


Abstract
In this paper, we present 2 rare cases of persistent embryonic anastomoses. In one case, the patient presented with persistent trigeminal artery along with multiple foci of cerebral infarction as well as central retinal artery thrombosis. In the other case, the patient had direct anastomosis of the vertebral artery with ipsilateral external carotid artery as well as pontine infarction, aneurysm, and unilateral hypoplasia of the vertebral artery. The findings in these cases may shed light on the clinical presentation of such persistent anastomoses and aid their detection in clinical settings.
The primitive trigeminal artery (PTA) is a temporary embryonic vascular anastomosis between the carotid and vertebrobasilar arteries. The persistence of the PTA into adulthood is an uncommon congenital cerebrovascular variation that results in an abnormal anastomosis between the carotid and basilar arteries. The incidence of persistent PTA (PPTA) was reported to be 0.1-1.0%.1,2 The advances in neuroimaging techniques have led to the increased detection of PPTA and prompted considerable research interest in its clinical significance.3,4 Studies have shown that in approximately 25% of the cases, PPTA occurs in combination with other cerebrovascular lesions, such as aneurysms,5 cavernous fistula, and arteriovenous malformation,6,7 which are clinically manifested as trigeminal neuralgia, paralysis of the oculomotor nerve or abducens nerve, or palsy of the trochlear nerve.2 These conditions can lead to compression of the brain stem and, eventually, cerebral ischemia.8 The detection of the PTA is also important from the standpoint of the safety of surgical and interventional procedures performed on the affected population. However, changes of cranial hemodynamics associated with PPTA are complicated, and how and what PPTA lead to stroke is also unclear. The PPTA linked to central retinal artery occlusion and embolic stroke are a rarely reported cerebral vascular accident. The objective of this study is to present 2 cases of rare types of PPTA diagnosed on the bases of the findings of brain magnetic resonance angiography (MRA). In the first case, the PPTA occurred along with multiple foci of cerebral infarction and central retinal artery thrombosis. In the second case, the patient had direct anastomosis of the vertebral artery with the ipsilateral external carotid artery, in combination with pontine infarction, aneurysm, and unilateral hypoplasia of the vertebral artery.
Case Report
Patient 1
The patient was a 73-year-old man who was referred to our hospital from the local hospital for the evaluation of dizziness, weakness of the lower extremities, and blindness of the left eye. The symptoms were first noticed 20 days before admission, after a walk. His blood pressure at that time was 180/100 mm Hg (≤140/90 mm Hg). He had been diagnosed with hypertension and coronary heart disease one month before the episode, with the highest blood pressure recorded of 200/110 mm Hg; however, he did not receive any treatment. He was a habitual smoker, smoking approximately 900 cigarettes a year. With regard to family history, he reported that his father had died of some form of brain disease.
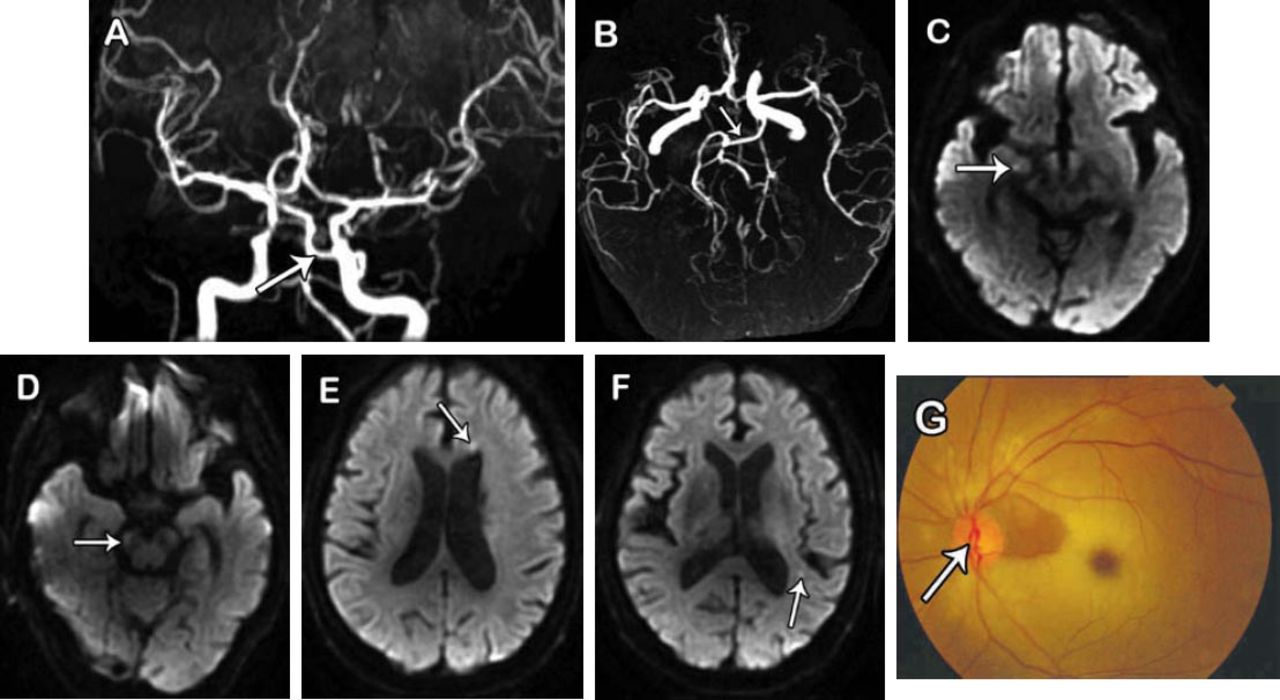
The findings on physical examination at the time of admission to our hospital were as follows: body temperature 36.5°C (36.3-37.2°C); pulse rate, 60 beats/min (60-100 beats/min); respiratory rate 19 cycles/min (16-24 cycles/min), and blood pressure 200/100 mm Hg (≤140/90 mm Hg). He was conscious, with normal verbal fluency, but cognitive decline. Examination of the eyes revealed symmetry of the eyelid fissures and normal eye movements on both sides, without nystagmus. The diameter of the left input was 4.0 mm and of the right pupil was 3.0 mm, with a slow response and high sensitivity to light. The visual acuity by left eye was limited to hand movement only. Muscle strength of the upper limbs was of grade 5 and that of the lower limbs was 4+, with normal muscle tone and tendon reflexes (++) in both the upper and lower limbs. The Babinski sign was positive on the left side and negative on the right side. When the Romberg test was performed, he had imbalance on opening or closing the eyes. No abnormalities were detected on examination of the chest and abdomen, and no edema was noted in the lower extremity. He had arrhythmia and premature beat, but no pathological murmurs were detected on auscultation of the valve area. Vascular sonography of the neck revealed a bilateral increase in the intima-media thickness of the carotid artery and bilateral plaque formation in the carotid arteries. Echocardiography revealed: aortic regurgitation, reduction in the magnitude of the motion of the left ventricular anterior wall, left ventricular diastolic dysfunction, and arrhythmias. No abnormalities were detected on transcranial Doppler ultrasonography. Transesophageal echocardiography showed patchy, hypoechoic areas in the aortic arch. The Holter exam showed sinus rhythm, with junctional escape beat and wandering heart rhythm. The average heart rate was 61 beats/min (range, 46-87 beats/min), with continuous ST-segment depression and T-wave flat changes. The serum levels of brain natriuretic peptide level was 147.5 pg/mL and homocysteine was 23.43 µmol/L. The results of other routine blood, urine, and feces tests were normal. The findings of cranial MRI, MRA, and fundus photography are shown in Figure 1.

Imaging findings in patient 1: A-B) persistent primitive trigeminal artery, basilar artery hypoplasia, and C-E) right vertebral artery hypoplasia revealed by magnetic resonance angiography, F) multiple infarcts, as indicated by spots in the anterior and posterior circulation by diffusion-weighted imaging, and G) occlusion on the left central retinal artery detected by fundus fluorescein angiography.
Patient 2
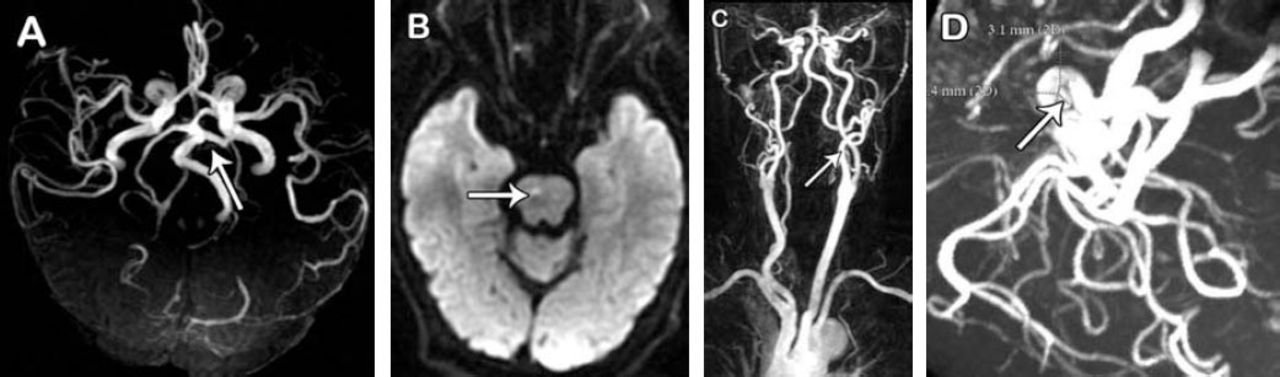
An 80-year-old woman presented to our hospital with a sudden onset of dysphasia with dizziness and cough for one day. She had a 30-year history of hypertension, and 12-year history of cerebral infarction. On physical examination, her body temperature was 36.4°C; pulse rate 72 beats/min, blood pressure 160/90 mm Hg, and respiratory rate 18 cycles/min. She was conscious, with mild dysarthria, and cognitive decline. The right side showed a slow response to the gag-reflex test, and the drinking water test (30 mL) was positive. No other signs of cranial nerve abnormalities or abnormal movement of the limbs were noted. The Romberg test showed unsteadiness on opening or closing of the eyes. No abnormalities were observed on abdominal and cardiopulmonary examinations, and no edema was present in the lower extremities. Vascular ultrasonography of the neck showed an increase in the resistance index of the right common carotid artery and bilateral plaque formation in the carotid arteries. Further, the blood flow signals from the middle section of the left vertebral artery were minimal. Echocardiography revealed marked enlargement of the left atrium, thickening at the base of the ventricular septum, mild mitral and aortic regurgitation, and left ventricular diastolic dysfunction; however, the echocardiogram was almost normal. The serum level of brain natriuretic peptide was 153.5 pg/mL. The results of other blood, urine, and stool tests were normal. The findings of cranial MRI and MRA are presented in Figure 2.

Imaging findings in patient 2: A) persistent primitive trigeminal artery, and B) right vertebral artery hypoplasia revealed by magnetic resonance angiography, C) right pontine infarct by diffusion weighted imaging, D) communication between left vertebral artery and external carotid artery revealed by contrast enhanced magnetic resonance angiography (aneurysm in the left internal carotid artery by magnetic resonance angiography).
Discussion
During embryonic development, several anastomoses are present between the developing carotid artery and the vertebrobasilar system, including the PTA, hypoglossal artery, otic artery, and proatlantal intersegmental artery; these anastomoses exist only for 7-10 days, and then involute in normal individuals. In some cases, these anastomoses remain patent even in adulthood.4 The PTA is the most common cerebrovascular anastomoses observed, and PPTA can be classified into 3 types; namely, Saltzman types I, II, and III. The PPTA in Patient 1 was classified as Saltzman type I. The head MRI showed infracts in the anterior and posterior circulation as well as embolization in the central retinal artery of the left eye; this combination of PPTA and unilateral embolization of the eye has not yet been reported. In light of the results of the Holter test and transechocardiography, it may be inferred that cardiogenic embolism was the most probable cause of the symptoms in this case. The detached fragments of the emboli possibly travelled to the left ophthalmic artery, and the basilar artery via the left internal carotid artery. Previous reports9 have indicated that PPTA could result in the communication between the anterior circulation and posterior circulation, with vascular support from the ipsilateral internal carotid artery. Stenosis or rupture of the atherosclerosis plaques or cardiogenic emboli in the ipsilateral internal carotid artery can lead to the simultaneous ischemia or infarction of both the anterior and posterior circulations. Patient 1 had higher blood flow and pressure in the internal carotid artery than in the vertebrobasilar system as well as hypoplasia of the basilar artery; therefore, the possibility of the emboli moving from the vertebrobasilar system into the internal carotid artery appears to be minimal. In addition, as the left common carotid artery directly originates from the aortic arch, it is possible that the cause was a cardiogenic emboli that ruptured into the left internal carotid artery system. Thus, the simultaneous infarction of both the anterior and posterior circulation could PPTA.
Patient 2 had PPTA of Saltzman type II. Cranial MRI revealed acute pontine infarction. This is the second report of this combination of PPTA with direct anastomoses of the vertebral artery (VA) and the ipsilateral external carotid artery (ECA), the ECA-VA anastomose is so-called type 2 proatlantal artery. Uchino et al10 reported the first PPTA associated with type 2 proatlantal artery. However, in our patient, aneurysm and infarction were found together, which has not been reported yet. The vertebral artery is very thick in the presence of PTA. There is an abnormal blood flow between the anterior and posterior circulation via the internal carotid and external carotid artery anastomosis, which may have a compensatory effect on the blood flow in the basilar artery system. Previous studies have shown that PPTA may be associated with several cerebrovascular abnormalities.1,3 The PPTA was reported to occur along with a missing carotid artery and occlusion9 and in combination with hypoplasia of the basilar artery.1 These appearances support the fact that embryological abnormal development is the probable cause. The presence of the PTA resulted in the communication between the anterior and posterior circulation and established a direct connection between the ipsilateral carotid and vertebral artery, which is very rare. The cerebrovascular compensation offered by this double loop structure had a beneficial effect. We agree and believe that PTA may be found more frequently if cerebral MR angiography is routinely performed and includes the carotid bifurcation.
In conclusion, the recognition of PPTA in a clinical setting is important to avoid mistaking these lesions for other pathological abnormalities. The PPTA is indicative of cerebrovascular developmental disorders and is often accompanied by one or more cerebrovascular abnormalities. The PPTA and other congenital abnormalities capable of causing hemodynamic changes should be ruled out in cases where there are infarctions in both anterior and posterior circulation.
Acknowledgment
We thank Dr. Jing L. Cheng from the First Affiliated Hospital, Zhengzhou University, Zhengzhou, China, for reviewing the Figures for clarity and correctness.
Footnotes
Disclosure. This study was supported by the Bureau of Science and Technology, Zhengzhou City, China (No. 20130559). Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received October 30, 2014.
- Accepted February 12, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.