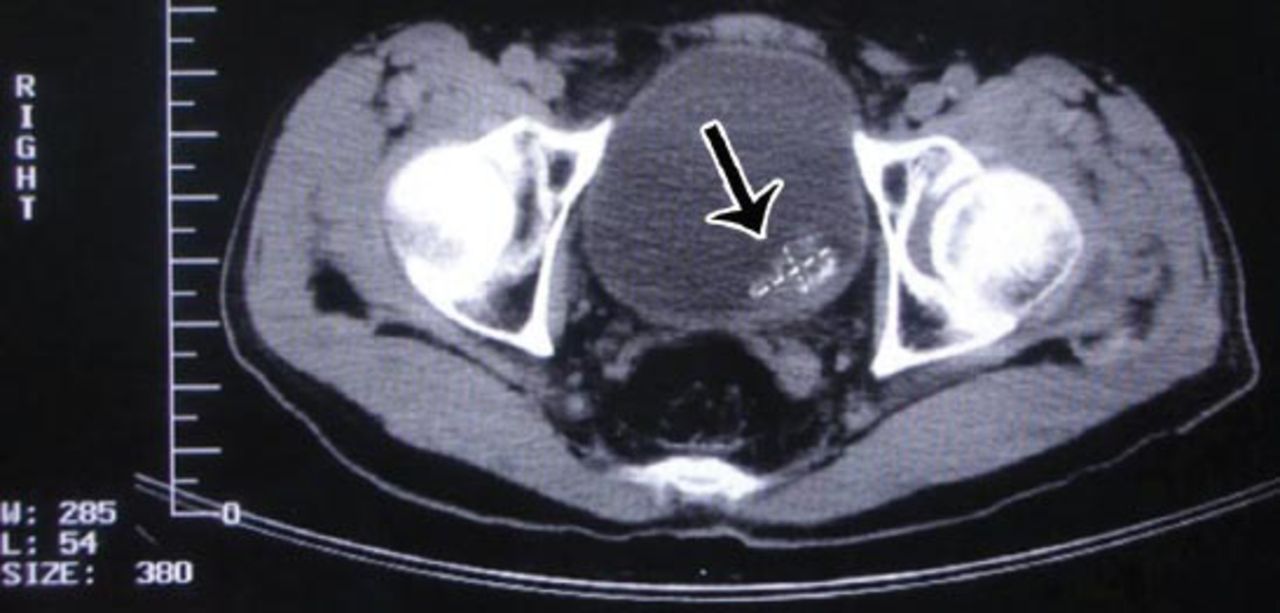
Computed tomography scan of the primary lesion with a size of 3.5× 2.0-cm, as indicated by the arrow. Perivesical invasion was not seen.
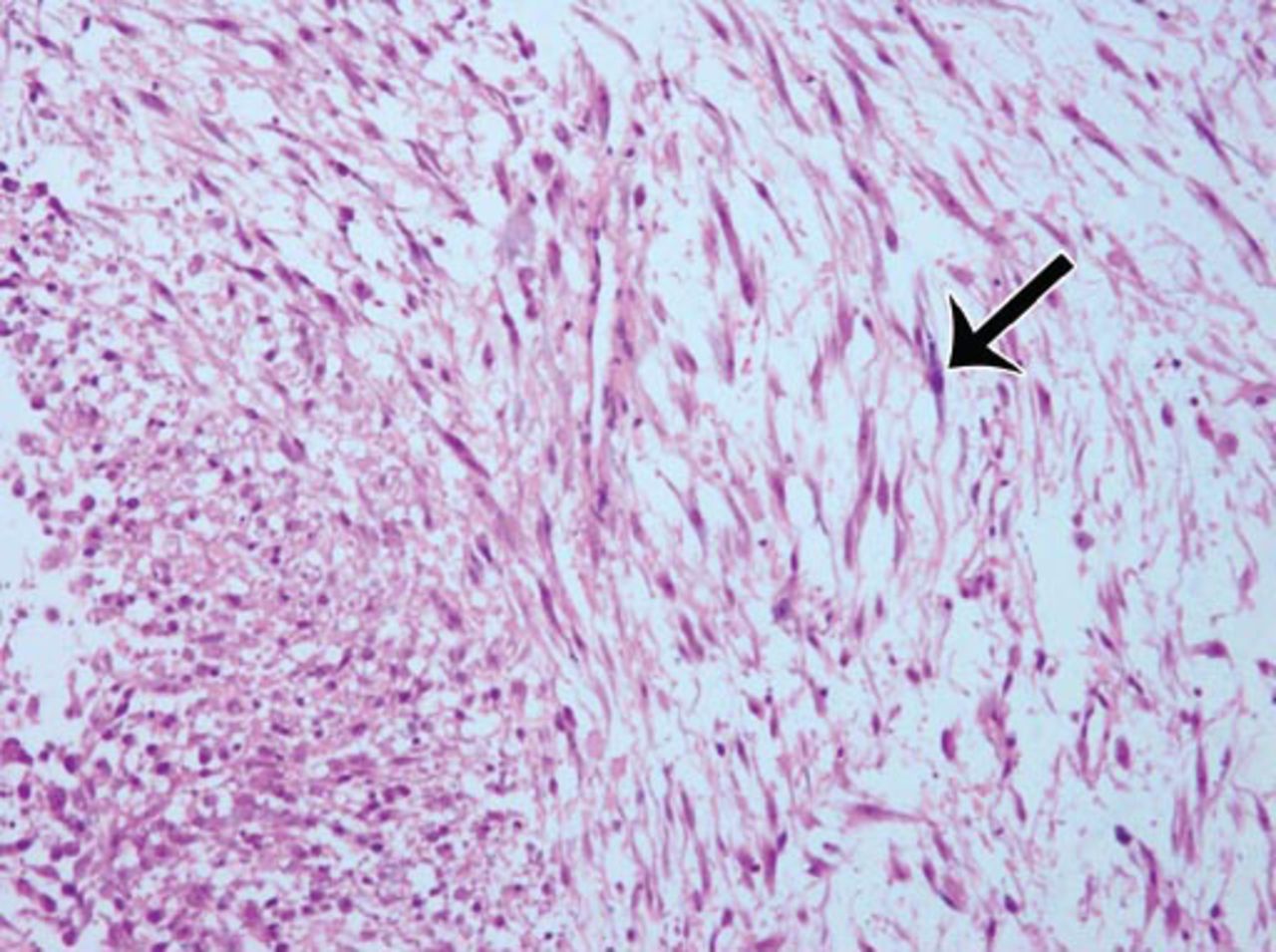
The histopathological examination revealed spindle or round myofibroblasts with red cytoplasm and large nuclei (as indicated by the black arrow); nucleoli were visible, with a certain degree of pleomorphism and mitotic figures. Cells are fascicular and staggered, with a background of interstitial edema and some inflammatory cells infiltration. Original magnification ×200.
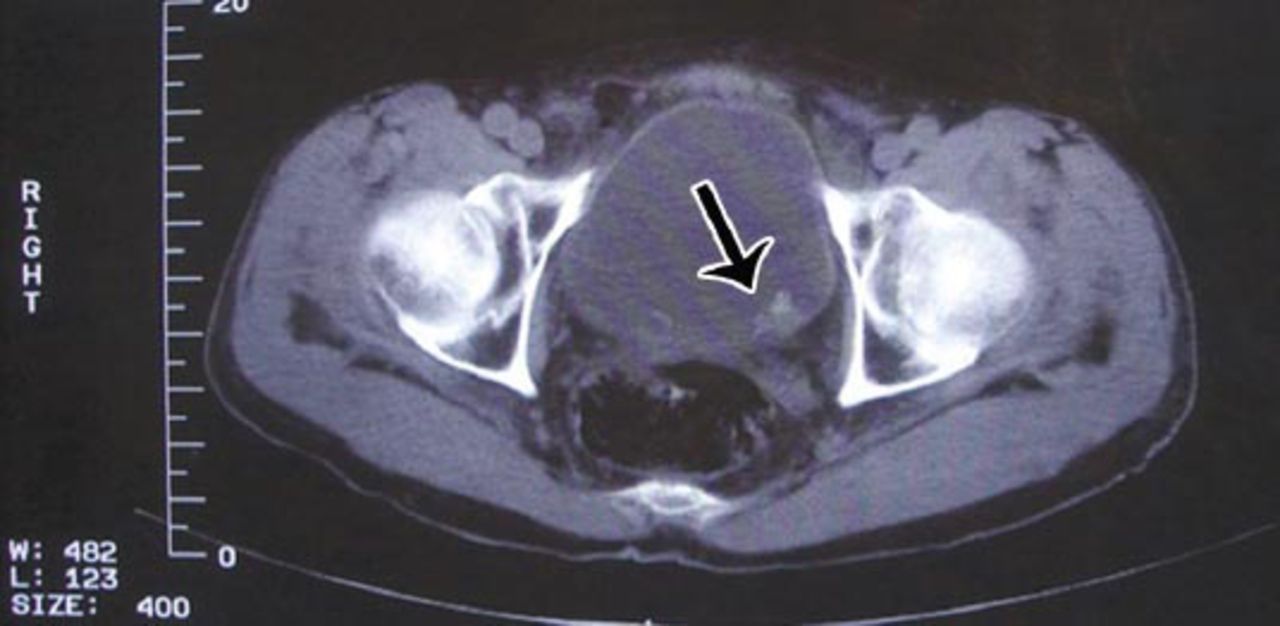
After 4 months, he returned to our institution, complaining of discomfort in the lower abdomen. The CT scan showed a new neoplasm of approximately 2.0 × 1.0-cm, adjacent to the location of the primary tumor that had been removed previously (Figure 3). A biopsy was performed, and the pathological and IHC result identical to the original nodule, confirming the recurrence of PMP. Considering his fear on reduced quality of life and neoplasm relapse, we performed TUR-BT followed by intravesical administration of mitomycin C (40-mg regimen). Intravesical instillations were repeated once a week for 6 weeks. Further, every 3 months during the first year postoperatively and every 6 months after that, he underwent reexamination by chest radiograph, abdominal CT scan, and ultrasound to detect any disease recurrence or metastasis. After a 3.5-year follow-up, we did not find any signs of local recurrence or distal metastasis, and his clinical course has been satisfactory.

Computed tomography scan of the recurrent lesion with a size of 2.0×1.0-cm, as indicated by the arrow. Perivesical invasion was not seen.
Discussion
Mesenchymal myofibroblastic spindle cell proliferation is a vast and heterogeneous category that includes PMP and other entities, varying from indolent lesions to highly aggressive tumors. Genitourinary tract involvement by PMP is an extremely rare occurrence, and the most commonly occurring location is the bladder. Since 1980 to date, several designations have been proposed to describe the entities encompassed under the category of myofibroblastic proliferations of the bladder, and yet, this issue remains debatable. The terms PMP and IMT may be more frequently used than others; that is fibromyxoid pseudotumor and plasma cell granuloma. According to the World Health Organization, IMT has been defined as a low grade malignancy tumor that typically occurs in children.7 However, the relationship between PMP and IMT, and whether PMP is a post-inflammatory process, or a true neoplasm as is IMT is still subject to controversy. Very few studies have reported cases of PMP, compared with those of IMT, with a ratio of 1:8. Harik et al8 reported a rather large case series that included 42 cases of PMP, and they reported that some lesions developed spontaneously while others were secondary to instrumentation, surgery, or drugs. Herein, we reported a case of locally recurrent PMP. We did not find any evidence of urinary infection, and the patient had no history of operation or trauma; thus, our findings further support the clonal origin of PMP. Therefore, we suppose that the 2 designations, IMT and PMP, actually refer to the same entity.
Establishing a preoperative diagnosis of PMP is challenging as there are no specific clinical manifestations. Moreover, imaging examination techniques, such as CT and MRI, and cystoscopic findings are usually difficult to distinguish from malignant tumors. Therefore, the diagnosis of PMP often depends on the postoperative pathological examinations. In this case, the combination of the patient’s painless hematuria and the appearance of the lesion under cystoscopy suggested that the lesion may comprise a malignant bladder cancer, until the pathological results were obtained. The positive results of ALK-1 for the present case were consistent with those case reported in previous studies.9,10 Thus, ALK-1 is important because of its differential diagnosis with the lesions of spindle cell neoplasms, such as rhabdomyosarcoma and myxoid leiomyosarcoma, because the latter 2 are negative for ALK-1.11
Although the clonal origin of PMP is still unclear, most of the available data highlight its benign and indolent clinical course, and conservative treatment is selected in most cases. Alquati et al2 found that 65% of the reported cases were treated with TUR-BT and 27% with partial cystectomy. In the present case, we selected TUR-BT for the management of the primary and recurrent lesions. Furthermore, the bladder was washed with mitomycin C to prevent lesion recurrence, although previous researchers believed that aggressive management was unnecessary. Considering its benign pathology, the absence of recurrence on follow-up may be related to the natural history of the disease instead of to the use of mitomycin C. The follow-up result showed a satisfactory clinical course. We did not find any reports of management experiences referring to recurrent PMP lesions; thus, our case may serve as a treatment reference for urologists who encounter similar cases. It is noteworthy that the serosa of the bladder and the trigone area were not involved by either the primary or recurrent lesions. Therefore, a closer follow-up regime may be required for cases of lesions beyond the serosa and multiple, or large lesions.
In conclusion, we present a successful treatment experience for a rare case of bladder PMP with local recurrence in a young male. As most PMPs are generally benign and do not metastasize, upon recurrence, an aggressive management may be considered with close follow-up.
Acknowledgment
We would like to express our gratitude to Prof. Jiang for preparing and reviewing the figures.
Footnotes
Disclosure. This study was supported by the project of Natural Science Foundation of China (NSFC) (Project Number: 81370855; 81270841). Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received August 28, 2014.
- Accepted December 1, 2014.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.