


Abstract
The treatment of deep anterior crossbite is technically challenging due to the difficulty of placing traditional brackets with fixed appliances. This case report represents a none traditional treatment modality to treat deep anterior crossbite in an adult pseudo class III malocclusion complicated by severely retruded, supraerupted upper and lower incisors. Treatment was carried out in 2 phases. Phase I treatment was performed by removable appliance “modified Hawley appliance with inverted labial bow,” some modifications were carried out to it to suit the presented case. Positive overbite and overjet was accomplished in one month, in this phase with minimal forces exerted on the lower incisors. Whereas, phase II treatment was performed with fixed appliances (braces) to align teeth and have proper over bite and overjet and to close posterior open bite, this phase was accomplished within 11 month.
Anterior forward displacement of the mandible due to interferences causes anterior cross bite, which is a characteristics of pseudo-Class III and true skeletal Class III malocclusions.1,2 The differences between true skeletal Class III and pseudo-Class III malocclusion lies in both skeletal and dent-alveolar components. In the skeletal component, the true skeletal Class III malocclusion patient has deficient maxilla, protruded mandible, or both producing a true skeletal Class III malocclusion. However, in pseudo-Class III malocclusion, the patient has normal maxilla and mandible sizes and have skeletal Class I malocclusion.3 In the dento-alveolar component, usually the true skeletal Class III patient has dental compensation due to protruded maxillary incisors and retruded mandibular incisors. In pseudo-Class III malocclusion, the upper incisors are retroclined with normal or protruded lower incisors. To differentiate between true skeletal Class III and pseudo-Class III malocclusions, a proper diagnosis of each case has to be performed because both malocclusions clinically have anterior crossbite.4 Correct pseudo-Class III malocclusion diagnosis makes a huge difference in the type of orthodontic treatment plan. Diagnosis is performed clinically by guiding the patients into centric relation, if the incisors show an edge-to-edge relationship with posterior open bite and for the posterior teeth to occlude in centric occlusion, a forward functional mandibular shift is created causing incisors to occlude in anterior crossbite, this indicates that the patient has pseudo-Class III malocclusion. However, this diagnosis should be supported by radiographic analysis, as the patient with pseudo-Class III malocclusion have skeletal Class I relationship with normal maxilla and mandible sizes.5 Anterior crossbite has been associated with a variety of complications, such as gingival recession of the lower incisors, incisal wear, and eventually losing these teeth. Skeletally, this malocclusion worsens the growth pattern to develop into true skeletal Class III malocclusion.6 In orthodontic treatment, it is known that the correction of anterior crossbite can be carried out by fixed, or removable appliances.7 However, the therapeutic use of the inverted labial bow incorporated in a removable appliance to open the bite and correct the anterior crossbite was rarely used. In the literature, this appliance was first introduced by Wang in 19968 after that only few reported cases used it successfully.9,10 The presented study offers a way to deal with pseudo Class III malocclusion complicated by reverse deep bite with retruded supraerupted both upper and lower incisors. The inverted labial bow in the appliance described by Wang in 19968 was used; however, modifications were made to open the reverse deep bite and to correct the anterior crossbite without exerting any force on the retruded lower incisors. The aim of this study is to introduce a simple appliance that can treat a pseudo Class III malocclusion in an adult patient complicated by a reverse deep bite with retruded supraerupted of both upper and lower incisors.
Case Report
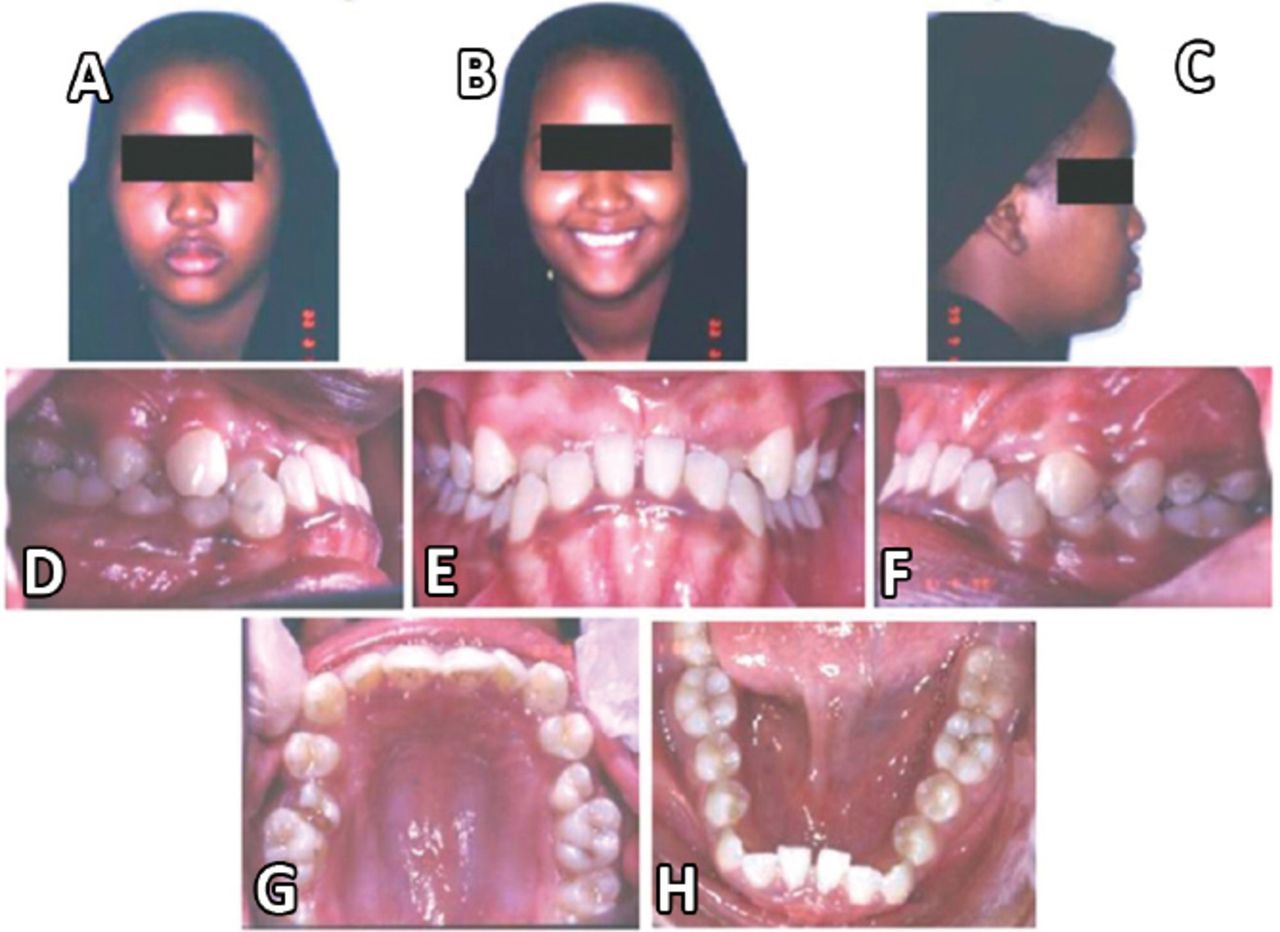
A 16-year-old female patient, complains of the appearance of her anterior teeth (abnormal anterior deep crossbite resembling monkey’s bite), with both upper and lower incisors being severely retruded and supraerupted. She was diagnosed with pseudo Class III malocclusion; the incisors are in an edge-to-edge relationship, but due to incisal interference between the upper and the lower incisors, an anterior functional mandibular shift was created and the teeth fall in deep anterior crossbite as she closes in centric occlusion. Skeletally, she was Class I; hence, this confirms the pseudo Class III malocclusion diagnosis (Figure 1A-1H).
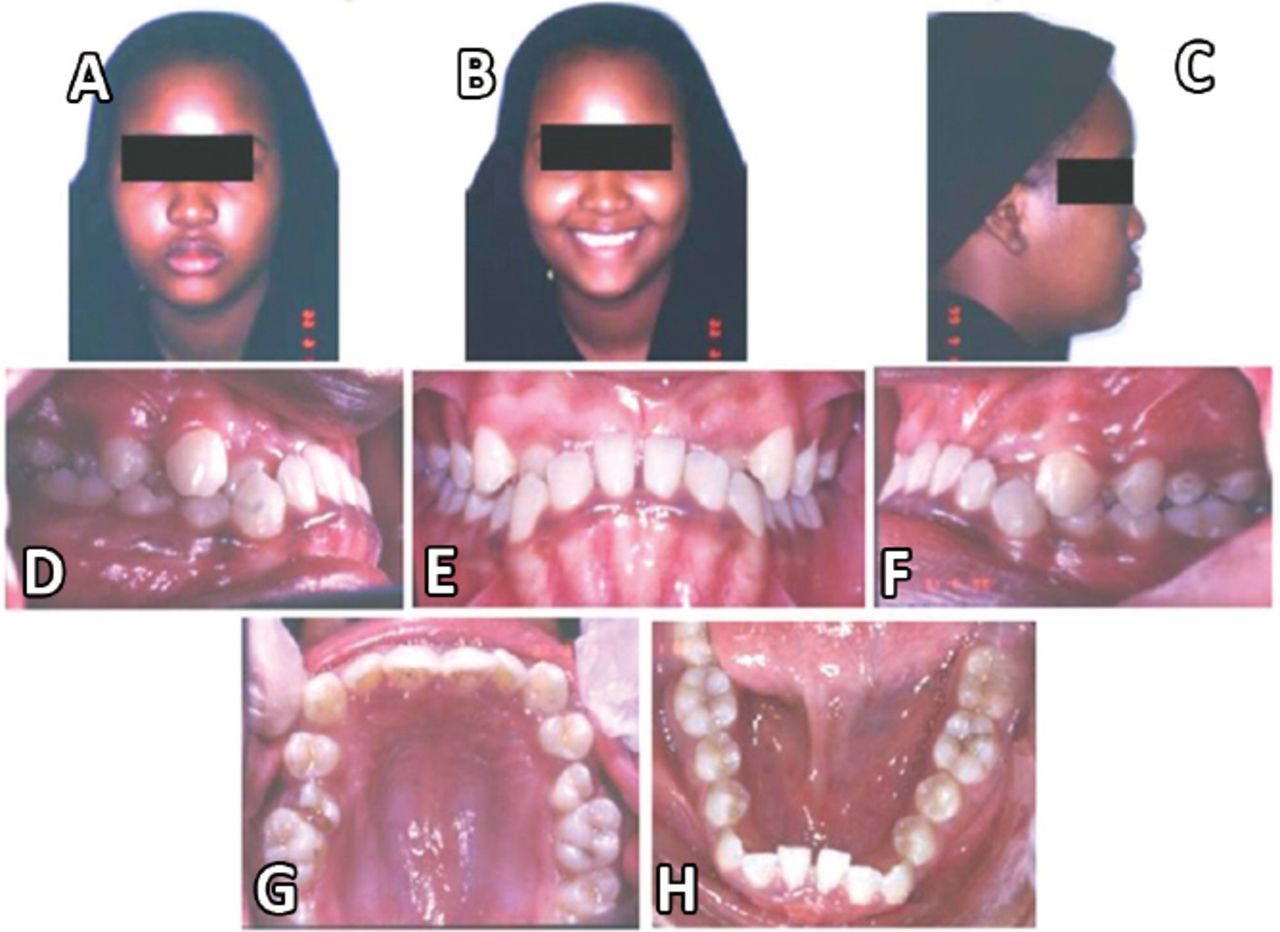
Pre-treatment extra-oral photos (A-C) and intra-oral photos (D-H) showing the patient chief complain (unpleasant monkey bite).
Appliance design
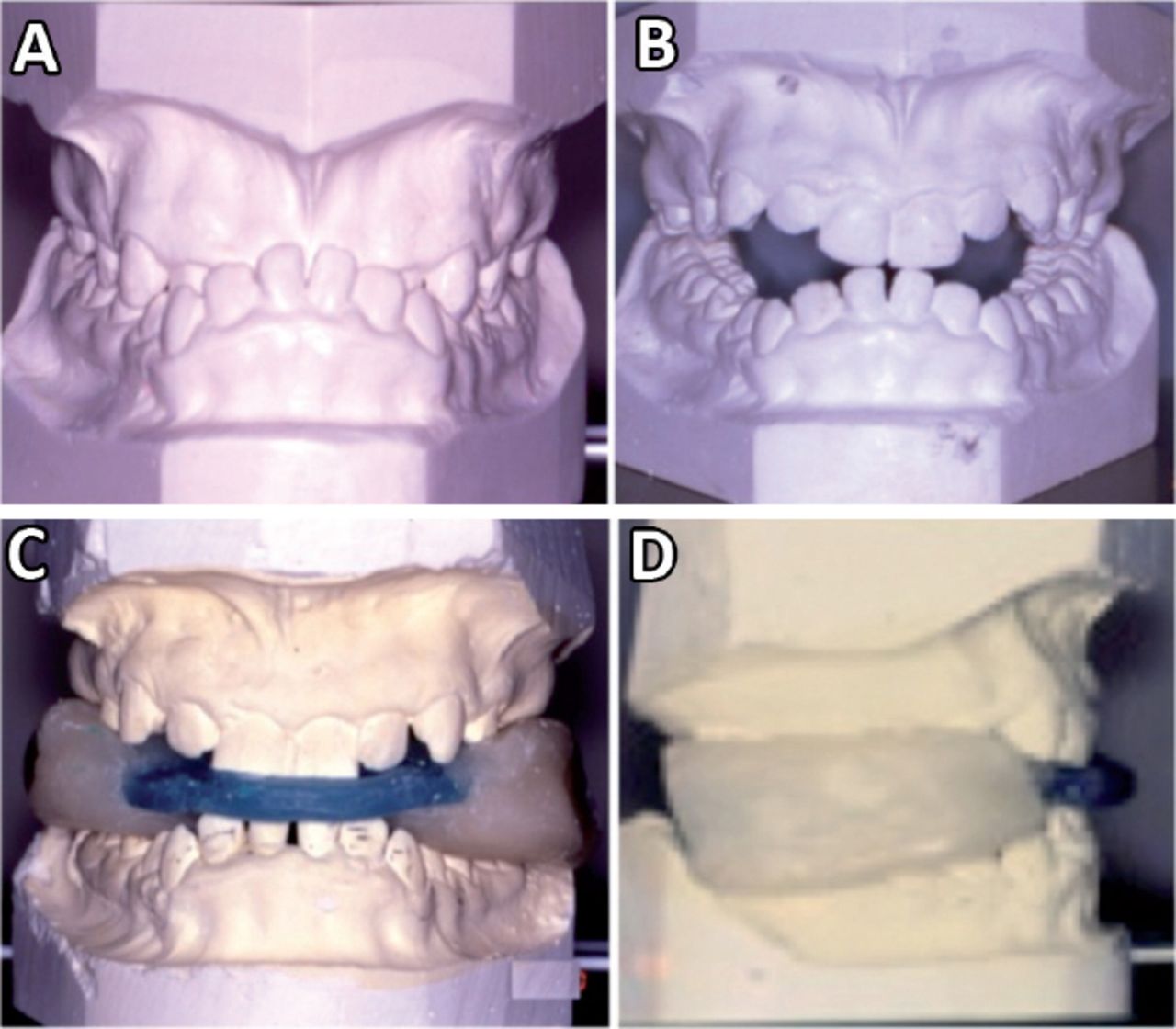
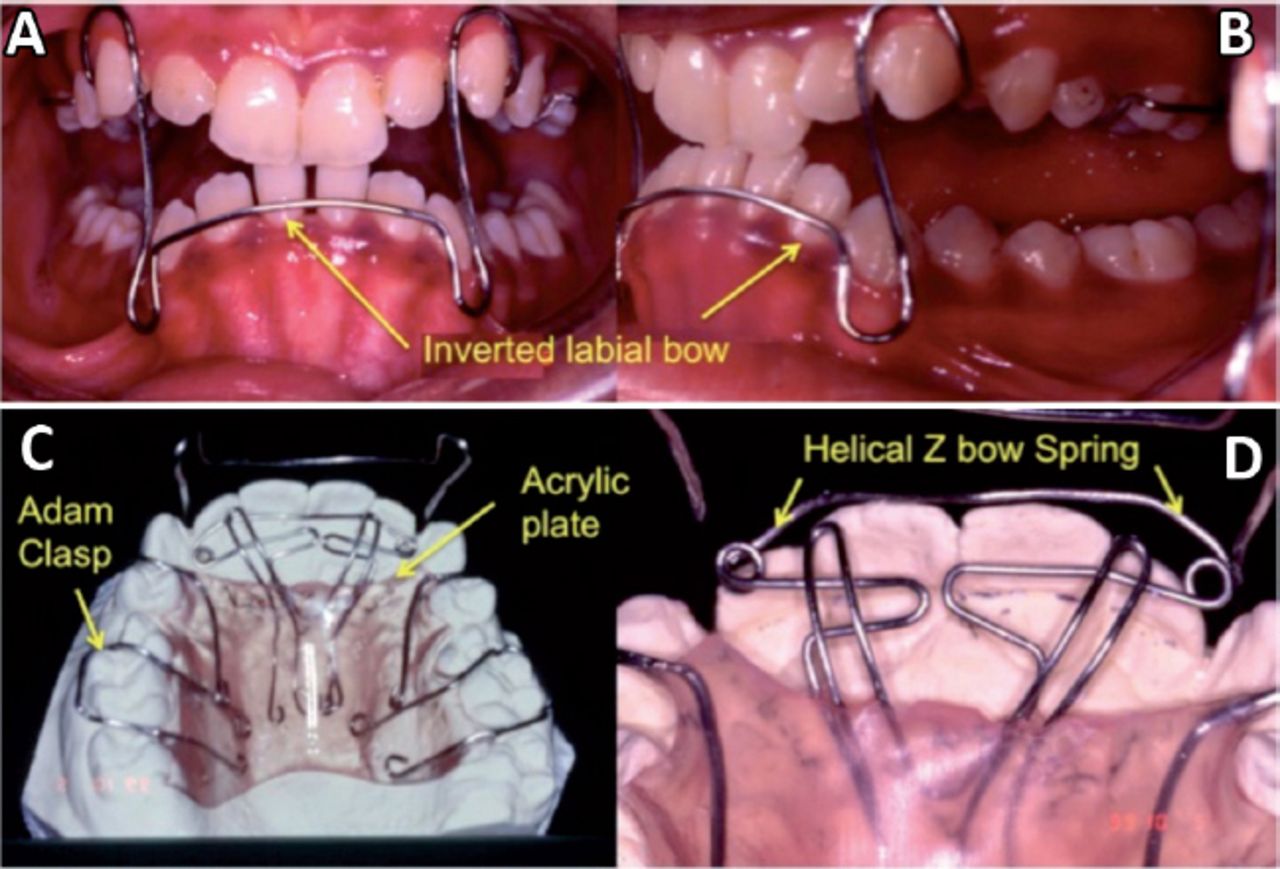
In order to construct the removable appliance “Hawley appliance with inverted labial bow,” the bite registration was taken for the patient in centric relation; this was carried out by guiding the mandible posteriorly in an edge-to-edge incisor relationship. The bite was then transferred to the working model articulated in a hinge articulator (Figure 2A-2D). Construction of inverted labial bow was performed on the lower arch and 2 Adams clasps on upper first molars, and these represents the retentive components of this removable appliance, whereas, the active component was the helical Z bow spring fabricated behind the upper incisors and they are supported by a horizontal wire extensions and all these components were attached to the palatal acrylic plate, which was cut intentionally away from the upper anterior teeth (Figure 3A-3D).
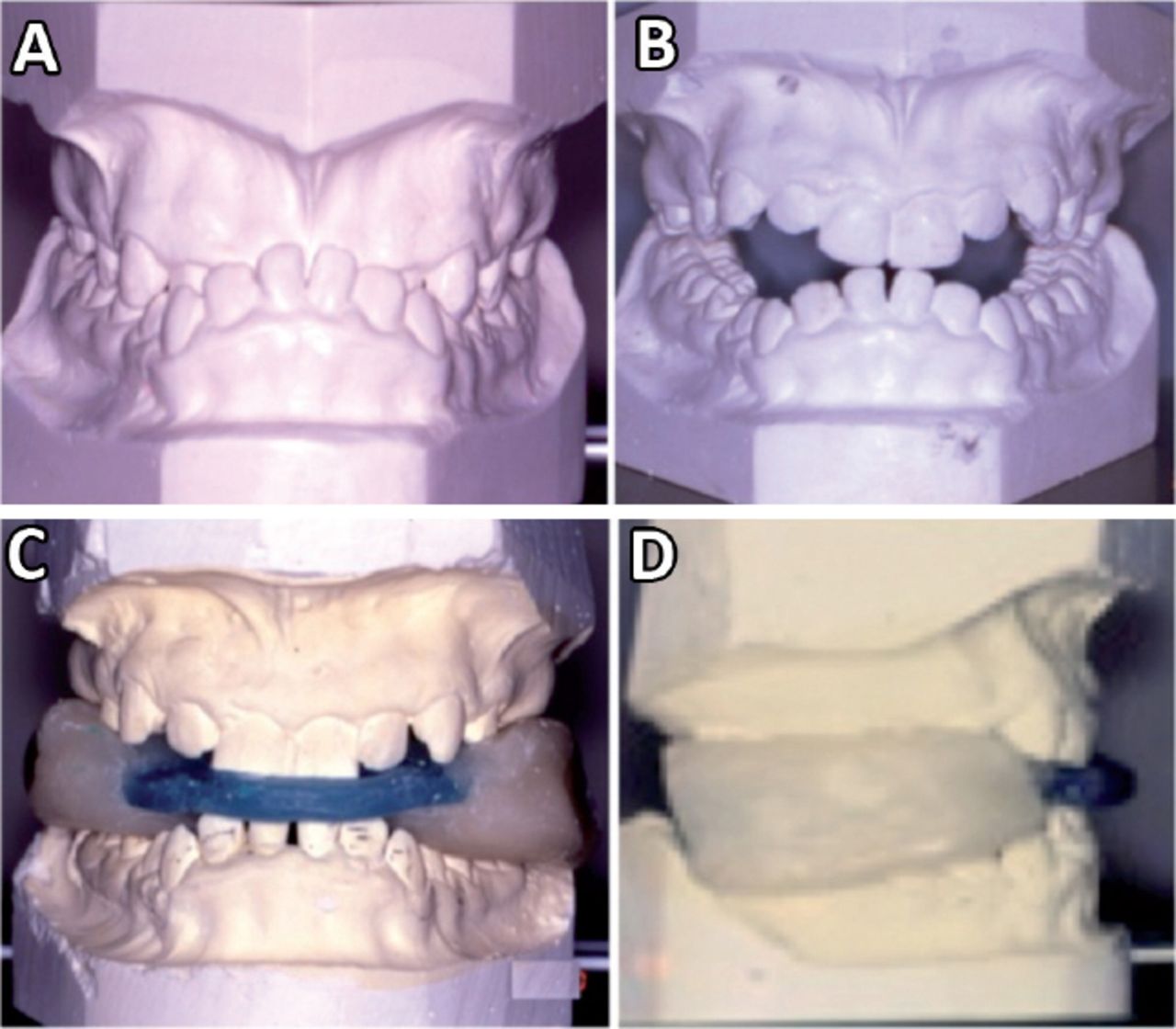
Frontal views of the patient cast in: A) centric occlusion, B) centric relation, and C - frontal view and D - side view) the bite registration of the mounted patient’s cast in centric rrelation.

Intra-oral photos (frontal and side views) after insertion of the appliance showing: A & B) the inverted labial bow, and C & D) upper view of the patient cast with the appliance showing 2 Adams clasps and helical “Z” bow spring.
Treatment progress
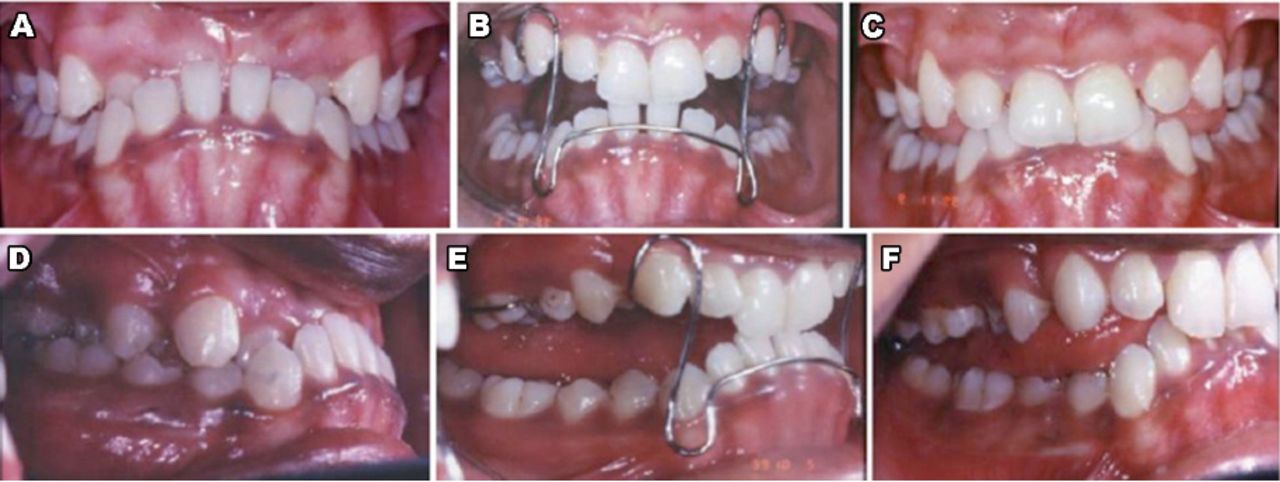
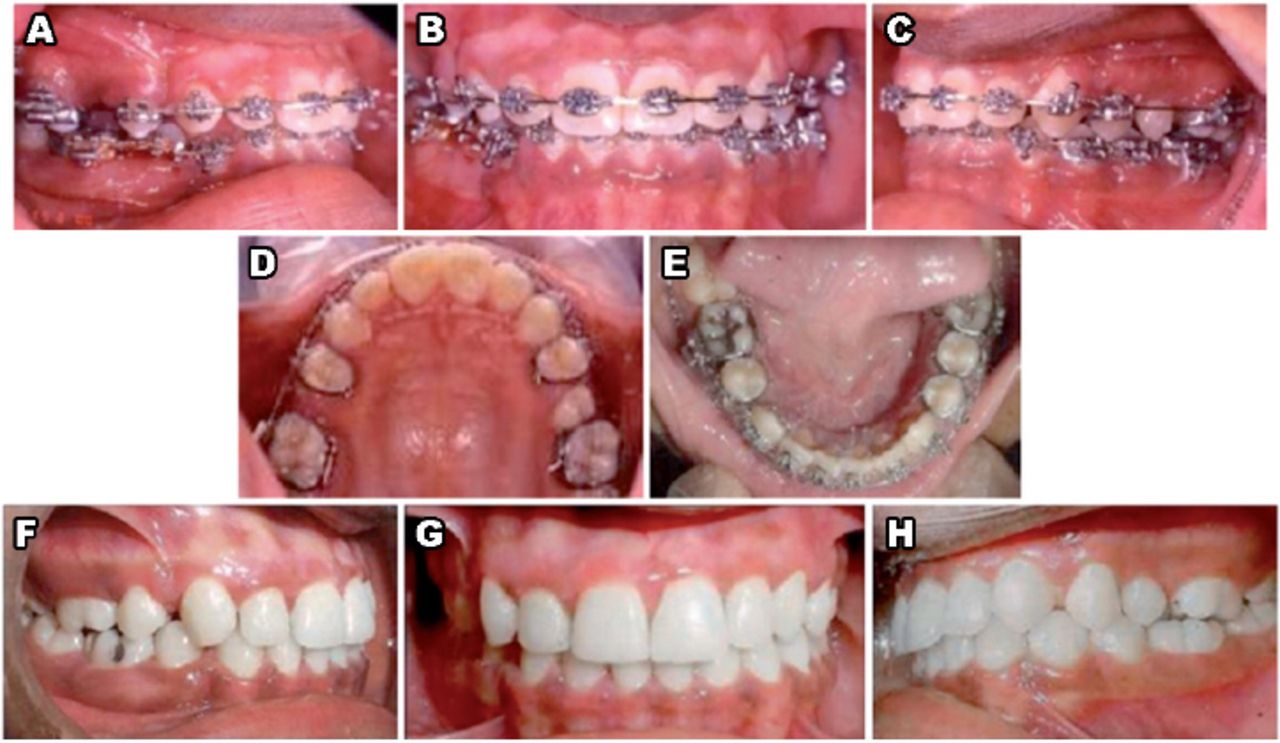
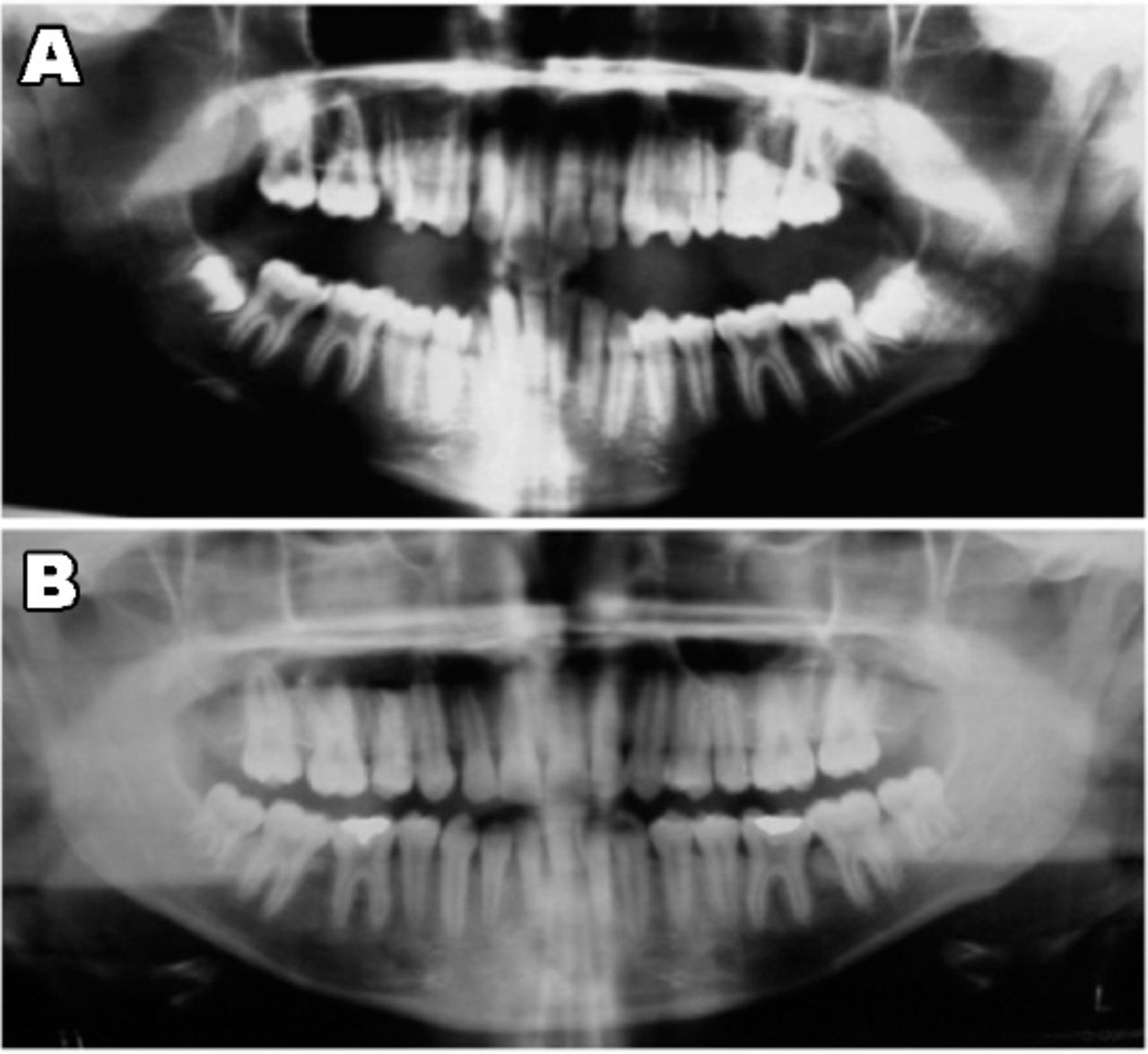
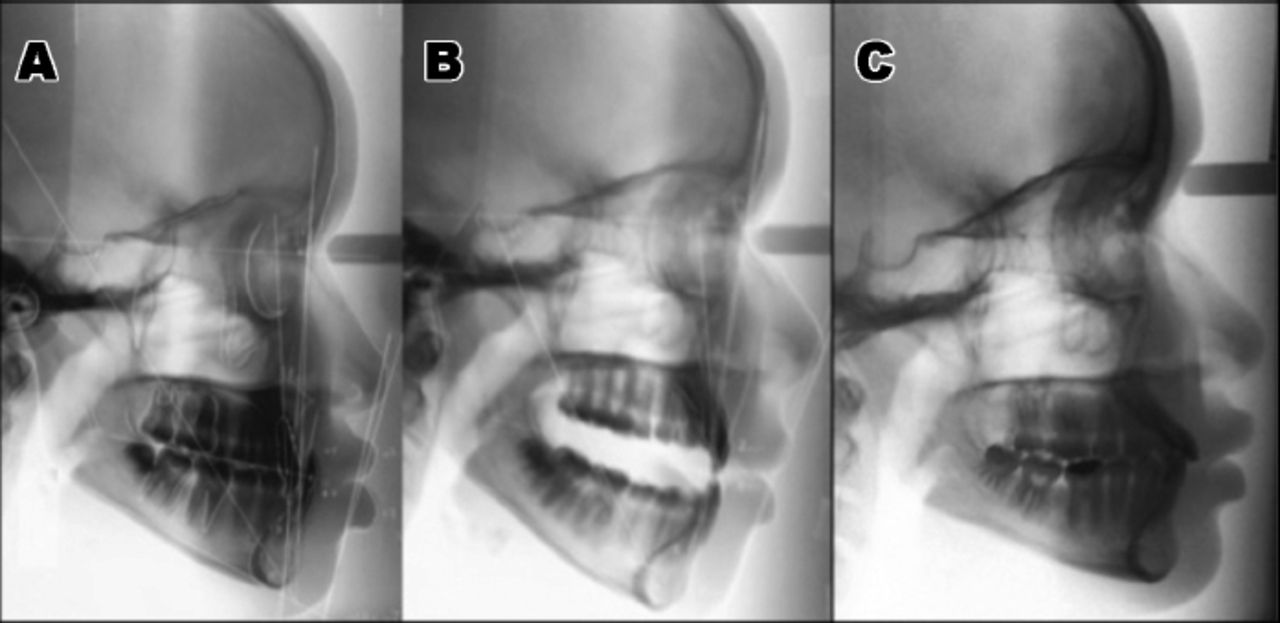
Treatment of this case was carried out in 2 phases. In phase I treatment, the removable appliance with the inverted labial bow was used. The objective of this phase was to create a positive overbite and overjet and this was accomplished in one month. At the beginning, to test if the appliance was fabricated correctly, it was fitted passively in the mouth. This was performed by fitting the Adams clasps in the upper part of the appliance on the upper first molars and the acrylic plate on the palate with the helical Z bow spring passively lying behind the upper incisors, then her mandible was guided to bite in centric relation (edge to edge relation) placing the lower anterior teeth into the inverted labial bow in the lower arch. After making sure that the appliance was fitted correctly, it was then taken from patient’s mouth and 2 modifications were carried out before re-inserting it back. The first modification was expanding the labial bow by opening slightly the U shape of the inverted labial bow to fit it loosely on the lower incisors and the second modification was activating the helical Z bow spring by opening slightly the helixes of the spring to push the upper incisors forward out of crossbite. She was trained on wearing and removing the appliance several times, and instructions were given to her to use it all the time including nighttime. It will be removed only during eating and brushing. This was continued for 3 weeks. A follow-up appointment was made after 3 weeks of wearing the appliance, it was noticed that she was able to close in centric occlusion with positive overbite and overjet with no anterior forward shift. For retention, she was asked again to re-use the appliance at bedtime for another week and then the appliance was discontinued (Figure A4-4F). In phase II treatment, fixed appliances (braces) were placed to align teeth and to have proper overbite and overjet, which was accomplished in 11 months (Figure 5A-5H). She had a very small size upper right and left second premolars; however, the upper right second premolar had undermined deep carious lesion that was extended to the roots, and it was hopeless to treat; thus, it was extracted before orthodontic treatment. The decision was made to mesialize the upper right first and second molar into its place. Asymmetrical extraction was also carried out in the lower right arch because even after having positive overbite, she still has Class III canine relationship on the right side and Class I canine relation on the left side. Thus, it was decided to extract the lower right first premolar during orthodontic treatment to correct the right side canine relationship and help to flatten the curve of Spee. Panoramic views of the case pre and post phase II treatment is shown in Figure 6A & 6B. Lateral cephalometric radiographs of the pre-treatment in centric occlusion, the pre-treatment in centric relation, and the post-treatment are shown in Figure 7A & 7C. The lateral cephalometric analysis of the pre-treatment measurements in centric occlusion (Pre-CO), the pre-treatment measurements in centric relation (Pre-CR), and the post-treatment (POST) measurements were compared with the mean cephalometric measurements in a normal adult of black ethnic race7 were shown in Table 1. Post-treatment measurements were almost normalized compared with the mean. Overall comparison of pre, progree, post-treatment extra-oral photographs were shown in Figure 8, and intra-oral views were al gathered in Figure 9.

Intra-oral photos (frontal and side views) showing: A & D) pre-treatment, B & E) progress-treatment phase I after the insertion of the removable appliance, and C & F) post-treatment.
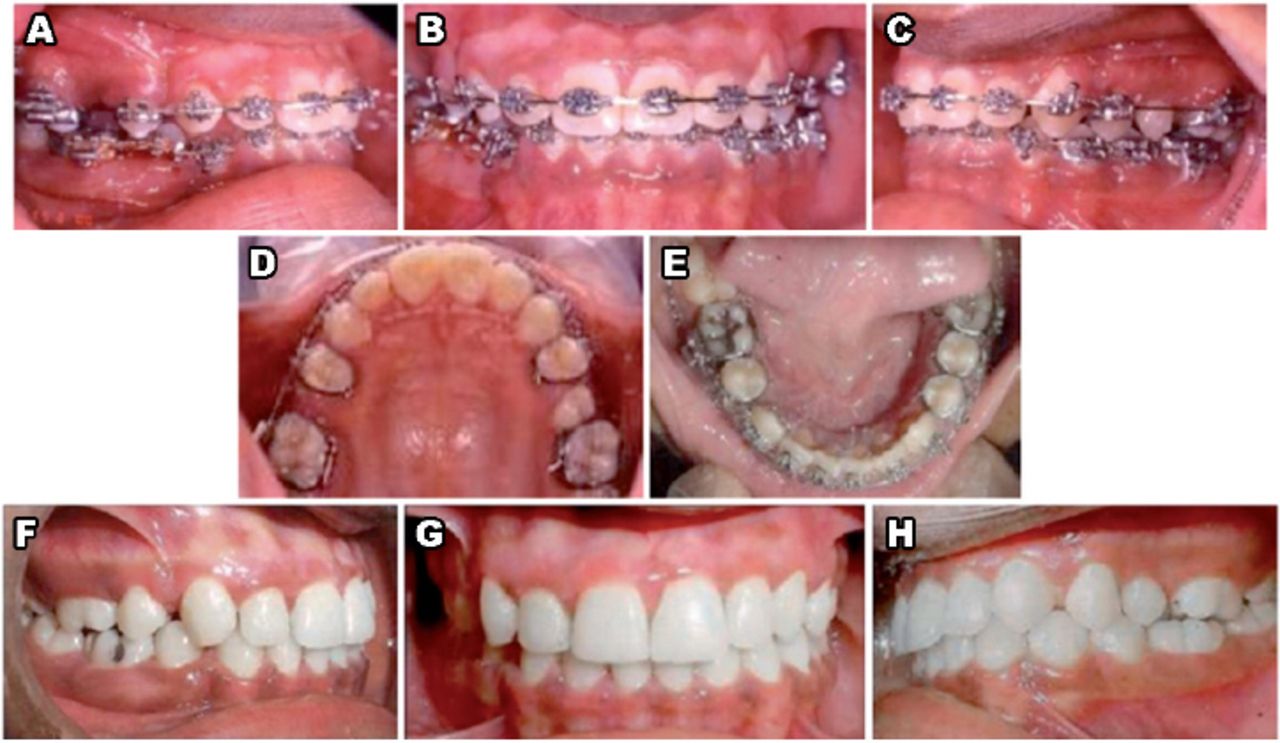
Intra-oral photos (frontal and side views) of phase II progress-treatment photos with fixed appliances “Braces” (A-E), and post-treatment photos (F-H).

Panoramic radiographs of the case in: A) pre-treatment, and B) post-treatment.

Cephalometric radiographs of the pre-treatment in: A) centric occlusion, B) the pre-treatment in centric relation, and C) the post-treatment.
Cephalometric measurements of the pre-treatment in centric occlusion (Pre CO) and the pre-treatment in centric relation (Pre CR) and the post-treatment (POST).

Extra-oral photographs comparing the pre-treatment, progress-treatment phase I, and post-treatment. Improvements were seen in frontal, smiling, and profile views.

Intra-oral photographs comparing the pre-treatment, progress of (phase I & phase II)-treatment, and post-treatment. Improvements were seen in frontal and side views.
Discussion
Previous study reported that treatment of a pseudo-Class III malocclusion must be performed as soon as it is detected to prevent dental and skeletal consequences.6-8 In the literature,2,5,6,8-10 several different appliances were suggested for correction of dental anterior cross-bite, they are either fixed or removable appliances. The most popular appliances were 2X4 fixed appliances in mixed dentition or full upper fixed appliances in adults with the use of expanded upper arch wire, or using removable appliance with Z helical spring or jackscrew behind upper incisors. The idea of all these appliances was to push or protrude the upper incisors labially.7,8 In Wang,8 Albarakati,9 and Negi and Sharma’s10 studies, all used a removable appliance with the inverted labial bow similar to the appliance used in this study. However, the idea of the inverted labial bow in their studies was to exert a lingually directed force on the lower anterior teeth by activating the inverted labial bow. This produced a reciprocal labial force on the upper incisors through the palatal spring incorporated in the acrylic of inverted Hawley appliances. They used their appliances on young growing patient in mixed dentition stage approximately 9 to 10 years with the lower incisors that normally positioned.8,10 Whereas, in this study the patient adult and the lower incisors were already retruded, and using the same appliance without making any modification could cause damaging effect. However, some modifications were made during fabrication and insertion of the appliance used in this case, and these modifications were made so as to exert minimal or no lingual forces on lower incisors. This was performed by expanding inverted labial bow to prevent direct lingual effect to the lower retruded incisor and cutting the acrylic away from all upper anterior teeth to prevent any reciprocal push forces transmittede to the lower incisors through the inverted labia bow after activation of the helical Z bow spring behind the upper incisors. Thus, the inverted labial bow was totally passive and it was only used for opening the bite. For retention and to guide the mandible in centric relation. However, the force to push upper incisors labially came only from the activation of the helical Z bow spring incorporated in this removable appliance. In the presented study, it was impossible to place fixed brackets on the upper anterior teeth to protrude them due to the presence of the reverse deep bite and the supraerupted, retruded lower incisors. However, opening the bite by placing posterior bite plane would produce intrusion effect on the upper and lower posterior teeth because the bite would open beyond the normal rest space limits (the free way space), thus, this intrusion effect would worsen the case since the cause of the excessive deep bite in this case is due to the supraerupted, retruded both upper and lower anterior teeth and not by the extruded posterior teeth. Thus, using this appliance creats a positive overbite quickly and efficiently.
In conclusion, deep anterior crossbite of pseudo Class-III malocclusion was successfully treated using none traditional treatment modality (removable appliance with inverted labial bow and helical Z-bow spring) followed by fixed appliance therapy. The presented removable appliance with its modifications was proven to be the cheapest and simplest appliance to correct anterior crossbite in pseudo Class-III malocclusion with deep bite as compared with other appliances.
Saudi Medical Journal Online features
* Instructions to Authors
* Uniform Requirements
* STARD
* Free access to the Journal’s Current issue
* Future Contents
* Advertising and Subscription Information
All Subscribers have access to full text articles in HTML and
PDF format. Abstracts and Editorials are available to all
Online Guests free of charge.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received October 21, 2015.
- Accepted February 22, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.