


Abstract
Objectives: To determine the effect of thrombectomy on platelet function in patients undergoing primary percutaneous coronary intervention (PPCI) for ST segment elevation myocardial infarction (STEMI).
Methods: This retrospective study included 413 consecutive STEMI patients who underwent PPCI between March 2012 and September 2013 at Kartal Kosuyolu High Specialty Education and Research Hospital, Istanbul, Turkey that were assigned to the thrombus aspiration (TA) group or the non-TA group. Platelet count and mean platelet volume (MPV) were obtained at baseline and 24 hours (h), 48 h, and 72 h post PPCI.
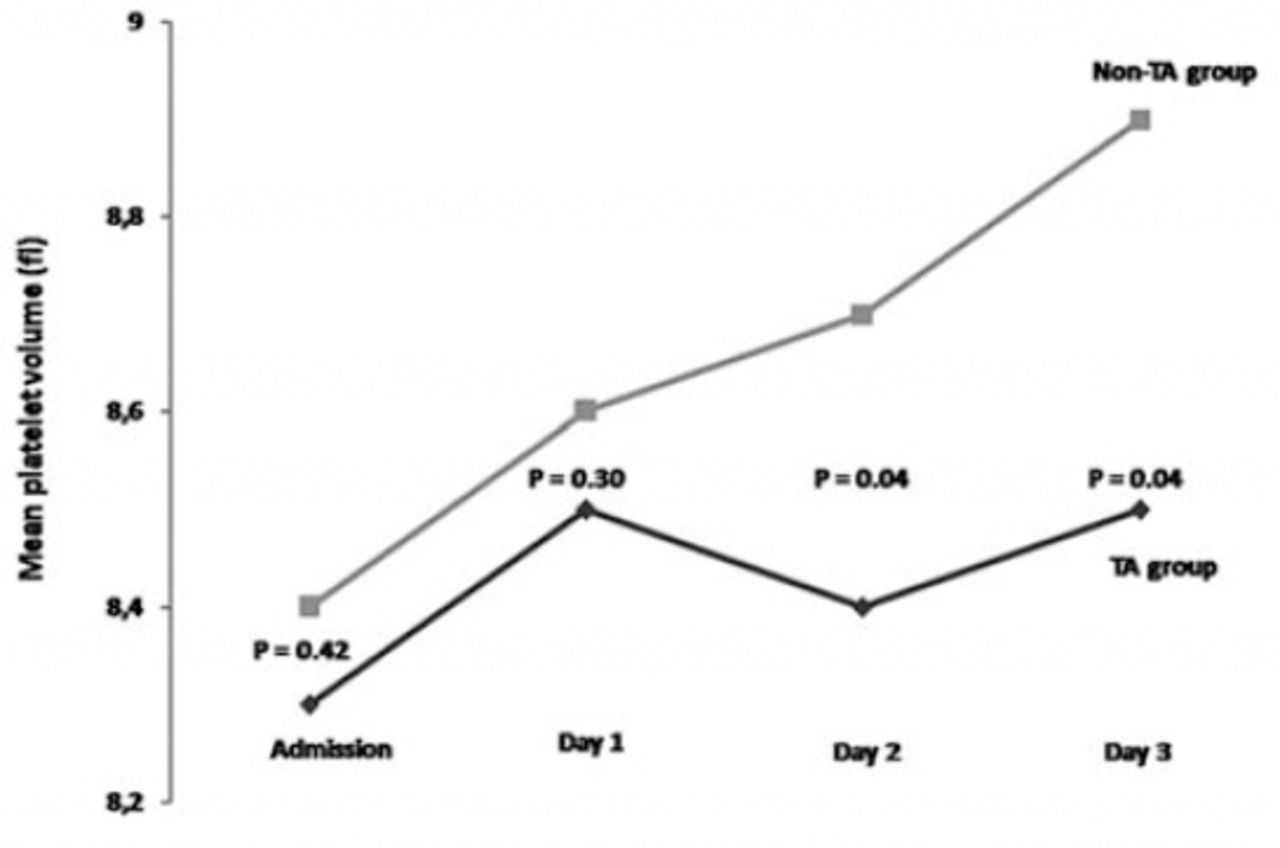
Results: Baseline MPV was similar in both groups, whereas the baseline platelet count was higher in the TA group (p=0.42 and p=0.002). The platelet count was higher in the TA group 24 h post PPCI (p=0.02), but was similar in both groups 48 h and 72 h post PPCI (p=0.18 and p=0.07). The MPV 48 h and 72 h post PPCI was higher in the non-TA group than in the TA group (8.4 ± 1.3 fL versus 8.7 ± 1.6 fL [p=0.04] and 8.5 ± 1.1 fL versus 8.9 ± 1.5 fL [p=0.04]).
Conclusion: Thrombectomy reduced platelet activity via removal of thrombi from the coronary arteries in patients undergoing PPCI for STEMI.
In acute ST-segment elevation myocardial infarction (STEMI), the main initiating factor is atherosclerotic plaque rupture or erosion, then platelets become activated and aggregated leading to acute coronary artery occlusion.1 Primary percutaneous coronary intervention (PPCI) is the standard treatment in patients with STEMI.2 In recent years, implementation of adjunctive mechanical and pharmacological therapies during PPCI, including manual thrombus aspiration (TA), has improved myocardial reperfusion and clinical outcome in STEMI patients.3-5 In daily practice, thrombectomy devices are used to remove thrombi or to prevent embolization of thrombi and plaque during PPCI.6 Platelet volume is a marker of platelet activation and is measured via mean platelet volume (MPV).7 An increase in MPV can occur in cases of acute myocardial ischemia, acute myocardial infarction, coronary atherosclerosis,8,9 and early stent thrombosis (ST).10 The Percutaneous Coronary Intervention in Acute Myocardial Infarction (TAPAS) study5 showed that TA therapy during PPCI decreases mortality and reinfarction rate.5 We speculate that the good results obtained with TA therapy are not only related to improved tissue perfusion but also may be related to reduced platelet activation. Therefore, the present study aimed to determine the effect of thrombectomy on platelet function and ST in patients undergoing PPCI for STEMI.
Methods
This retrospective study included 413 consecutive STEMI patients who underwent PPCI between March 2012 and September 2013 at Kartal Kosuyolu High Specialty Education and Research Hospital, Istanbul, Turkey, and were assigned to the thrombus aspiration (TA) group or the non-TA group. The institutional Ethics Committee approved the study, and consent was obtained from all patients for participation in the study and collection of detailed clinical data. The study complies with the principles outlined in the Declaration of Helsinki.
The STEMI was defined according to the European Society of Cardiology 2012 guidelines.2 Patients that were admitted to the hospital within 12 hours (h) of the onset of acute STEMI were included in the study. All patients had total occlusion of the infarct-related artery, with thrombolysis in myocardial infarction (TIMI) flow grade 0 or one based on coronary angiography prior to PPCI and angiographic evidence of intraluminal thrombus in the infarct-related artery. Exclusion criteria included hemodynamic instability, defined as systolic blood pressure <90 mm Hg, use of inotropic agents or an intra-aortic balloon pump, significant arrhythmias, significant renal dysfunction (estimated glomerular filtration rate <30 mL min–1), moderate to severe valvular heart disease or heart failure, any clinical evidence of active infection or cancer, hematoproliferative disorders, inflammatory or autoimmune diseases, steroid therapy, thyroid dysfunction, history of percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG), stent thrombosis, need for emergency CABG, and history of alcohol consumption of 40 g week–1. Additionally, patients whose complete blood count or medical records were unavailable, and those that did not achieve TIMI flow grade 2/3 following PPCI were excluded from the study. In total, 413 patients with STEMI were included in the study; the TA group included 219 patients that underwent TA and the non-TA group included 194 patients that did not undergo TA. All patients were pretreated prior to revascularization with aspirin 300 mg and clopidogrel 600 mg. Anticoagulant (intravenous unfractionated heparin) and optional glycoprotein IIb/IIIa inhibitor were used according to operator discretion. After diagnostic coronary angiography, a guiding catheter was inserted into the infarct-related artery. The lesion was passed with the guide wire. The TA was performed using a Diver CE (Invatec, Brescia, Italy), according to operator discretion. A Diver CE (Invatec, Brescia, Italy) is a rapid-exchange 6-F compatible TA catheter, with a central aspiration lumen (0.6604 mm) and a soft, flexible non-traumatic tip with multiple holes that communicate with the central lumen; aspiration is performed by connecting a 20-mL syringe to the aspiration catheter. Aspiration was started proximal to the occluded site, gently advancing the catheter through the occlusion, and then pulling it in a proximal direction, maintaining negative pressure even when the occlusion was crossed. Withdrawal of the catheter from the artery and from the guiding catheter was performed with constant negative pressure. Aspiration was terminated when successful aspiration was followed by aspiration without any debris, or when 7 aspiration attempts did not show any visible material. Additional pre dilatation or post dilatation with a balloon and stent implantation were used at the discretion of the operator. Intracoronary nitroglycerine was administered periprocedurally based on operator discretion. Standard therapy post PPCI included aspirin, clopidogrel, beta-blockers, lipid-lowering agents, and angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers, according to current society guidelines.2
Blood samples for biochemical analysis were collected from an antecubital vein. Complete blood count, including hemoglobin, platelet (PLT) count, MPV, and white blood cell count, and differential counts were obtained at baseline (within one h of admission), and 24 h, 48 h, and 72 h post PPCI. Blood samples were collected into standard tubes containing dipotassium Ethylenediaminetetraacetic acid (EDTA) and processed at room temperature. The time between blood collection at admission and analysis was <45 min. The PLT count and MPV were determined via the Coulter counter technique (Coulter Gen. S Hematology Analyzer, Beckman Coulter Corp, Hialeah, FL, USA).
Statistical methods
Statistical analysis was performed using the Statistical Package for Social Sciences statistical software (SPSS version 17 for Windows; SPSS Inc., Chicago, IL, USA). Parametric variables are shown as mean ± SD, and categorical variables as absolute number and percentage (given in brackets %). The level of statistical significance was set at p<0.05. Parametric variables were compared between groups using the independent samples t-test. Comparison of the frequency of categorical variables between groups was performed using the x2 test.
Results
This study included 413 patients (347 male and 66 female) with a mean age of 56.3 ± 11.3 years that underwent PPCI. In all, 50.3% of the patients had multi-vessel disease. Patient demographic and clinical characteristics are summarized in Table 1, which were similar in both groups, except for the baseline PLT count. The interventional and angiographic characteristics of the 2 groups are summarized in Table 2. The balloon predilatation was significantly higher in non-TA group. The in-hospital stent thrombosis rate was lower in the TA group than in the non-TA group; however, baseline MPV was similar in both groups, but the baseline PLT count was higher in the TA group than in the non-TA group (Table 3). The PLT count was higher in the TA group 24 h post PPCI, but was similar in both groups 48 h and 72 h post PPCI (Figure 1). Although MPV 24 h post PPCI did not differ significantly between the 2 groups, it was higher in the non-TA group 48 h and 72 h post PPCI (Figure 2).
Baseline characteristics of 413 patients underwent percutaneous coronary intervention (PPCI).
Angiographic and periprocedural findings among 413 patients underwent percutaneous coronary intervention (PPCI).
Hematological values among 413 patients underwent percutaneous coronary intervention (PPCI).
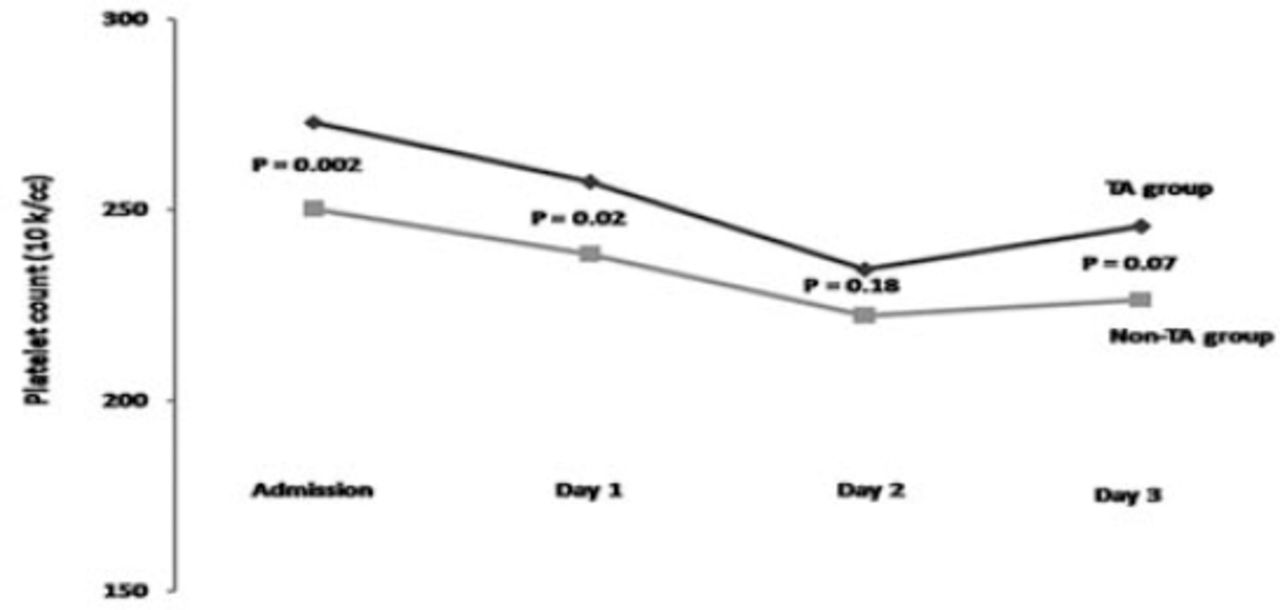
Platelet counts in groups among 413 patients underwent percutaneous coronary intervention (PPCI).
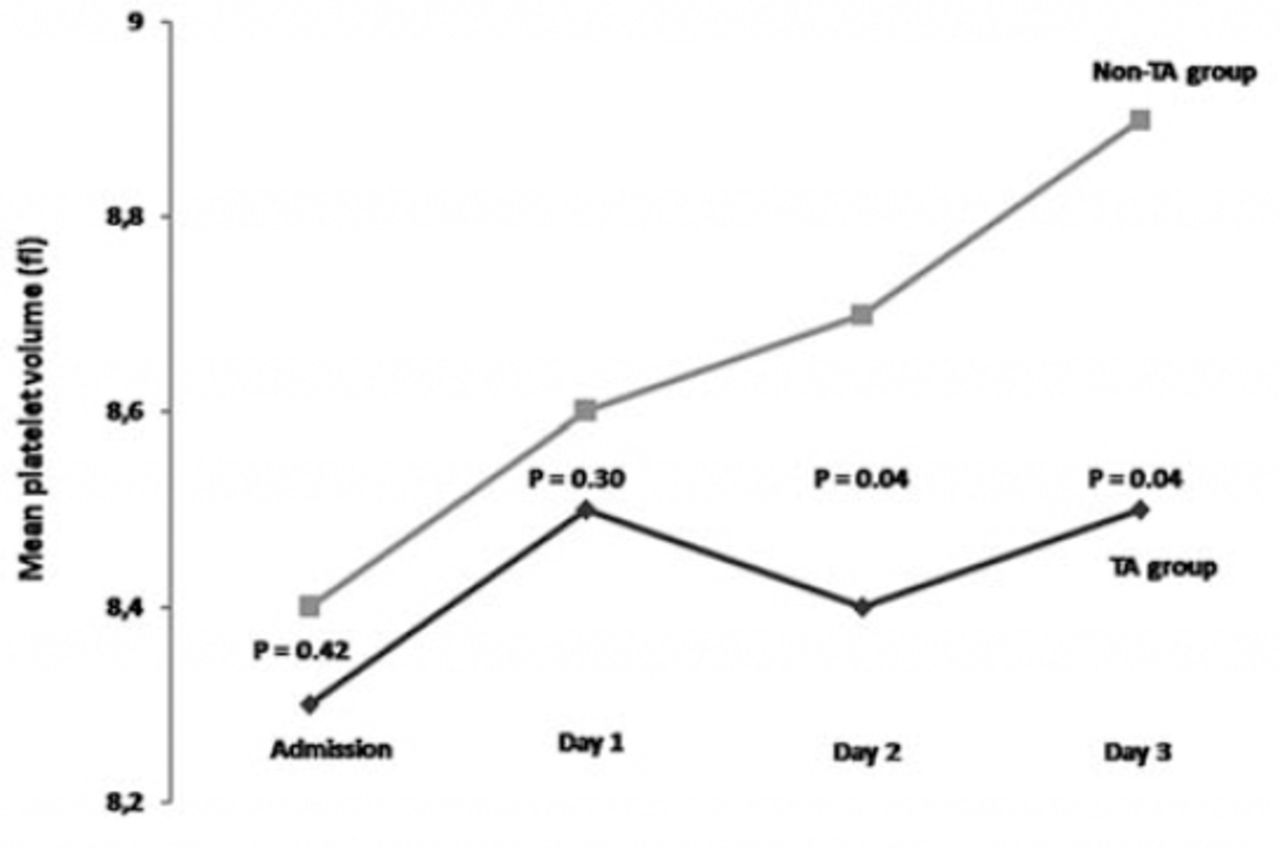
Mean platelet volumes in groups among 413 patients underwent percutaneous coronary intervention (PPCI).
Discussion
The present study’s findings show that the MPV levels significantly increased to a greater degree post PPCI in the non-TA group than in the TA group. Also, the in-hospital stent thrombosis rate was lower in the TA group than in the non-TA group. Therefore, we hypothesize that thrombectomy during PPCI for the correction of coronary perfusion might reduce platelet activity and in-hospital stent thrombosis. Platelet volume is a marker of platelet function and activation,7 and is measured as MPV using clinical hematology analyzers. Larger platelets have higher granule content and higher thromboxane A2 levels, and express more glycoprotein Ib and IIb/IIIa receptors.11 Consequently, large platelets are more reactive than small platelets and produce more prothrombotic factors.12 An increase in MPV may play a role in the development of coronary atherosclerotic disease,8,9 but MPV varies according to the pathophysiology of coronary artery disease. Angiographically visible distal embolization is related to reduced myocardial reperfusion, more extensive myocardial damage, and poor prognosis.13 Reducing the thrombus burden by mechanically removing it from the infarct-related artery might improve myocardial reperfusion and clinical outcome. The TAPAS study5 reported that TA resulted in improved myocardial reperfusion, and one-year clinical outcome post PPCI as compared with conventional PPCI. In our study, balloon predilation, and usage of stent were lower in the TA group. Accordingly, TA prevents the unnecessary use of material. This approach may be associated with lower cost. Additionally, thrombectomy reduces thrombus burden and residual thrombus, threrefore increase the minimal lumen diameter of the coronary artery. Our findings support this view that stent diameter was bigger in the TA group. Stent implantation after thrombectomy during PPCI allows for a larger-diameter stent to be used and may help reduce stent thrombosis and restenosis rates. Although many studies3,4 reported that manual TA improves myocardial perfusion and clinical outcome, no study has investigated the effect on platelet activation; therefore, we hypothesized that manual TA prior to stenting in patients with STEMI would reduce platelet activation. According to the present findings, baseline MPV was similar in the TA and non-TA groups, but 48 h and 72 h post PPCI it was lower in the TA group. In addition, the baseline PLT count were higher in the TA group, but was similar in both groups 48 h post PPCI, which indicates that platelet activation was lower in the TA group 48 h post PPCI. Multiple pathways contribute to platelet activation; adenosine diphosphate, thromboxane A2, serotonin, epinephrine, collagen, and thrombin are important platelet activators.14-16 Thrombin is the most potent platelet activator and can activate platelets at very low concentrations.16 Thrombin binds protease-activated receptor (PAR)-1 and PAR-4 on the platelet surface, and activates the receptors.17 The TA therapy removes thrombi from coronary arteries, and decreases the likelihood of distal embolization during subsequent angioplasty and stent deployment.18 We hypothesized that decreasing thrombin via thrombus aspiration reduces platelet activation. Moreover, the in-hospital stent thrombosis rate in the present study was approximately 3-fold lower in the TA group than in the non-TA group. Huczek et al10 reported that baseline platelet size is greater in acute coronary syndrome patients developing early ST following PCI. They reported that there is a positive correlation between baseline platelet size and future response to dual antiplatelet therapy; MPV was the lowest in good responders to dual antiplatelet therapy, moderate in poor responders to either drug, and highest in dual poor responders. The lower in-hospital stent thrombosis rate observed in the present study’s TA group may have been related to less increase in platelet activation and good response to dual antiplatelet therapy.
Study limitations
This single center and moderate size study has several limitations. Firstly, intravascular ultrasound was not routinely used, and therefore the possible influence of inadequate stent expansion or stent malposition not observed angiographically on the incidence of ST cannot be excluded. Secondly, TA use was left to operator discretion, which could have led to a selection bias that may have impacted outcomes. Also, we did not obtain the surrogate markers of platelet activity.
In conclusion, manual thrombectomy added to PPCI may reduce platelet activation, which can reduce the incidence of in-hospital ST in patients with STEMI. Large prospective studies are needed to confirm our findings.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received March 10, 2015.
- Accepted June 22, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.