


Abstract
We aimed to present a case of symmetrical Wallerian degeneration (WD) in the middle cerebellar peduncles (MCPs) after a unilateral paramedian pontine infarction, which was examined by multimodality magnetic resonance imaging (MRI). In addition, we summarize the small number of reported cases. In our clinic, we observed a case of symmetrical WD of bilateral MCPs that occurred 6 months after the onset of a pontine infarction. We searched the Wanfang (Chinese) and PubMed databases and found 23 reported cases of this condition with characteristic similar to our patient. From the 24 cases, the detection time of WD ranged from 3 to 33 weeks. Symmetrical WD in the bilateral MCPs can occur after unilateral paramedian pontine infarction. Most cases were in Stages 2 and 3 of the disease and showed good clinical prognoses.
Wallerian degeneration (WD), a progressive process that occurs in both the central nervous system (CNS) and peripheral nervous system (PNS), involves the degeneration of an axon distal to a site of injury or transection. The pathological process of WD begins with rapid axonal disintegration, followed by the destruction of the myelin sheath, activation of microglia and macrophages, removal of tissue debris, and reactive gliosis. Wallerian degeneration often results from cerebral infarctions in the CNS, which can impact voluntary movements through the pyramidal tract.1
Wallerian degeneration after pontine infarction is a rare, but possible cause of bilateral middle cerebellar peduncles (MCPs). However, there is no consensus on the clinical and radiological features of the disease.1,2 Over the past years, a report attempted to uncover a relationship between the prognosis of pontine stroke and WD in patients with MCPs, yet the limited number of cases hindered their ability to draw any reliable conclusions.3 In a recent retrospective study, magnetic resonance imaging (MRI) hyperintensities were found in 100% (n=7) of patients with bilateral MCPs in the T2-weighted (T2W) fluid-attenuated inversion recovery (FLAIR) images.4 Therefore, an assessment of the clinical features, neuroradiological findings, and prognosis of patients with WD in bilateral MCPs at different pathological stages of the disease are needed in the literature.
Herein, we report a case of symmetrical WD in asymptomatic bilateral MCPs after a paramedian pontine infarction. In addition, we reviewed the current literature to investigate the clinical, radiographic, and electrophysiological characteristics of this disorder, along with the prognosis, of this disorder. This study aimed to increase the awareness of this disease by providing new insight into the diagnostic criteria, multimodal imaging characteristics, pathological stages, and prognosis of patients with WD of bilateral MCPs.
Case Report
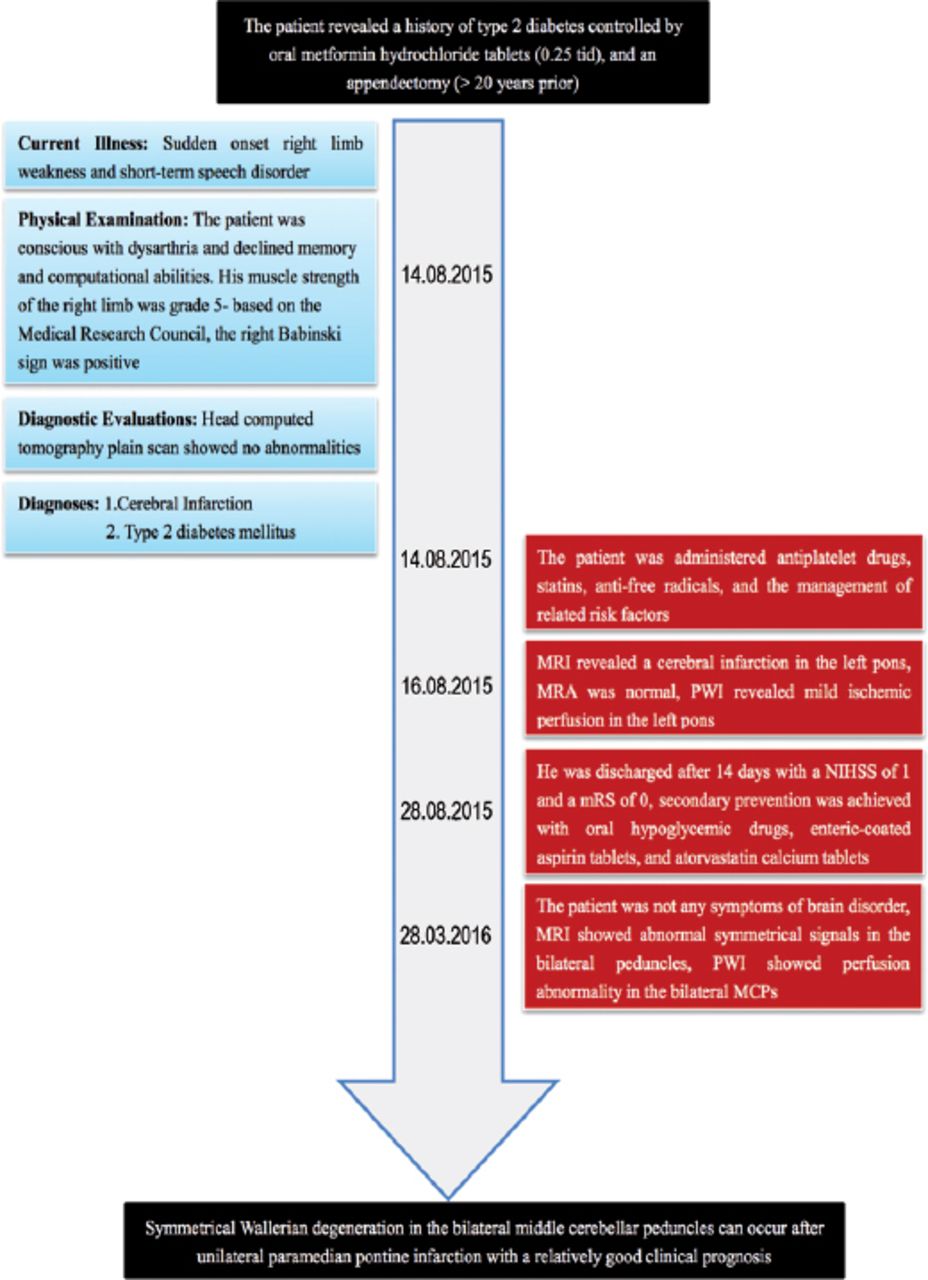
A 66-year-old man with sudden onset right limb weakness and short-term speech disorder (7 hour) was admitted to our hospital on August 14th, 2015. He showed no signs of fever, headache, dizziness, nausea, vomiting, double vision, tinnitus, deafness, incontinence, limb twitching, or consciousness disorders. He revealed a history of type 2 diabetes controlled by oral hypoglycemics, and an appendectomy (>20 years prior). He showed no signs of hypertension, coronary atherosclerotic heart disease, hyperlipidemia, or nephropathy.
Clinical findings
The physical examination revealed a temperature of 36.5°C, pulse of 60 beats/min, respiration of 18 times/min, blood pressure of 135/85 mmHg, pain score of 0, and body mass index (BMI) of 28.34. He was conscious with dysarthria and declined memory and computational abilities. He exhibited a shallow right nasolabial sulcus, tongue extended to the right and a positive water swallow test of 30 mL. His muscle strength of the right limb was grade 5- based on the Medical Research Council, the muscle tension was normal (tendon reflex ++), the right Babinski sign was positive, the left muscle strength was normal (tendon reflex ++), and the left Babinski sign was negative. There were no abnormalities of the deep or shallow sensory system. The bilateral finger-nose and heel-knee-tibia tests were stable and accurate, and the Romberg’s sign was negative. His neck was soft, and the Kernig and Brudzinski signs were negative. The respiratory sounds were clear in both lungs and without dry or moist rales. He had a normal sinus rhythm and strong heart sounds with no pathological murmurs at any of the valve auscultation areas. His abdomen was flat and soft, the liver, spleen, and subcostal areas untouched, with no edema in the lower limbs.
Diagnostic assessment
Routine blood, urine, and stool analyses, along with liver function, renal function, fibrinogen, hypersensitive C-reactive protein, homocysteine, total cholesterol, and low-density lipoprotein cholesterol (LDL-C) were within the normal ranges. His triglyceride level was 2.62 mmol/L, fasting glucose was 6.3 mmol/L, and glycosylated hemoglobin was 6.91%. The chest radiograph was normal. However, echocardiography revealed a light aortic regurgitation and left ventricular diastolic dysfunction, while color Doppler ultrasound of the neck vessels showed plaque formation in the left common carotid and right subclavian arteries. Magnetic resonance imaging (MRI) plus magnetic resonance angiography (MRA) revealed a cerebral infarction in the left pons, but no abnormal changes were detected in the head or neck vessels (Figure 1). Perfusion-weighted imaging (PWI) revealed mild ischemic perfusion at the left monitoring point (fresh infarct area) of the midline pons (Figure 1). Brainstem auditory evoked potential (BAEP) and blink reflection (BR) examinations showed a left BAEP III-V/I-III wave interval ratio >1, along with a healthy right auditory pathway, and functional bilateral trigeminal and facial sensory pathway.

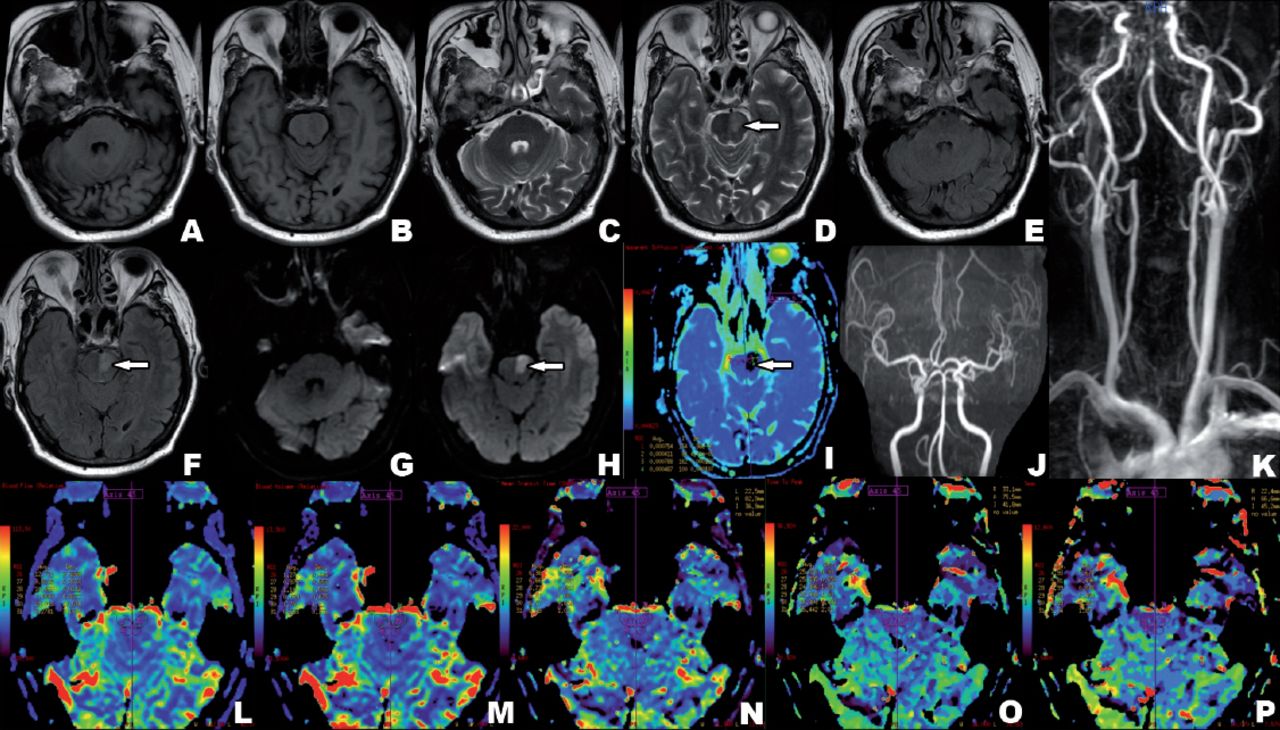
First multimodality magnetic resonance imaging (MRI) showed acute left pontine infarction (August 16, 2015). A-I) High T2-weighted fluid-attenuated inversion recovery, high diffusion-weighted imaging (DWI) signal intensities, and low apparent diffusion coefficient signal intensity, in the left pons paramedian (red arrows). There were no abnormal signals in the bilateral peduncles. J-K) Magnetic resonance angiography (MRA) and contrast-enhanced MRA (CEMRA) showed no significant stenosis of the head and neck vessels. L-P) Perfusion-weighted imaging showed decreased cerebral blood flow and cerebral blood volume of the left peduncles, and prolonged mean transit time, time to peak, and maximum time. There were no noticeable perfusion changes in the bilateral peduncles.
Therapeutic intervention
He was administered antiplatelet drugs, statins, anti-free radicals, and the management of related risk factors. He was discharged after 14 days, when the limb weakness and speech disorder were largely recovered with a National Institutes of Health Stroke Scale/Score (NIHSS) of one and a Modified Rankin Score (mRS) of 0. Secondary prevention was achieved with oral hypoglycemic drugs, enteric-coated aspirin tablets, and atorvastatin calcium tablets.
Follow-up and outcomes
At the 6-month follow-up, he showed no signs of headache, dizziness, speech disorders, limb weakness, or movement disorders. He displayed normal vital signs with no general health or nervous system abnormalities. He could perform routine daily tasks and experienced no symptoms of the disease. However, the patient was assessed in our hospital as requested by the family, and secondary prevention measures were performed for cerebral infarction. The patient’s triglyceride level was 1.92 mmol/L, LDL-C was 3.78 mmol/L, fasting glucose was 6.2 mmol/L, and glycosylated hemoglobin was 6.12%. Color Doppler ultrasound imaging of the neck vessels revealed an uneven thickened inner-median membrane of approximately 1.1 mm, and a posterior wall bilateral common carotid artery bifurcation both shown as hyperechoic irregular spots. Color Doppler flow imaging verified the normal flow of blood in each segment. An unbalanced irregular spot of approximately 12.0 x 9.0 mm was discovered in the posterior wall of the right subclavian artery.
Magnetic resonance imaging plus MRA showed an abnormal signal in the bilateral peduncles, a potential change in the soft lesions of the left pons. However, there were no apparent abnormalities in the blood vessels of the head or neck (Figure 2). Perfusion-weighted imaging showed hypoperfusion in the right cerebellar hemisphere at the bottom of the cerebellum and right side of the medial medulla, hypoperfusion in the lateral MCPs and right midline pons of the upper MCP layer, and hypoperfusion in the right corona (Figure 2).

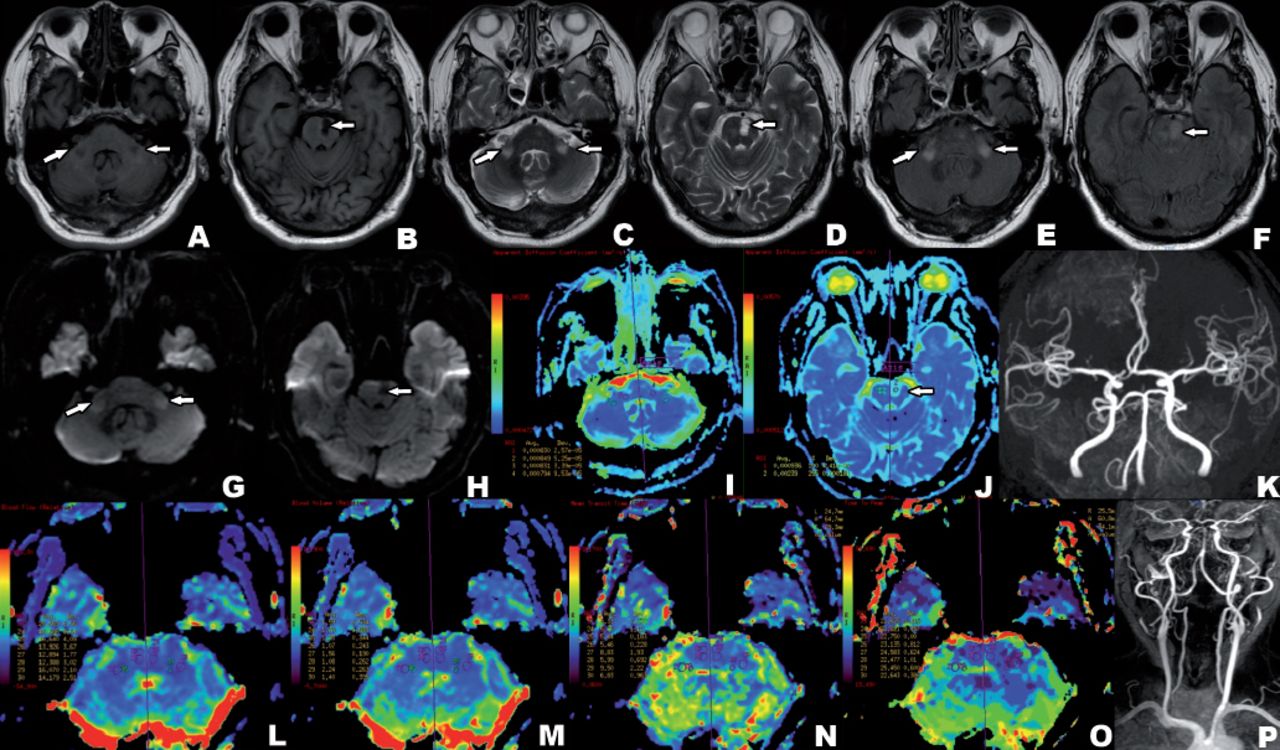
Multimodal magnetic resonance imaging showed bilateral symmetrical Wallerian degeneration in middle cerebellar peduncles (March 28, 2016). A-J) Low T1-weighted (T1W) and diffusion-weighted imaging (DWI) signal intensities in the left pons paramedian, with high T2-weighted (T2W), fluid-attenuated inversion recovery (FLAIR), and apparent diffusion coefficient signal intensity (arrow). Symmetrically low T1W signal in the bilateral peduncles, with high T2W, FLAIR, and DWI signal intensities (arrow). K,P) Magnetic resonance angiography (MRA) and contrast-enhanced MRA (CEMRA) showed no significant stenosis of the head and neck vessels. L-O) Perfusion-weighted imaging showed decreased cerebral blood flow (and cerebral blood volume in the bilateral peduncles, and prolonged time to peak, which was more evident on the right side.
Findings from the BAEP and BR examinations were the same as the first examination, with a left BAEP III-V/I-III wave interval ratio >1 with a normal right auditory pathway, and a normal bilateral trigeminal and facial sensory pathway. Lastly, Figure 3 shows the timeline of the figure.
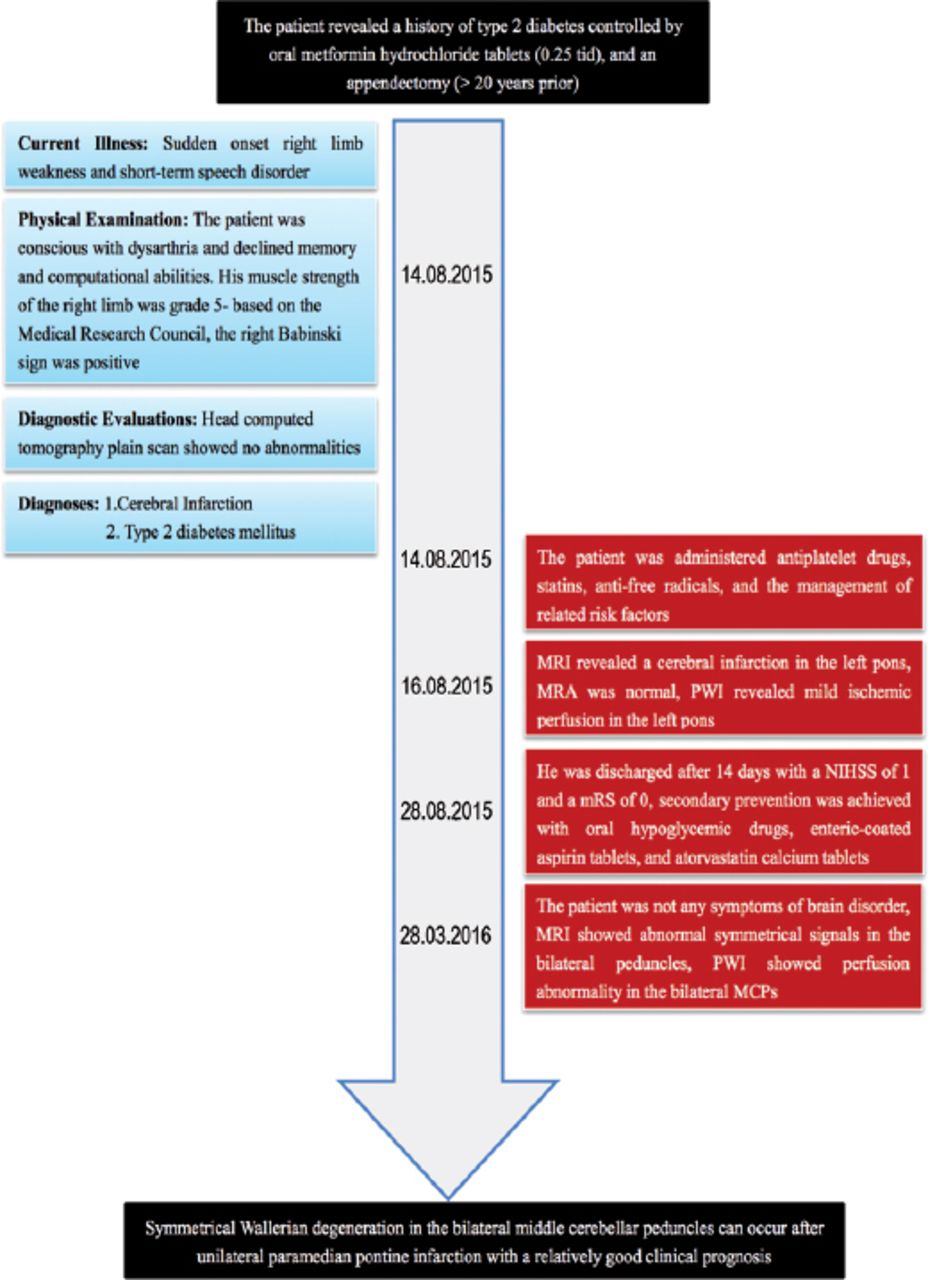
The timeline of the case. The figure showed the symptoms, history, diagnosis and evolution process of the patient.
Discussion
We have collected and summarized the current literature to describe the imaging characteristics and prognosis of patients with symmetrical WD in bilateral MCPs after pontine infarctions. The literature review was limited to case reports about symmetrical WD in bilateral MCPs after pontine infarction in the Wanfang (http://www.wanfangdata.com/) and PubMed (https://www.ncbi.nlm.nih.gov/pubmed/) databases. In the Wanfang database, 2 studies conducted between January 1, 2001 and December 31, 2018 were found, of which the first study reported on a single patient with WD after infarction (Table 1), while the second study had 3 cases with only one as symmetrical WD in the bilateral MCPs after a pontine infarction (Table 1). In PubMed, the search terms “Wallerian degeneration AND middle cerebellar peduncles and pontine infarction,” resulted in 16 studies conducted between from January 1, 2001 and December 31, 2018, 3 studies were excluded from this review, 2 of which were non-case reports, and the third was non-English, which left 13 original reports that contained 21 total cases for our analysis (Table 1).
Characteristics of symmetrical Wallerian degeneration in bilateral middle cerebellar peduncles after pontine infarction.
From the literature search, 23 cases were found to have clinical characteristics similar to our patient. After adding our patient to the data set, we had 24 cases. The 24 cases were comprised of 16 men and 8 women (age range: 37-80 years; mean age: 66 years). Paramedian pontine infarctions were found in all 24 cases, including 8 cases on the right side, 14 cases on the left side, and 2 bilateral cases. When WD was detected, the original symptoms were exacerbated in 5 of the cases, while the other 19 cases showed no symptoms. We recorded the mRS according to the description of the reviewed articles, and a mRS ≥2 was considered a good prognosis. From the 24 cases, 19 had good prognoses, while the 5 cases with severe primary pontine infarctions showed poorer prognoses.
Patient’s perspective
Symmetrical degeneration in the bilateral MCPs is also found in other diseases, including venereal diseases (human immunodeficiency virus), metabolic conditions (Wilson’s disease), inflammatory diseases (acute disseminated encephalomyelitis), drug intoxication (metronidazole), degeneration conditions (olivopontocerebellar atrophy), inherited disease (fragile X ataxia), demyelinating diseases (extrapontine myelinolysis with alcoholism), and cancer (example: lymphoma).5 However, these diseases were excluded from our study based on the clinical symptoms, 2 evoked potential examinations, multimodal MRI.
A unilateral paramedian pontine infarction always results in symmetrical WD in bilateral MCPs, a structure associated with the distribution of nerve fibers at the basilar section of the pons. A unilateral pontine basal infarction damages the ipsilateral pontine nucleus and any surrounding axons, along with the crossed axons that originate from the contralateral pontine nucleus. Wallerian degeneration should be considered when the primary infarct site is close to the secondary site, but not in the same region of the vascular innervation.2
The 24 cases reviewed in this study appeared between 3 weeks and 33 weeks of recovery, indicating that WD is more common during the chronic stage of a pontine infarction. However, an unstable and transiently high DWI signal was also reported 7 days after the cerebral infarction, which disappeared by 22 days after the infarction.6 The pathological process of WD is classified into 4 stages, and each stage is associates with different radiographic alterations. Stage 1, which occurs 0-4 weeks after an acute infarction, involves the degeneration of axons and myelin sheaths. Although the signal alterations are not visible by conventional MRI during this time, DWI may reveal a strong signal intensity. From our literature search, a high DWI signal was found in 2 cases with stage one disease.1,2 Diffusion tensor imaging (DTI) has also been reported to show changes in this stage of WD. Stage 2, which occurs 4-16 weeks after an acute infarction, is associated with the rapid destruction of myelin fragments, along with a low T2 signal intensity on MRI, potentially high T2 signal intensity after nearly 16 weeks, and clinical dyskinesia in some cases. In our review, 5 cases showed worsening of the original symptoms,1,5-8 and 19 cases showed no signs with 4 of the cases being at this stage. During stage 3 at 16 weeks and beyond, the myelin sheath is largely degraded, and gliosis replaces the degenerated axons and myelin sheaths. During this stage of the disease, MRI shows high T2 and FLAIR signal intensities, and low or equal ADC signal. In our review, there were 16 cases with stage 3 disease, as well as our single case from the present study. At stage 4, which occurs several years after onset, the primary MRI alterations involve tissue atrophy, which may cause dyskinesia. According to the pathological staging, WD of bilateral MCPs is primarily observed during stages 2 and 3. However, stage one WD is often mistaken for acute cerebral infarction, which makes it essential to properly stage WD to ensure that patients receive prompt and effective treatment.
From the patients reviewed in this study, only one patient completed a spectral analysis, which revealed a reduced N-acetyl-L-aspartic acid peak,9 while patients with perfusion changes were not reported. In the present study, our patient showed decreased regional cerebral blood flow and volume of the bilateral peduncles, along with a prolonged regional mean transit time and regional time to peak. These findings were consistent with hypoperfusion and indicated the presence of ischemic tissue alterations. These characteristics contributed to the differential diagnosis of several other diseases, including inflammation, tumors, and demyelinating diseases.10 Additional studies are needed to determine whether these are characteristic of WD. Using DTI, a gradual decrease in partial diffusion anisotropy in the medulla oblongata and bilateral MCPs from the 1st to the 12th week after the unilateral pontine basal infarction was previously reported. Thus, DTI can be used for the detection of abnormal focal signals in the MCPs of patients with chronic pontine infarctions, as it accurately reflects the degree and time course of changes of the efferent and afferent cerebellar fibers in WD.
Some of the cases reported has no new clinical symptoms, while others reported new symptoms during the follow-up visits. A few of the cases were diagnosed with WD due to a worsening of the primary symptoms. Similarly, there were no new clinical symptoms in our reported case, and WD in the bilateral peduncles was diagnosed at the 6-month follow-up visit. Brainstem auditory evoked potential and BR examinations are useful for detecting clinical lesions. As the 2 evoked potentials in our case were unchanged, we excluded subclinical lesions. Corticospinal tract WD after acute stroke was previously reported to be associated with a poor prognosis.11 However, from the 24 cases included in the present study, 19 cases had a good prognosis, and 5 cases had a poor prognosis, despite the primary infarctions being relatively severe. Thus, the prognosis of WD after pontine infarction is good, which contrasts with that of the corticospinal tract WD after acute stroke. Wallerian degeneration after pontine infarction, when associated with a severe primary infarction, may further exacerbate the symptoms of the disease.
Study limitations
There were a small number of cases, and the absence of sequential MRI to monitor the evolution of WD. In addition, the effect of therapeutic intervention and physical therapy on the MRI signal were not considered, which may have introduced some bias into our study. As another limitation, some of the multimodality imaging studies included a small number of cases and were unable to obtain regular scans. Hence, the utilization of multimodality imaging in WD requires further investigation.
In conclusion, there are limited information about the clinical characteristics, diagnostic criteria, radiographic features, and electrophysiological changes of WD in bilateral MCPs after a pontine infarction in the current literature. After reviewing of the literature, we found that most patients have no clinical symptoms during follow-up visits, while WD occurred in the patients after a unilateral paramedian pontine in most of the cases. Furthermore, the majority of cases were in Stage 2 and 3 of the disease when the clinical prognoses were good for the patients.
Acknowledgment.
We would like to thank Medjaden Bioscience Limited for English editing and proofreading of this manuscript. We thank Dr. Jing L. Cheng from the First Affiliated Hospital, Zhengzhou University, Zhengzhou, China, for reviewing the figures for clarity and correctness.
Footnotes
Disclosure. This study was funded by the research deputy of National Natural Science Foundation of China (No. 81471203).
- Received May 30, 2019.
- Accepted August 8, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.