


Abstract
We report a case of a 17-year-old female patient, who was operated on for choledocal cyst with Roux-en Y hepatojejunostomy. She was admitted to hospital with recurrent attacks of acute ascending cholangitis due to left intrahepatic duct stones. After a failed attempt at conventional endoscopic retrograde cholangiopancreatography through the anatomical route, she was treated successfully with laparoscopy assisted transjejunal endoscopic retrograde cholangiography.
Endoscopic access to the biliary system can be difficult in patients with surgically altered anatomy of the upper gastrointestinal tract (GIT), such as Roux-en-Y reconstruction, because of the changed anatomy. However, endoscopic retrograde cholangiopancreatography (ERCP) is challenging in cases such as our patient;1,2 this is due to the distance needed to be traversed and looping. Our objective in presenting this particular case is to describe and highlight a laparoscopy assisted transjejunal ERCP to permit successful treatment and removal of intrahepatic duct stones in a post Roux-en-Y patient, and to minimize surgical inetervention to reduce unnecessary risks to the patient.
Case Report
A 17-year-old female, born with choledochal cyst, for which a hepatojejunostomy with Roux-en-Y reconstruction was performed at the age of 4. Postoperatively, she was doing well until 2 years ago, when she had multiple hospital admissions due to recurrent attacks of right upper quadrant and epigastric abdominal pain, fever, and jaundice. She was diagnosed with acute ascending cholangitis, which was managed conservatively. The frequency of the cholangitis attacks increased in the last few months. Therefore, she was referred to our clinic for further evaluation. On admission, clinically, she was sick, in pain, febrile with a temperature of 38.6° C, heart rate 105 beats per minute, blood pressure of 110/60 mm Hg. She was jaundiced, with mild epigastric tenderness on abdominal examination. Hemoglobin (Hb) 13.3 g/dl, white blood cells (WBC) 11.1×103/ul, Platelet (PLT) 249×103/ul, alkaline phosphates (Alk ph), 587u/l, total bilirubin 3.7 mg/dl, direct bilirubin 0.9 mg/dl, and indirect bilirubin 2.8 mg/dl, and international ratio (INR) 1.6. Abdominal ultrasound scan (USS) showed dilatation of the intrahepatic biliary tree with multiple stones. MRCP showed dilated left intrahepatic biliary ducts, which were filled with multiple large stones (Figure 1). Endoscopic access to the anastomosis site (hepatojejunostomy) proved impossible through the conventional route. Therefore, after thorough discussion at the multidisciplinary meeting, a decision was made to carry out ERCP through a laparoscopy approach. She underwent laparoscopy assisted ERCP under general anesthesia in which 3 trocars were placed. An optic tractor was placed in the infraumbilical position and the other 2 5mm trocars at the right and left mid clavicular lines at the level of the umbilicus. The operation began with complete laparoscopy exploration, which was of moderate difficulty due to massive adhesions secondary to the previous operation. Adhesions were released without complications or bowel injury. At the beginning, it was difficult to determine which limb, was the afferent limb, with gentle bowel dissection, we were able to identify both afferent, efferent, and the anastomosis portion of the bowel. The bowel was easily drawn up to the abdominal wall through the optic port laparoscopy incision. A longitudinal enterotomy was performed and a therapeutic channel video gastroscopy (TJF-160VF, Olympus Corporation, Center Valley, PA, USA) was inserted into the enterotomy and advanced to the level of the hepatojejunostomy (Figure 2), which was just approximately 10 cm away from the enterotomy. Under the portable C-arm fluoroscopy (Figure 3), the intrahepatic duct was easily cannulated and cholangiography was performed, which showed evident dilatation of the left intrahepatic bile ducts with multiple stones (Figure 4). Balloon dilatation of the anastomotic site and irrigation of both right and left intrahepatic ducts with saline were performed yielding some pus from the left intrahepatic duct. Some stones were consequently extracted using a 12-15 mm balloon catheter, while a few small stones remained and were expected to pass after our balloon dilatation. The bowel was subsequently freed from the skin and the enterotomy was closed, and one non suction tube drain was inserted into the peritoneal cavity.

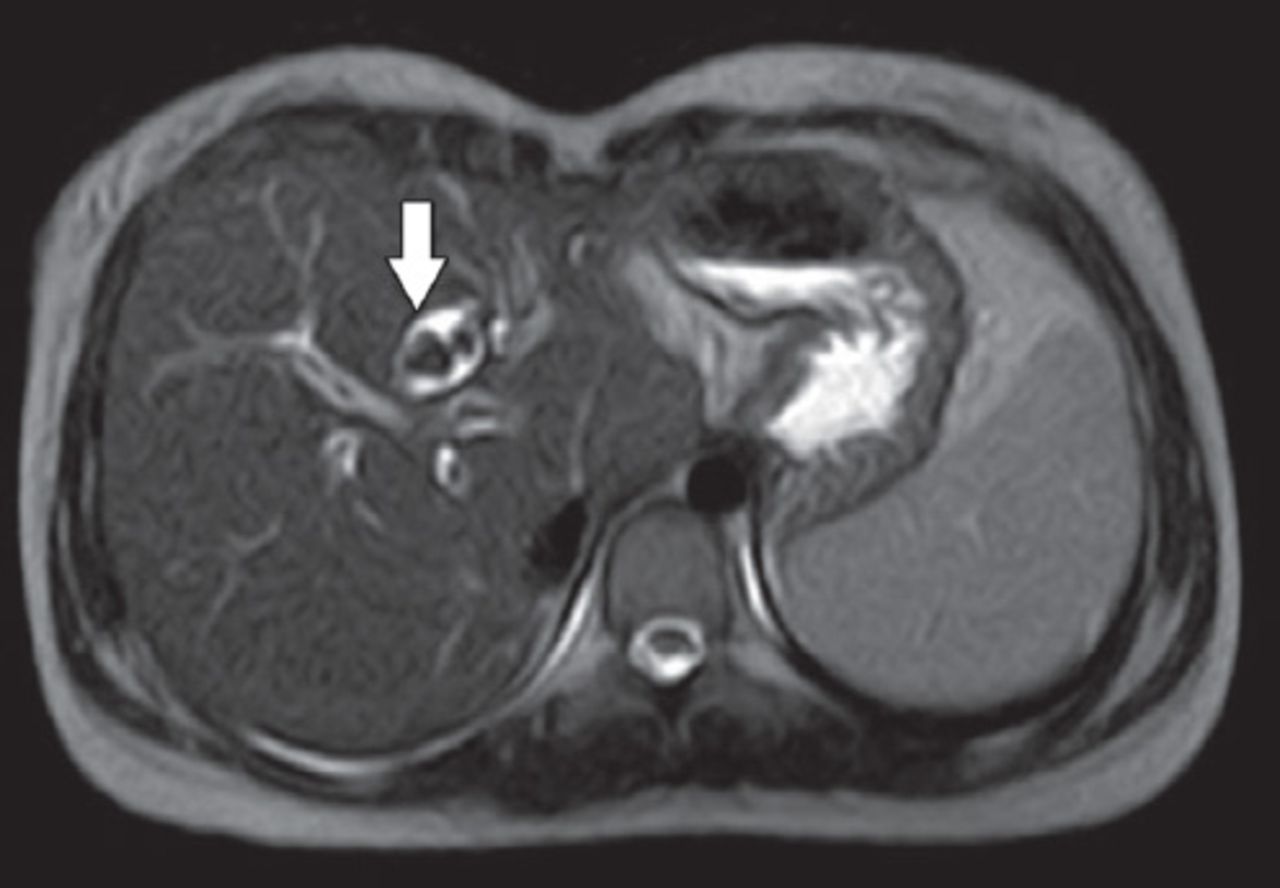
Axial view of magnetic resonance cholangiopancreatography, show multiple stones (filling defect, arrow) in dilated left intrahepatic bile duct.

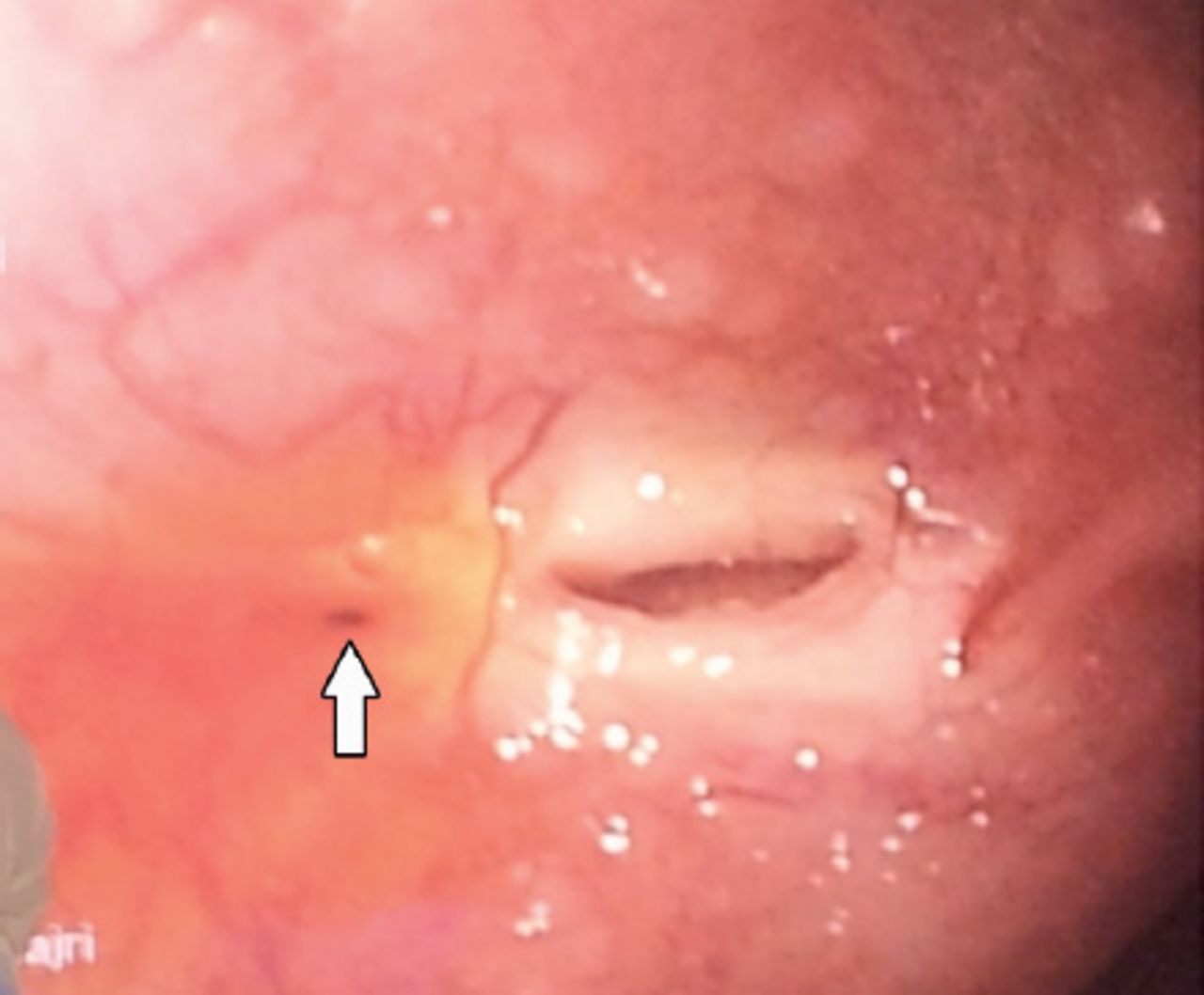
Endoscopic view of the site of anastomosis (hepatico-jejunostomy) with bile secretion.
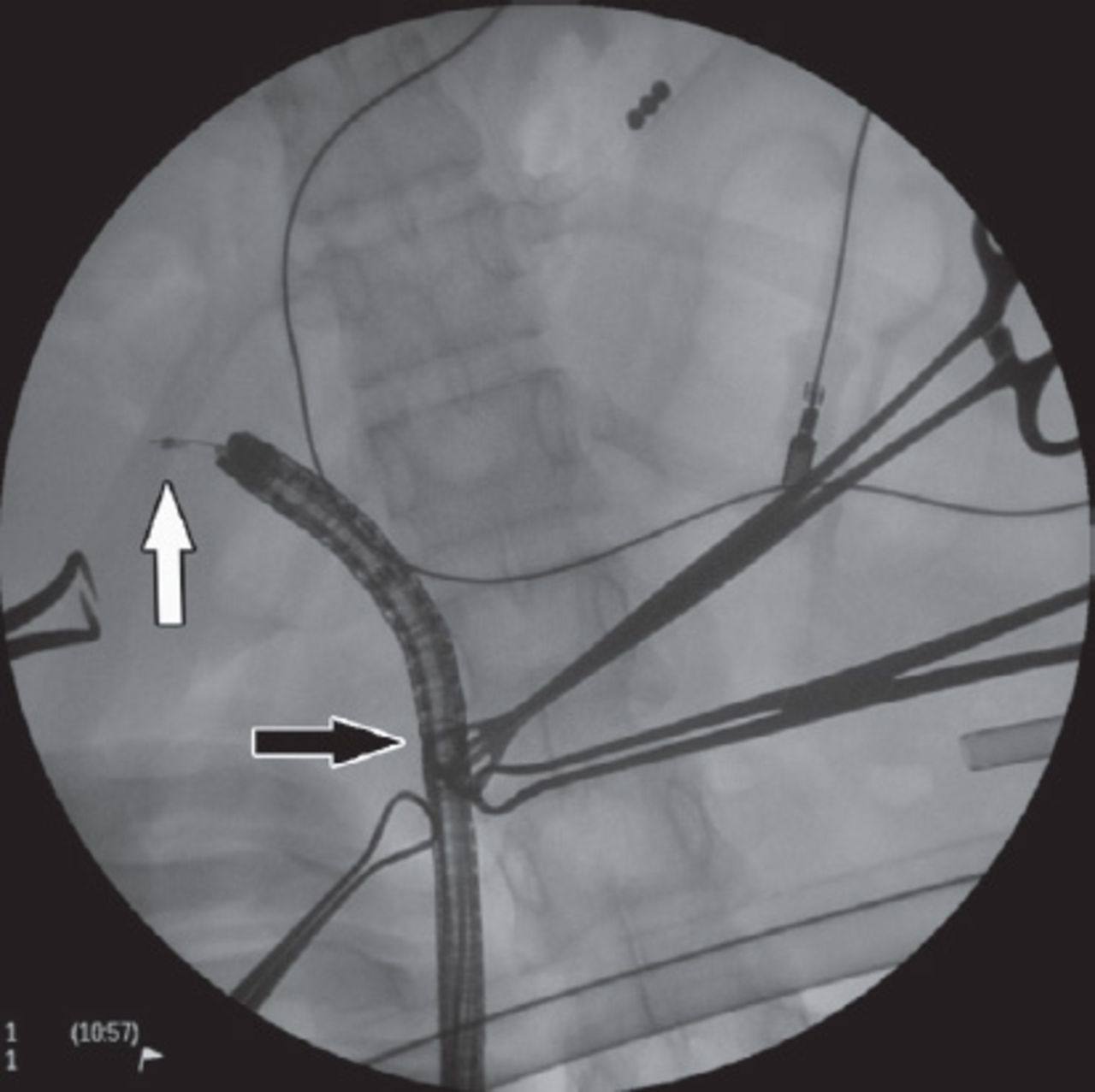
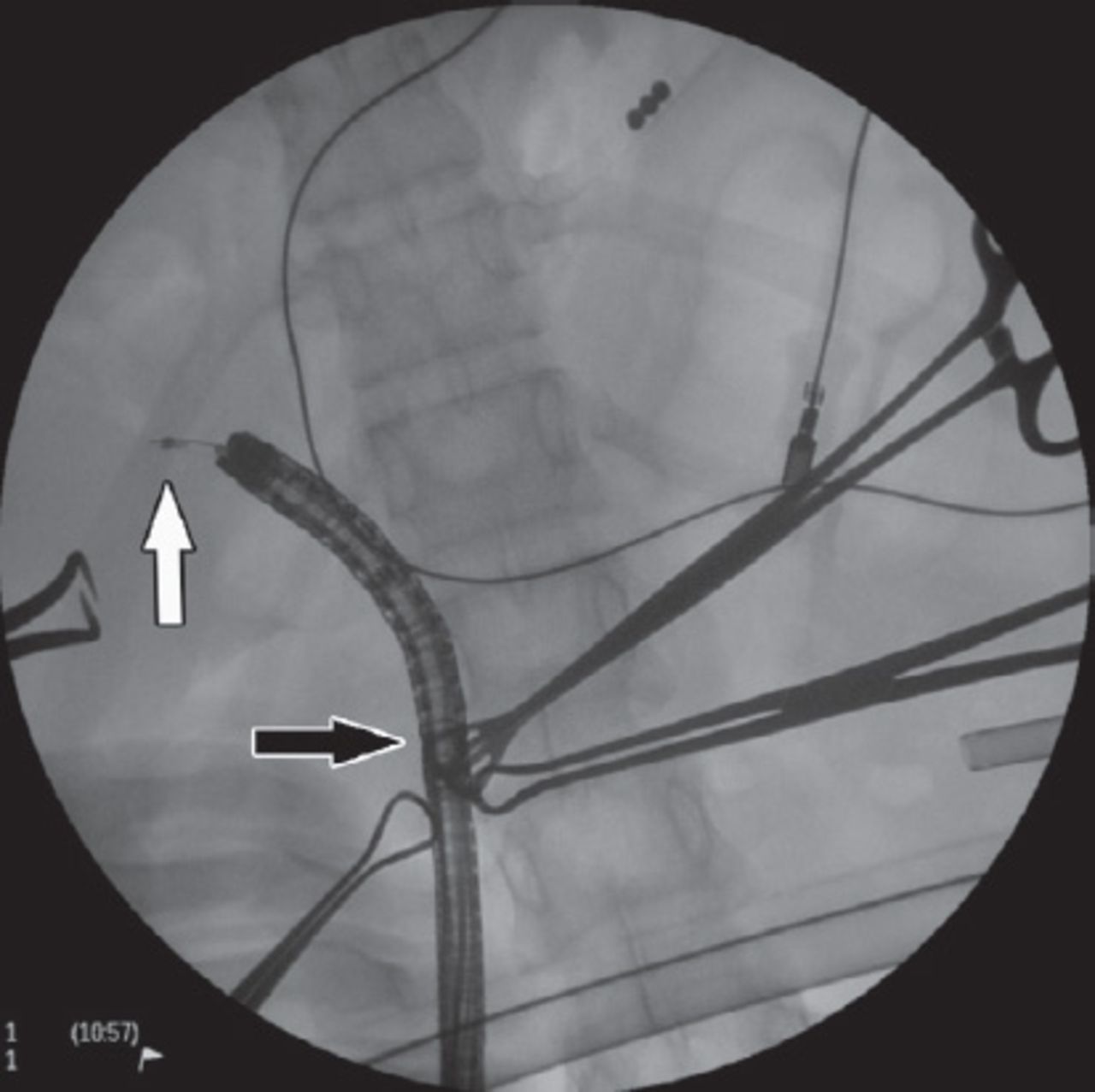
C-arm fluoroscopy view showing the gastroscope introduced through the anterior abdominal wall (optic trocar incision, black arrow), and site of cannulation (white arrow).
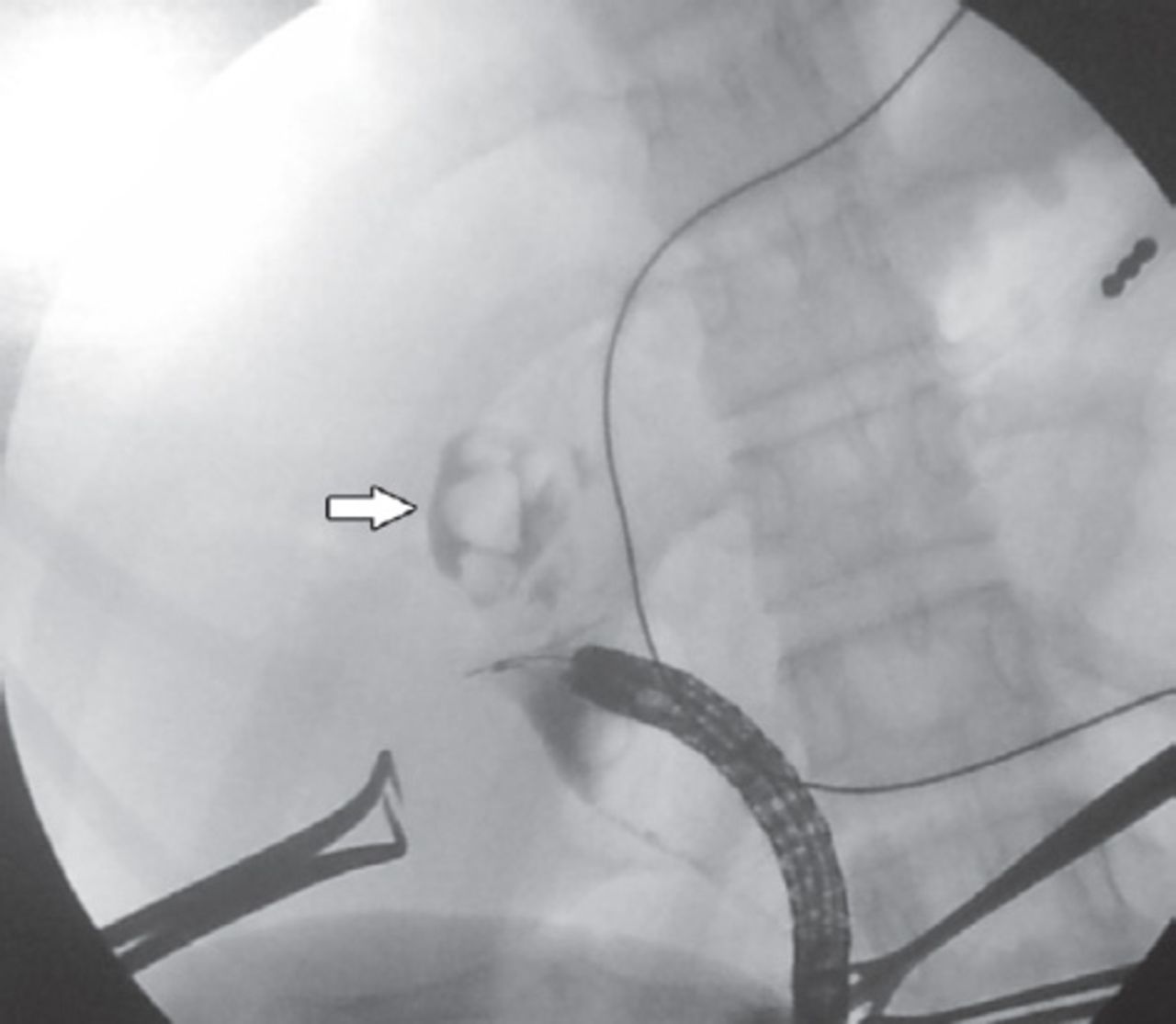
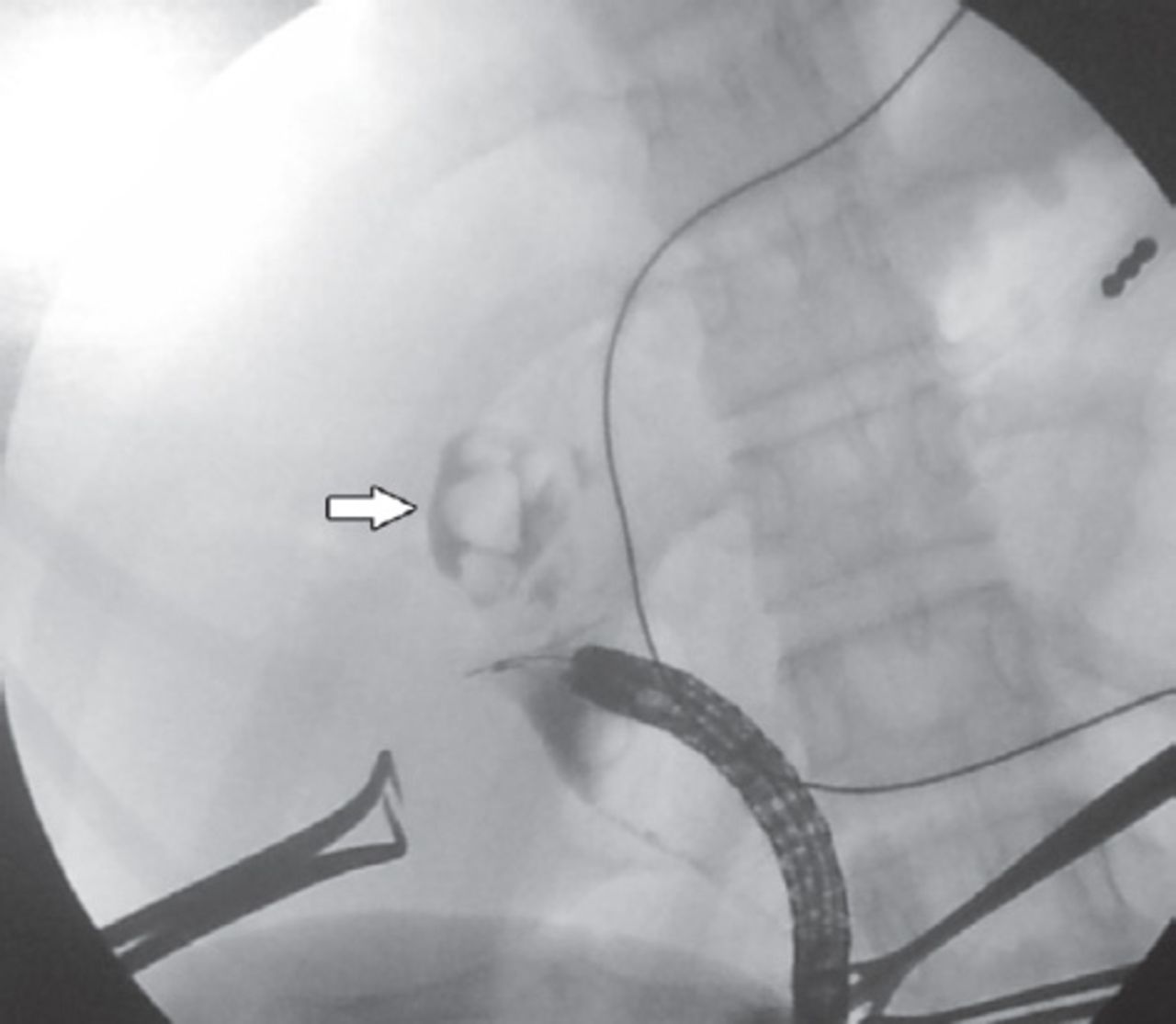
Intrahepatic duct cholangiogram showing left intrahepatic bile duct dilatation with multiple stones (filling defect, arrow).
The post operative period passed smoothly, and she was kept fasting for 3 days and was maintained on dextrose saline, Ceftriaxone one gm twice daily and Acetaminophen 250 mg 4 times a day. She was discharged home 5 days later in a very good general condition. Her investigations on discharge day were, Hb 12.1 g/dl, WBC 10.5×103/ul, RBC 4.3×106/ul, PLT 171×103/ul, total bilirubin 1.0 mg/dl, direct 0.4 mg/dl, and indirect 0.6 mg/dl. An abdomen USS showed small stones at the site of anastomosis. She continued to improve, and one month later, a follow-up abdomen USS showed minimal dilatation of intrahepatic ducts, which were free from stones. She followed in the outpatient clinic for one year after the procedure with no surgical complications reported.
Discussion
Roux-en-Y gastric bypass is a surgical procedure that leads to alteration of upper gastrointestinal tract anatomy, which may be performed in management of congenital diseases such as choledochal cyst (as in our case), management of benign disorders like bariatric surgery in obesity, pancreaticoduodenectomy (Whipple procedure) in treatment of chronic pancreatitis, liver transplantation, and repair of bile duct injuries with formation of hepatico-jejunostomy. It is also a part of the management of malignant diseases such as partial or total gastrectomies in gastric cancer, Whipple procedure in pancreatic cancer, distal cholangiocarcinoma, and periampullary carcinoma.
Due to increased popularity of the Roux-en-Y bypass operation, we should expect a parallel increase in the prevalence of bile duct diseases that occur in these patients. In this situation, stone extraction, and bile duct clearance remain challenging.3-5 Our patient had a hepatojujenotomy anastomosis, which was working very well for the previous 13 years, but lately she formed stones in the left intrahepatic ducts making her susceptible to cholangitis. At this point, we did not want to expose her to a major operation as revision of the satisfactory functioning anastomosis to remove the stones. Furthermore, we did not want to subject her to the risk of operative dissection in a massive adhesion area of a previous operation, which carries the risk of adjacent organ injury, and biliary leak from the new anastomosis. Therefore, we took the decision to attempt a routine per oral ERCP to access the biliary tree first. Unfortunately, the attempt did not succeed. In patients with complex upper GIT anatomy per oral ERCP is challenging1,2 due to the changed and long-length anatomy.
Intraoperative ERCP is often performed in patients with Roux-en-Y gastric bypass, in which the papilla is usually not accessible through endoscopy.6 Intraoperative transjejunal ERCP uses an open approach with a small incision, it was first reported by Mergener et al.7 In that case, a successful biliary intervention took place in a patient with a Roux-en-Y hepatojejunostomy. With the development of laparoscopy, and clear appearance of its advantages; such as lower rates of wound complication, less post operative pain, and early return to normal activity, we decided to use the laparoscopy approach for this procedure. Using laparoscopy assisted endoscopic retrograde cholangiography; we could achieve a minimally invasive ERCP procedure to remove stones without the need to expose the patient to the major risks of operation. Cannulation and dilatation, at the site of anastomosis, washing of intra-hepatic bile ducts with normal saline and stone extraction through an easy, short way by opening of the efferent jejunal loop near to the site of the hepatojujenal anastomosis.
In this paper, we described our experience in the diagnosis and treatment of a biliary disease using laparoscopy assisted transjejunal ERCP in a patient who had altered anatomy of the upper GIT due to previous surgical intervention. Access to the Roux limb was easily obtained, a diagnostic cholangiography was carried out, and therapeutic interventions were performed at the same time. These results are in line with recent reports that demonstrated the safety and feasibility of the laparoscopy assisted transjejunal ERCP procedure for this indication, and in selected cases of hepato-biliary-pancreatic lesions, since these procedures require expertise in laparoscopic surgery and ERCP.
By reviewing the literature, Lopes et al8 concluded that laparoscopy assisted ERCP is a valuable option in patients with Roux-en-Y anatomy. They reported a patient with partial gastrectomy and Roux-en-Y reconstruction who presented with abdominal pain due to sphincter of Oddi dysfunction. After failed conventional ERCP, the procedure was successfully performed by laparoscopic assistance through an enterotomy into the biliopancreatic limb.
Saleem et al9 also concluded that laparoscopy assisted ERCP is a useful modality in patients with surgically altered anatomy. After treating a patient with subtotal gastrectomy with Roux-en-Y gastrojejunostomy, the procedure became furtherly complicated by recurrent left pleural effusion due to pancreaticopleural fistula. After a failed conventional ERCP, the fistula was managed successfully with laparoscopy-assisted transjejunal ERCP (Table 1). To date, there is no single standard therapeutic method for treating biliary duct stones in post Roux-en-Y patients. However, we found several techniques that have been reported. Double balloon endoscopy techniques were used to examine the entire small bowel and to access the biliary tree.10 Percutaneous open surgical and endoscopic gastrostomy allows antegrade transgastric ERCP,11 and percutaneous transhepatic cholangiography for accessing the biliary tree and treatment of choledocholithiasis after laparoscopic gastric bypass surgery.12
Intraoperative (conventional and laparoscopic) assisted transjejunal ERCP in literatures.
Schreiner et al13 demonstrated the feasibility of laparoscopy assisted ERCP as a minimally invasive technique in managing biliary stones in a patient with Roux-en-Y gastric bypass patients. The indications for each of the above methods depends upon various factors such as, the experience of the managing team, fitness of the patient for the procedure, fitness for general anesthesia, and the cost of the procedure.
In conclusion, laparoscopic assisted transjejunal endoscopic retrograde cholangiography is a possible alternative method as a diagnostic and therapeutic option for the treatment of intrahepatic biliary ducts disease in patients with a Roux-en-Y operation.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received September 30, 2014.
- Accepted October 20, 2014.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.