


Abstract
Desmoid tumors (fibromatosis) are rare benign tumors, they arise from musculoaponeurotic structures throughout the body. They are locally infiltrative, resulting in a high rate of local recurrence following surgical resection. Due to the rarity of these tumors in the head and neck region, we report a case of a patient with a desmoid tumor in the upper neck that was diagnosed and treated in our institution, to increase the awareness of the Otolaryngology-Head and Neck surgeons, and report available treatment options of this condition.
Desmoid tumors are a group of rare disorders arising from musculoaponeurotic structures throughout the body, and are slow-growing, histologically benign tumors. Despite their benign appearance, they are locally aggressive and invade surrounding structures.1 The incidence is estimated at 2.4 to 4.5 cases per million people annually, and most cases appear to be intra-abdominal with only 7-25% of cases involving the head and neck region.1-3 Due to the tendency of desmoid tumors to invade local structures and to recur, a multi-modality management strategy is usually employed.2,3 However, no management guidelines are available due to the rarity of these tumors in the head and neck region. We report a case of a patient with desmoid tumors of the left postero-lateral region of the neck that was diagnosed and successfully managed initially by wide surgical excision, followed by radiotherapy at a later stage.
Case Report
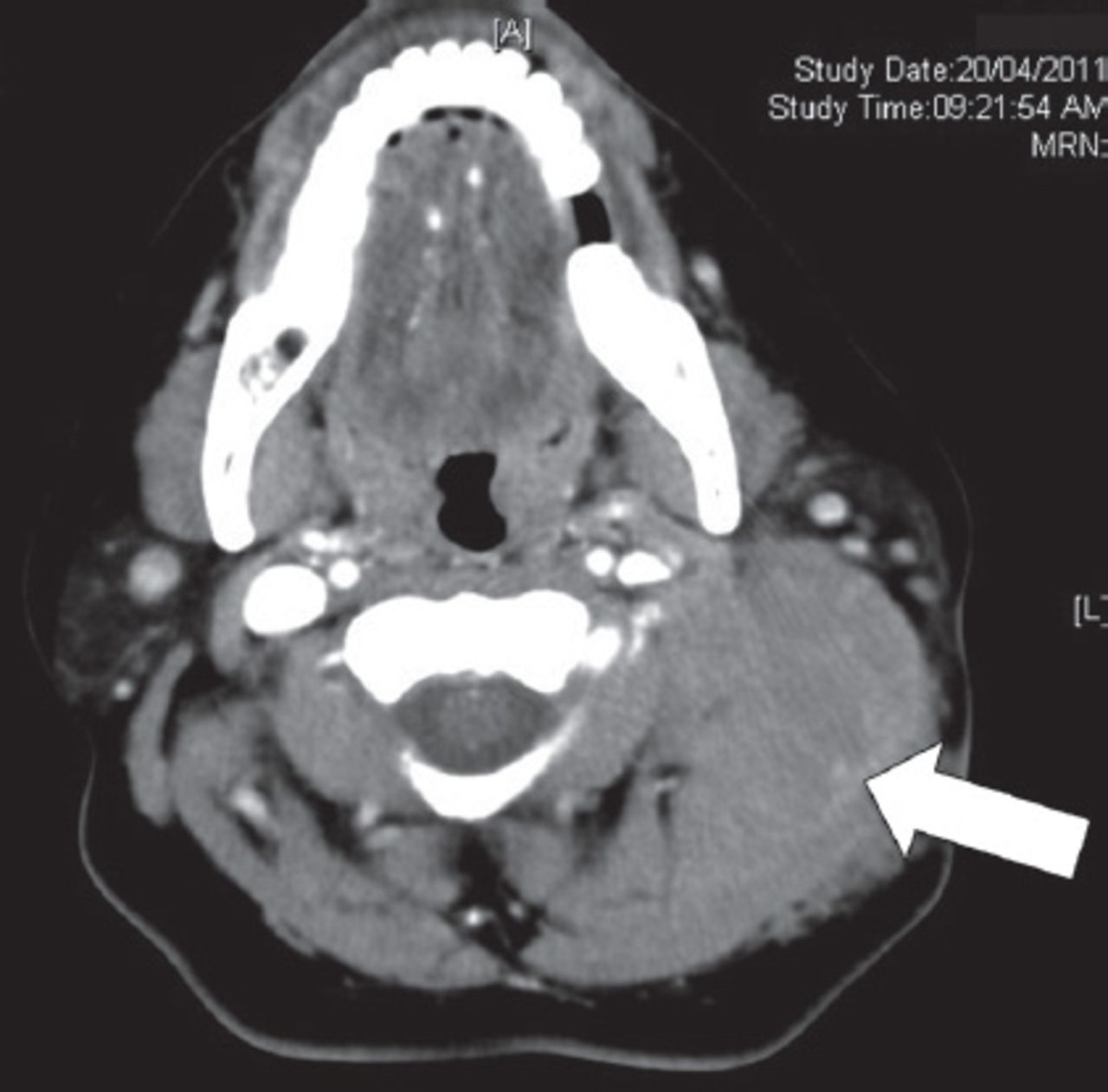
A 42-year-old female patient presented with a history of left neck mass for one year, which was gradually increasing in size. On examination, there was a neck swelling involving the left postero-lateral aspect of the upper neck, which was hard, non tender and fixed to the skin and deep neck structures (Figure 1), her CT scan is showed in Figure 2. After 2 non-conclusive fine needle aspirates (FNA), a biopsy was taken and was consistent with fibromatosis. On the basis of radiological and histopathological findings, a wide surgical excision of the mass was performed with difficulty during her surgical dissection due to local infiltration of surrounding muscles, fibrous tissues, and the tail of the parotid gland. A small remnant was left on top of the carotid artery; just at the bifurcation. Histopathology revealed a proliferation of uniform fibroblasts in a collagenous stroma, with infiltration of adjacent adipose and skeletal muscle tissues with negative excision margins except the part adjacent to carotid (Figure 3). Her surgery was complicated by partial facial nerve paralysis (House-Brackman Grade-II), which recovered completely after one year. Unfortunately, at her 16 month post operative follow up, her small residual was discovered locally above the carotid artery, which was seen in her follow up CT scan, and was noticed to be slowly enlarging, this was elected to be treated by external beam radiotherapy with total dose of 60 Gy. She was closely followed up for 2 years in our clinic with radiographic studies, which revealed significant regression of the tumor.

Clinical photo showing a mass in the left postero-lateral aspect of the neck (arrow).
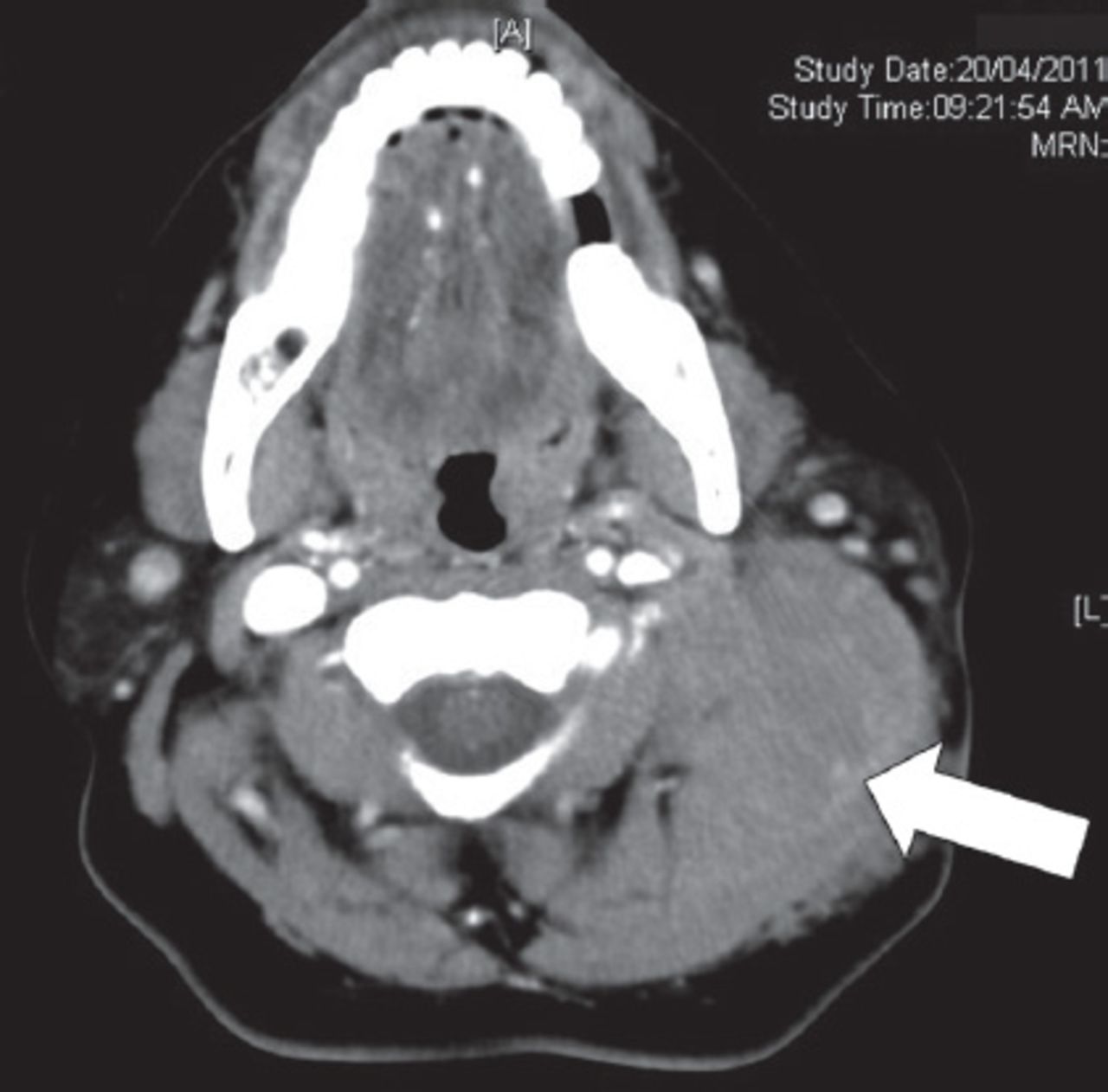
Computed tomography scan of the neck showing a soft tissue mass at the upper neck lateral to the sterno-cleidomastoid muscle, and infiltrating the deep lateral cervical muscles and surrounding superficial and deep fat (arrow).
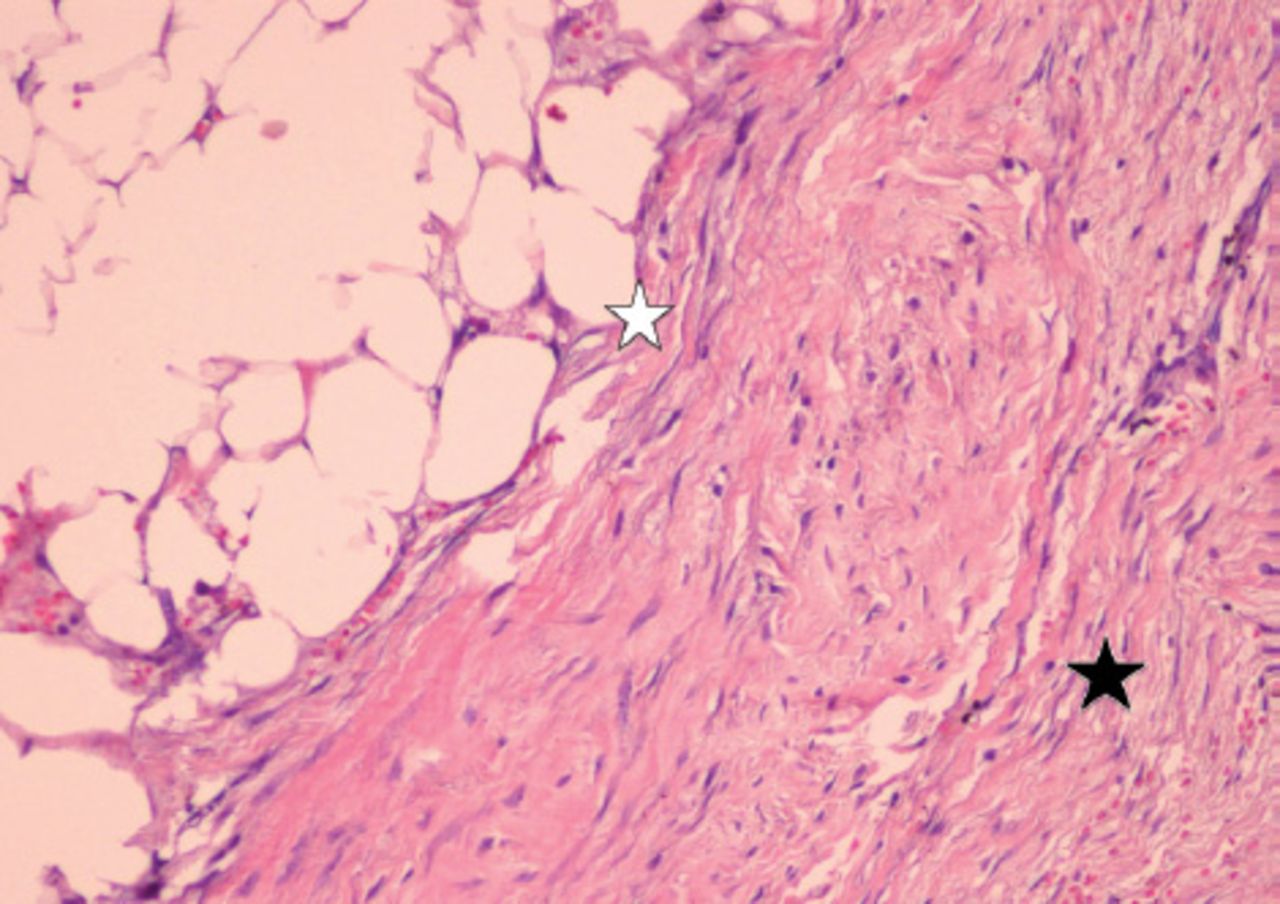
Histopathology (hematoxylin & eosin stain; ×40 magnification) revealing a proliferation of uniform fibroblasts in a collagenous stroma (black star), with infiltration of adjacent adipose and skeletal muscle tissues (white star).
Discussion
In general, desmoid tumors have a female predominance while the highest incidence arises among patients between the ages of 15 to 60 years old.1 According to the location of occurrence, desmoid tumors are classified into 3 types: intra-abdominal, abdominal, and extra-abdominal types. Extra-abdominal desmoid tumors comprise one third of all desmoids tumors and usually occur in the head and neck, shoulder, pelvic girdle, and limbs.3 The neck is one of the most common sites of occurrence, and most of them (80%) occur in the anterio-lateral aspect of the neck, but in our case it was in the postero-lateral region, followed by the face, oral cavity, scalp, and paranasal sinus.3
Unlike other benign tumors of the head and neck region, the true pathogenic potential lies in its ability to locally invade surrounding structures. This fact is of extreme importance in the head and neck region due to the dense anatomy and close association with vital neurovascular and anatomical structure. The histological appearance of this lesion is uniformly spindle shaped cells with an overall benign looking cellular architecture.2,3
The wide surgical excision of the lesion is the primary treatment modality; however, because of the infiltrative nature of the tumor in the head and neck region and sometimes the difficulty of complete surgical resection with negative margin in relation to surrounding vital structures; a multi-modality management strategy is usually employed to control the disease. Surgery is usually followed by radiation therapy for control of residual or recurrent diseases.4
Nuyttens et al5 performed a comparative review of 22 articles on the treatment of desmoid tumor from 1983 to 1998 and found the local control rates of the surgery plus adjuvant radiotherapy group for tumors with positive margin were 75%, and tumors with negative margin were 94%; significantly better than those of the surgery alone group for tumors with positive margin (41%) and negative margin (72%). However, some studies did not show this effectiveness of adjuvant radiotherapy for the tumor with microscopically positive margins.6,7
Radiation therapy is associated with a high risk of complications, especially in the head and neck region, and in our opinion should only be considered in cases with non-operable patients because of significant comorbidity, residual/recurrent disease, or where surgery may significantly impair the functional capabilities of the patient. Chemotherapy and pharmacological therapy can be considered for unresectable tumors, or in cases where surgical and radiation therapy may lead to significant morbidity.6 Sze et al7, reported a significant tumor shrinkage with low dose methotrexate and vinblastine. Meloxicam, a COX-2 inhibitor a non steroidal anti-inflammatory drugs (NSAID), has also been shown to be effective in controlling extra abdominal desmoids tumors.8
There are several systemic agents that have also been used in the treatment of desmoids tumors like hormonal therapy and NSAID’s.9,10 The use of various antiestrogen agents may result in regression of these tumors because of the association of estrogen levels with growth of the tumors especially in intra-abdominal types.9 In the literature, the overall NSAID response rate is around 50% with a combination of other medical therapy, and is usually considered as first-line medical treatment because of its lower toxicity rate.9,10 There are other drugs still undergoing research such as imatinib; the rate of response of solid tumors to imatinib is less than 10%.9 “Wait-and-see” is the new policy for observation of selected patients of unrespectable desmoid tumors, or in patients with significant co-morbidity.9 Due to the unknown natural behavior of the disease, patients should have a close observation period and the final decision whether to treat or not to treat should be based on patient symptoms, medical status, and the biological properties of the tumors.9,10
In conclusion, desmoid tumors are rare benign tumors with a unique biologic behavior and high propensity for local recurrence. The treatment recommendation for these tumors is often contradictory, but due to the high recurrence rate, a multi-modality management strategy is usually employed to control the disease. Local surgical control is usually followed by radiation therapy for control of residual or recurrent diseases and these patients must be closely followed by clinical examination and radiographic studies.
Acknowledgment
The authors would like to thank Dr. Noha Mereani, MBBS, for her help in the initial draft preparation, and Dr. Mohammed M. Abbas, MD for his help in preparing the pathology slide.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received October 16, 2014.
- Accepted November 24, 2014.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}
{kind=link}