


Abstract
Objectives To retrospectively evaluate the effectiveness of gastroesophageal stenting for post sleeve gastrectomy staple line leaks using removable self-expandable stents.
Methods Between April 2012 and June 2015, 12 consecutive patients (6 males) with mean age of 34 years: (21-38 years) presented with staple line leak 1-8 weeks after the operation (mean 2.8 weeks). Patients underwent gastroesophageal stenting by interventional radiology. A total of 23 stents were deployed with mean length of 17.8 cm (7-24 cm) and mean diameter 25.6 mm (18-36 mm). Stent re-insertion was needed in 7 patients (9 procedure), while 6 patients required percutaneous collection drainage and 3 patients required endoscopic glue injection with clipping. Two stent removal procedures were carried out under endoscopic visualization after failed stent capture under fluoroscopy, while the remaining stents were successfully removed by interventional radiology.
Results Stent placement was technically successful in all patients. Stent migration occurred in 6 patients (50%). There is a tendency for stent migration with shorter stent length (R= -0.557, p=0.008). The mean duration of stenting was 60.5 days (14-137 days). All patients underwent stent removal and resumed oral intake with no recurrence of leak at a mean follow up time of 190 days (14-410 days). Complications included gastrointestinal bleeding (n=1), proximal esophageal stricture (n=1) and stent occlusion (n=1).
Conclusion Gastroesophageal stenting as a primary measure after diagnosis of early post sleeve gastrectomy leak appears to offer a safe and effective alternative option in obviating repeat surgical interventions. Minimally invasive interventions may still be required for the management of persistent leak.
Post sleeve gastrectomy staple line leak occurs in approximately 1-5% of patients.1-4 Several endoscopic and surgical interventions have been implemented in treatment of post sleeve gastrectomy leaks depending on the time of diagnosis, size of leak and the presence of peritonitis.2,3,5-7 Gastroesophageal stents provide a barrier between the gastric contents and the staple line leak facilitating gradual healing while allowing for resumption of oral intake. Existing stents in the market include covered self-expandable metallic stents, partially covered self-expandable metallic stents, and covered self-expanding plastic stents. The overall reported success rate ranges between 80-95% when used for 6-12 weeks.5,7,8 This minimally invasive procedure is traditionally carried out under endoscopic guidance after visualization of the leak. In this study, we report techniques and clinical outcomes of esophageal stent placement and retrieval by interventional radiology.
Methods
The Institutional Review Board approved this retrospective study and patient’s consent form was waived. The inclusion criteria for this retrospective study were: a) patients who had sleeve gastrectomy complicated by post operative leak, b) patients who underwent esophageal stenting by interventional radiology. The exclusion criteria were: a) patients who were managed by surgical re-interventions, b) patients who underwent stenting by services other than interventional radiology, c) patients with missing clinical or imaging data, and d) patients who missed follow up.
Between April 2012 and June 2015, 12 consecutive patients (6 males) with a mean age of 34 years (21-38 years) were diagnosed with staple line leak 1-8 weeks after the operation (mean 2.8 weeks). No patients were excluded based on the exclusion criteria. Ten patients presented within 1-3 weeks after operation and 2 presented after 6 weeks. No patients were managed surgically prior to stent placement. Two patients were septic at the time of diagnosis. The remaining patients presented with chest infection (n=1) and upper abdominal pain associated with fever (n=9). Patients underwent gastroesophageal stenting by interventional radiology. A total of 23 fully covered self-expandable stents were deployed; PolyFlex® (Boston Scientific, Natick, MA, USA) (n=4); WallFlex® (Boston Scientific, Natick, MA, USA) (n=8); Hanarostent® (M.I.TECH, Gyeonggi-Do, Korea) (n=3), Niti-S™ (Taewoong Medical, Gyeonggi-Do, South Korea) (n=7); AliMaxx-ES (Alveolus® Inc., Charlotte, NC, USA) (n=1). The mean stent length was 17.8 cm (7-24 cm), and the mean diameter was 25.6 mm (18 30 mm).
Placement and retrieval procedures were preferably carried out under general anesthesia with nasotracheal, or orotracheal intubation. After cannulation of the esophagus, water-soluble contrast is injected in the distal esophagus to define the level and severity of leak. Intermittent oral and nasal suctioning is carried out to minimize the risk of aspiration. Once the duodenum is cannulated, the stent is introduced over a stiff guide wire without sheath to cover the area of leak. No post deployment balloon dilatation is performed (Figure 1). Post stenting feeding was resumed through nasojejunal tube or total parenteral nutrition, then liquid/solid oral diet was advanced as tolerated. Stent retrieval is carried out using a Raptor™ grasping device (US endoscopy, Mentor, Ohio) introduced through a 9 Fr sheath after placing a safety guide wire to maintain access after stent removal. The proximal edge of the stent is captured and removed along with the sheath through the mouth (Figure 2). Post removal esophagogram was carried out to check for persistent leak. Technical success is defined as successful sealing of the leak using the stent at the conclusion of procedure. Clinical success is defined as healing of the leak and resumption of oral intake at the time of follow up without the need for surgical intervention. Duration of stenting is the time between the initial stent placement and removal of the last stent. Follow up time is the time between removal of the last stent and last clinical follow up.

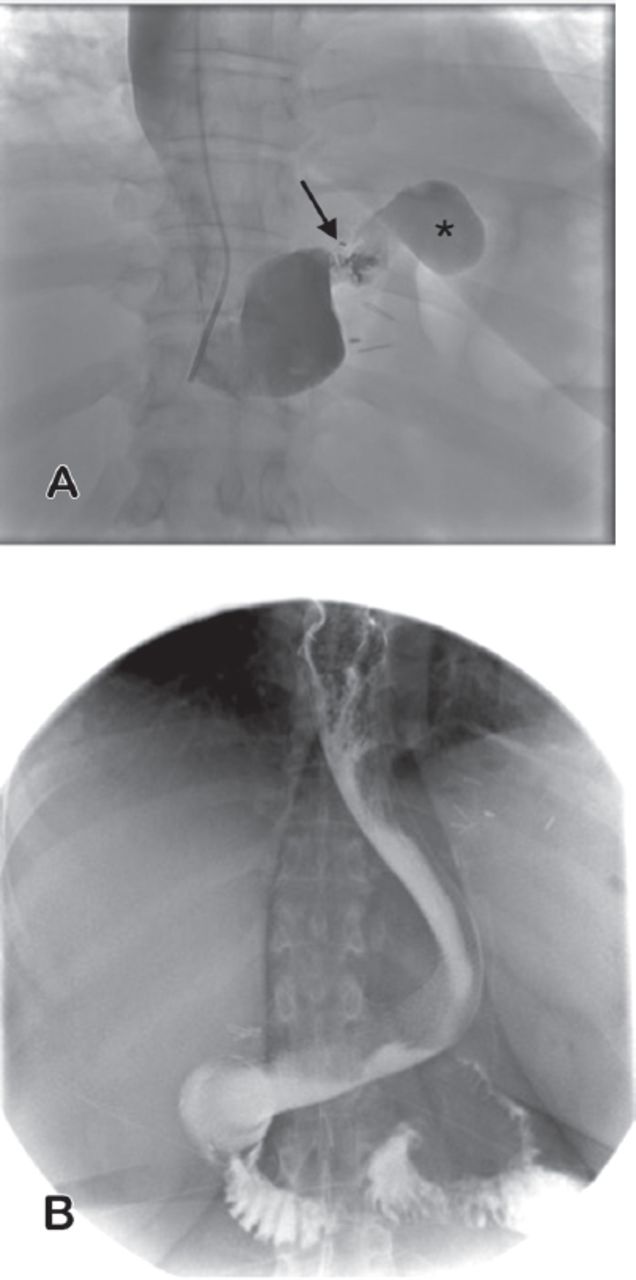
Esophagogram showing A) the initial proximal staple line leak (arrow) into a left subdiaphragmatic collection (asterisk) and B) follow up with stent in place with patent stent with no residual leak.
Linear Pearson correlation and univariate regression analysis was performed on Microsoft Excel® version 14.5.5 (Microsoft Corporation, Redmond, WA) supported by StatPlus:mac program Version 5 (AnalystSoft Inc., Walnut, CA, USA)

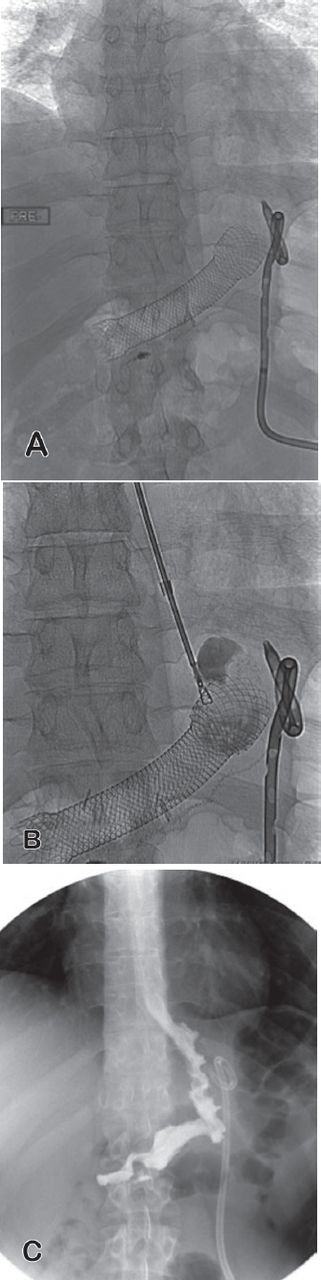
Control radiograph showing A) migrating esophageal stent into the gastric lumen. B) Intra procedural radiograph with a forceps capturing the proximal edge of the stent. C) Post removal esophagogram with no residual leak.
Results
Stent placement was technically successful in all patients. Asymptomatic stent migration occurred in 6 patients (50%). Migration occurred in cranial direction (n=1) and caudally (n=5). One stent migrated immediately after placement and required adjustment during the same session, while other stents migrated during follow up period. There is a tendency for stent migration with shorter stent length (R= -0.56, p=0.008). There is a weak negative correlation between migration and stent diameter (R= -0.47, p=0.03). The mean duration of stenting was 60.5 days (14-137 days). Patients reported no symptoms of stent intolerance or symptomatic reflux. No patients required additional surgical interventions. Nine stent re-insertion procedures were performed in 7 patients due to either stent migration (n=6) or persistent leak (n=5) after removal of the first stent. Additional interventions included percutaneous peri-gastric collection drainage in 6 patients. Endoscopic glue injection with clipping (n=3) was carried out due to persistent leak identified on esophagogram during stent removal earlier than 4 weeks. No subsequent endoscopic or surgical interventions. Two stent removal procedures were carried out under endoscopic visualization after failed stent capture under fluoroscopy, while the remaining stents were successfully removed by interventional radiology. One patient with Polyflex silicon covered stent required ballooning of the distal end of the stent as the stent was blocked against duodenal wall. One patient had an episode of upper GI bleeding post stenting with no identifiable source on endoscopy or angiography. Another patient had esophageal stricture at the proximal stent margin 6 months after stent removal, which required esophagoplasty with 16 mm esophageal balloon and 1 mm deep incisions at 4 quadrants under endoscopic guidance (Figure 3). All patients underwent stent removal and resumed oral intake with no recurrence of leak at a median follow up time of 190 days (14-410 days).

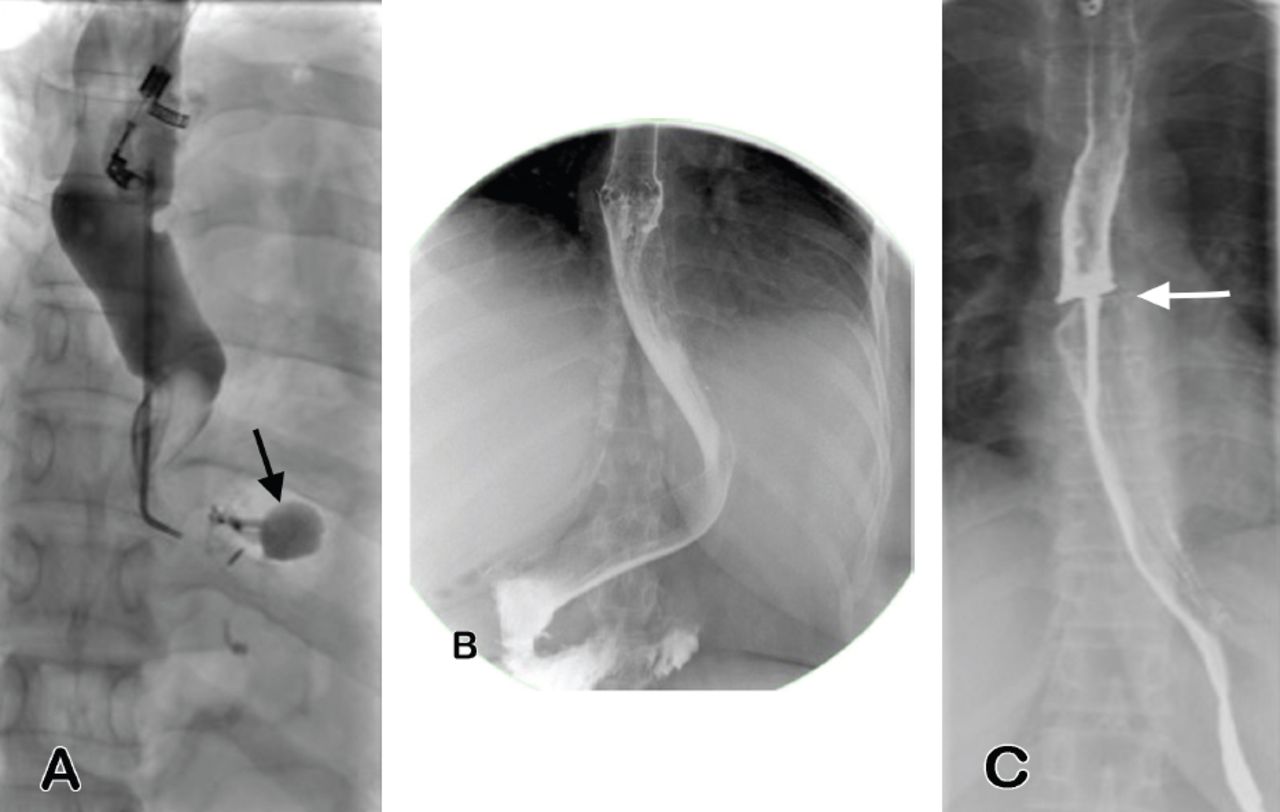
Esophagogram showing A) the proximal staple line leak (arrow), B) follow up 4 days following stent placement with patent stent with no residual leak, and C) 6 month follow up study post stent removal with high grade stricture at the level of the proximal stent margin (arrow).
Discussion
Despite increasing experience with laparoscopic sleeve gastrectomy and bariatric procedures, anastomotic and staple line leak continues to be a serious complication.1,3,9-11 While surgical interventions remain the mainstay in management of patients with symptomatic leak,3,10,12 covered stents are increasingly used as an effective adjunct method to isolate the leak from gastric contents and facilitate resumption of oral intake.2,3,5-8,10,12-21 According to the international sleeve gastrectomy expert panel consensus statement in 2012,11 leak is defined as acute <7 days, early 1-6 weeks, late 6-12 weeks, chronic >12 weeks. As majority agreed upon in the mentioned consensus document, stenting is a valid option for proximal acute or early leak as a primary management or after failed conservative treatment. In the absence of peritonitis or sepsis, early stent placement after diagnosis of gastric leak is associated with shorter healing time,8,12-14,17,18 while it has a limited role in the management of chronic leaks.3,11 In addition, smaller leaks are more likely to seal using covered stents in a shorter time compared to larger leaks. In a series of 19 patients, Nedelcu et al13 proposed the primary use of covered stents in patients who have early leak greater than 10 mm or for smaller leaks associated with stenosis. Using this algorithm, complete healing was achieved in all patients in average time of 3.4 months with no additional surgical interventions. However, time to complete healing was shorter in leaks smaller than 10 mm (2.8 month) compared to larger leaks (3.9 month). A retrospective review of stenting in 29 patients with acute staple line leak following sleeve gastrectomy (n=10) and a Roux-en-Y gastric bypass (n=19) showed a success rate of 96.5%.8 Primary stenting (with or without simultaneous surgery) resulted in shorter leak resolution time as compared to the secondary stenting (after surgical repair) (mean 50 versus 109 days, p=0.008).8 Based on findings of previous studies, the recommended duration of stenting varies between 4-12 weeks.14,17,18,21 In our cohort, the duration of stenting ranged between 2-20 weeks. Stent removal earlier than 4 weeks showed persistent leak and required either endoscopic glue injection with clipping or stent re-insertion.
Stent migration, which occurs in 15-60% of cases, is the most common complication that frequently requires re-intervention to maintain coverage of the leak.5,8,13,18 Migration occurred in our cohort in 50%, which was primarily linked to shorter stent length (<18 cm) and to a lesser extent to small stent diameter (<25 mm). While the use of partially covered stents is associated with less risk of migration, retrieval may become difficult requiring modified techniques due to tissue ingrowth and proximal mucosal injury.5,22 All stents used in this series were fully covered and there was no difficulty in the retrieval procedure.
Our study is inherently limited by its retrospective nature and small sample size that limit its statistical power. The use of different types of stents with variable diameter and length is an additional limitation. The duration of stenting also varied significantly among patients, which may affect the efficacy of stenting in management of leak. The exact fluoroscopy time for stent placement and retrieval procedures was not available in our archives.
In conclusion, stenting as a primary measure after diagnosis of early leak achieved successful healing in all patients. While minimally invasive interventions may still be required for management of stent migration or persistent leak, stenting appears to offer a safe and effective alternative option in obviating repeat surgical interventions.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received July 11, 2016.
- Accepted September 4, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.