


Abstract
It is very rare to have a big foreign body in the lungs without any complications or symptoms for 2 years. A 14-year-old male with episodes of minor hemoptysis for 4 weeks had a history of inhalation of a bullet 2 years earlier. He had asymptomatic for lung complications for 2 years. The bullet was removed by right thoracotomy and non-anatomical wedge stapled resection, and he followed an uneventful recovery. An aspirated foreign body although big can remain asymptomatic for a long time, especially if it has migrated to the periphery.
Latency of a foreign body (FB) in the thoracic cavity is something not common.1 Generally, the etiologies for the presence of such FBs include traumatic intention, accidental, or iatrogenic.2 Foreign bodies of airways are known for acute and chronic complications related to partial obstruction leading to choking, or secondary pathologies of the lungs including variable degrees of respiratory distress, atelectasis, chronic coughing, recurrent pneumonia, and even death.3 Foreign body aspiration (FBA) can be completely asymptomatic.4 The objective of the study is to act as instructive example with the record of clinical interactions, which help us to frame the investigations undertaken in order to determine a diagnosis and the course of treatment the patient underwent as a result for more rigorously designed clinical studies.
Case Report
A 14-year-old male with episodes of minor hemoptysis for 2 weeks. He neither got admitted nor had any respiratory ailment According to his father, he inhaled a bullet 2 years ago, but since then had remained asymptomatic, and no intervention was carried out.
His chest roentgenogram showed a FB in the right lung, and the lateral view of his chest roentgenogram indicated an aspirated bullet in the extreme periphery at the right lung base (Figure 1). Confirmation was carried out by CT of the chest with intravenous contrast, and showed a bullet showing a streak artifact in the posterior basal region of the right lower lobe in the peripheral 2 cm zone of the lung (Figure 2). The scan also showed dilated sub-segmental bronchus with no evidence of bronchiectasis, or cavitation. The remaining lung fields appear to be normal in the scan, which indicates the absence of any other pathological reason for causing hemoptysis in the patient. Bronchoscopic examination was not carried out due to the association of FB, leading to localized bronchiectasis, was quite obvious on the CT scan. Bronchoscopic examination was not expected to add any information to the clinical workup. Following consent for thoracotomy and wedge resection, a right posterolateral thoracotomy was performed at the seventh intercostal space with one lung ventilation using double lumen endotracheal tube under general anesthesia. The lower lobe had extensive adhesions with the diaphragm, which were lysed, and the FB was palpated in the posterior basal segment of the lung. The affected area was secured by duval forceps (Figure 3). Figure 4A shows non-anatomical wedge resection of the lung, within 1.5 cm from FB, carried out using 2 linear staplers (auto suture DST 80, 4.8 size).

Chest film showing the bullet A) lying in the lower zone of the right lung and B) the lateral view located peripherally.

Computerized tomography scan showing the A) deeply located bullet in right periphery of the lung, B) streak artifact, and C) the dilated sub segmental bronchus with no evidence of bronchiectasis or cavitation

Intraoperative photographs showing the A) collapsed right lung with bullet inside and B) the bullet in the lung using the Duval forceps (arrow).

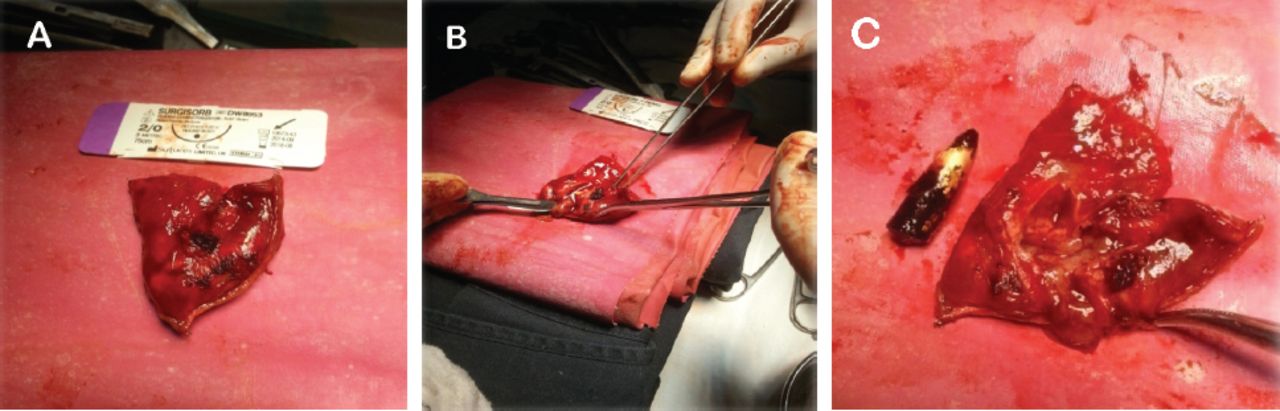
Photographs showing the A) resected part of right lung, B) incising the part for bullet retrieval, C) and the retrieved bullet and excised part of the lung.
Figures 4B & 4C the resected piece of the lung was then incised to retain the aspirated bullet. Postoperatively, airtight stapling was confirmed by saline dip test. He followed an uneventful recovery with extubation of the chest tube on the fourth postoperative day, and was discharged.
Discussion
Removal of an impacted FB from the lung is a great challenge for the thoracic surgeon especially if it is deeply located. In adults, the FBs are wedged distally mostly in the right lower lobe. Unlike this case, most FB inhalations are caused by cough, sputum, hemoptysis, and choking; and if dwell chronically can cause structural changes in the involved lung. The patient in this case was totally asymptomatic as he aspirated the bullet 2 years ago, and had no any respiratory symptoms. He took a medical advice when he started complaining of hemoptysis 4 weeks after. The radiographic findings showed the bullet located in the peripheral lower lobe of the right lung, but there was no finding of chronic suppuration. In such cases, FBs from the pleural cavity can be extracted either through thoracotomy, or video assisted thoracoscopic surgery (VATS)2 which gives the surgeon excellent exposure for removal of the object under direct vision.5 In this case, we choose an open thoracotomy due to the anticipated adhesions of the lower lobe with the diaphragm and peripheral posterior location of the FB. In an uncomplicated late presenting case, the decision was toward lung conservation in the form of stapled wedge resection as the lung parenchyma was healthy except an area immediately adjacent to the bullet, namely, a dilated sub-segmental peripheral bronchus telltale of the bullet track.
Most of the old inhaled, or aspirated FBs give rise to bronchiectasis and lung abscess, and mostly are not able to reach the respiratory bronchioles especially the narrow ones. Kürklü et al6 reported that although a patient was asymptomatic after FB aspiration, bronchiectasis was still observed. Steffensen et al’s7 study identified pleural effusionapart from obstructive emphysema, necrotizing pneumonia, and organizing pneumonia as the sequelae of FB aspiration. In another study, it was stated that a patient inhaled a rubber bullet, which was extracted after one year, but had episode of pneumonia, radio-graphically developed multiple areas of bronchiectasis and consolidations. After 2 months of extraction of the FB, the HRCT chest showed normal parenchyma of the lung.8
Our patient case was observed for postoperative complications, but remained well before discharge from hospital. We conclude that an incidental finding of an asymptomatic FB on chest x-ray does not necessarily mean that it is located in a recess of pleural space. It can be a silent lodged FB of the, lung especially if located in the peripheral zones.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 23, 2016.
- Accepted August 7, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.