


Abstract
Granulomatosis with polyangiitis (GPA) formerly called Wegener’s granulomatosis is a chronic necrotizing granulomatous inflammatory disease with systemic vasculitis involving the upper and lower respiratory tract, and kidneys. The typical histopathology is that of necrotizing granulomatous inflammation with palisading histiocytes, neutrophils, and lymphocytes. We report a case of a 57-year-old lady presenting with left eye swelling, left ear pain and discharge, but with no pulmonary or renal symptoms. Investigations revealed positive cytoplasmic antineutrophil cytoplasmic antibodies and proteinase 3 antibodies. The CT and MRI showed meningeal thickening and bilateral structural changes of the orbits and mastoids. Lacrimal gland biopsy showed non necrotizing granulation with an eosinophilic infiltration. She was diagnosed with eosinophilic variant of GPA of the eyes and mastoid bones bilaterally extending to dura and sparing the lungs and kidneys. She responded to corticosteroids and rituximab.
Granulomatosis with polyangiitis (GPA) formerly called Wegener’s granulomatosis (WG) is a chronic necrotizing granulomatous inflammatory disease with systemic vasculitis, particularly involving the upper and lower respiratory tract and kidneys. Typically, the biopsy shows vasculitis, necrosis, and granulation. It might present as the limited form involving the head and neck, but with no pulmonary or renal involvement. Regular GPA (with no tissue eosinophilia) can affect the orbits and mastoids unilaterally or bilaterally.1 A few cases are reported as an eosinophilic variant forms of GPA with peripheral or tissue eosinophilia of the upper and lower respiratory tract, but with no involvement of the orbits or the mastoids.2-7 The involvement of the orbit by a variant form of GPA with peripheral or tissue eosinophilia was reported only once.8 However, there are no reports of the involvement of both the orbits and the mastoids by eosinophilic infiltrations in GPA. Herein, we report a case of the eosinophilic variant of GPA involving both the orbits and mastoids bilaterally with histopathological features of eosinophilic inflammation of orbits, and mastoid bones with extension to the dura matter. The absence of asthma and atopy, and the presence of typical features of GPA, proteinase 3 (PR3)-antineutrophil cytoplasmic antibodies (ANCA) make the diagnosis of eosinophilic variant GPA more likely than eosinophilic granulomatosis with polyangiitis (EGPA) formerly called Churg-Strauss syndrome (CSS).6,7,9 Our objective in presenting this particular case is to highlight the rare existence of an eosinophilic variant of GPA involving both the orbits and mastoids bilaterally with histopathological features of eosinophilic inflammation of orbits, mastoid bones with extension to the dura matter, which is reported here for the first time.
Case Report
A 57-year-old lady presented to the local hospital with left eye swelling and left ear pain and discharge. Swelling of the left upper eye lid started insidiously and progressed over one month to involve the peri-orbital regions of both eyes accompanied by redness and pain of the involved areas. She started to have pain and swelling of both ears with yellowish thick discharge. She had a history of fever, arthralgia and myalgia for one month. She had no dyspnea, cough, hemoptysis, or hematuria. She has no past or present history of asthma or atopy. History included diabetes mellitus for the preceding 20 years on mixtard insulin, and hypertension for more than 20 years on lisinopril 10 mg daily. On examination, her vital signs were normal. However, both eyes were swollen in addition to a swelling at the left mastoid area. No mucocutaneous abnormalities were observed. Chest examination was normal. Complete blood count, renal function tests and urinalysis were normal. Cytoplasmic anti neutrophil cytoplasmic antibodies (C-ANCA) and PR3 antibodies were both positive. Rheumatoid factors and anti-cyclic citrillinated peptide antibodies were both negative. Cultures of blood and body tissues showed no growth. A CT of the left orbit showed diffuse thickening of lateral and superior recti muscles of the eyes with affection of lacrimal gland (Figures 1A & 1B). An MRI revealed left sided exophthalmos, poorly defined soft tissue intensity mass at the superior and lateral extra-coronal compartment of left orbit and complete opacification of the left mastoid bone air cells with dural involvement on the left side, and similar findings in the right orbit and mastoid bone although to a lesser degree (Figures 2A & 2B). Biopsy of the lacrimal gland from the left eye showed angiocentric necrotizing granulomatous vasculitis with extensive eosinophilic infiltrates (Figures 3A & 3B). Surgical excisional biopsy from the left mastoid process revealed necrosis, fibrosis, and granulation tissue. The diagnosis of an eosinophilic variant of GPA was made. She was started on intravenous methylprednisolone 30 mg twice daily for one week, then shifted to oral prednisolone 30 mg twice daily. This was gradually tapered to a dose of 5 mg daily, and stopped over a period of 6 months. However, upon stopping prednisolone her disease flared up again in the same sites. It was decided to start her on rituximab once intravenously, which was repeated after 2 weeks in addition to prednisolone 30 mg once daily for one month and then tapered over 2 months to zero. This lead to resolution of signs and symptoms and tradiological findings with remarkable resolution of soft tissue thickening around the lateral aspects of the left orbit (Figure 4).

Photograph showing: A) Axial CT sections without contrast through orbits showing varying levels of ill-defined soft tissue thickening surrounding the lateral rectus muscle on left side and the superior recti muscles. B) Coronal CT sections without contrast through orbits show varying levels of ill-defined soft tissue thickening around the lateral aspects of the left orbit surrounding the lateral rectus muscle and also extending into intraconal fat, superior rectus muscle and lacrimal gland.

Photograph showing: A) Coronal high resolution T2 weighted image (1) demonstrating increased signal intensity in the soft tissue along lateral aspect of the left orbit. T1 weighted image (2) shows corresponding decreased signal intensity. Post contrast T1 weighted images (3,4) show enhancement in the abnormal orbital soft tissue. Minimal similar abnormalities are seen in the right orbit as well. There is also abnormal meningeal thickening and enhancement along the base and lateral aspect of the cerebral hemisphere. B) Axial post contrast T1 weighted images (5,6) show enhancement of the abnormal soft tissue as well as abnormal thickening and enhancement of the dura on left side. Axial pre contrast T1 weighted image (7) shows ill-defined soft tissue thickening around the lateral aspect of the left orbit.

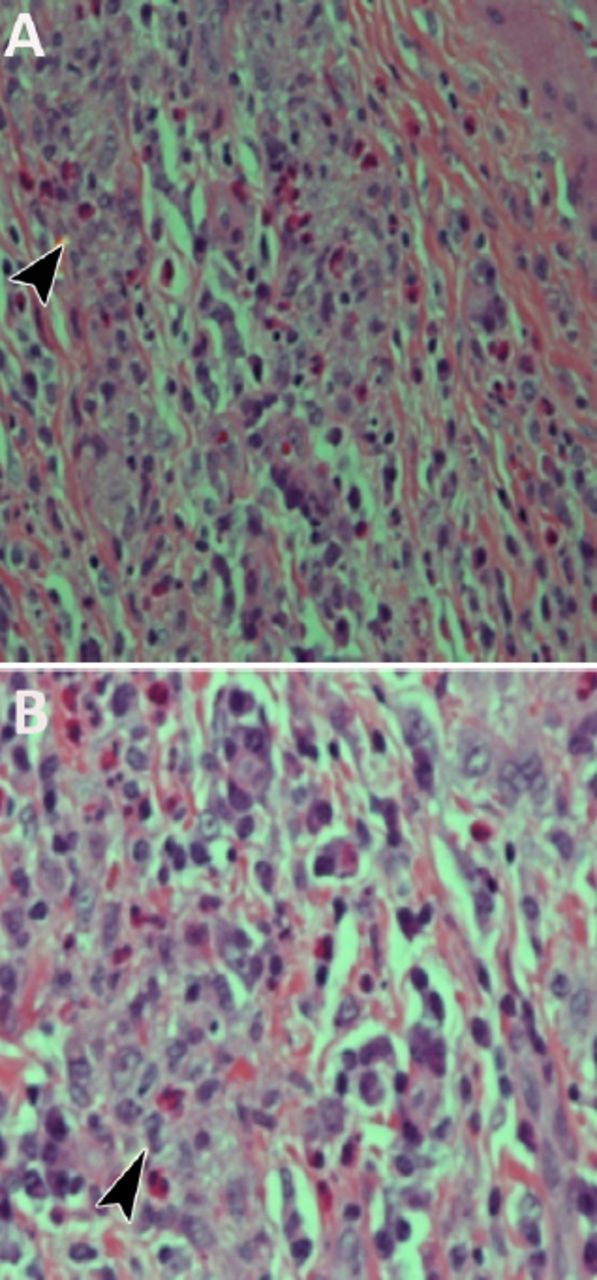
Photograph showing: A) Lacrimal gland biopsy shows granulation, medium sized vessel wall infiltrated by eosinophils (arrow head) and plasma cells. The lumen of the vessel is obliterated by similar cells and there are newly formed vessels (hematoxylin and eosin stain X400). B) Lacrimal gland biopsy shows eosinophilic granuloma. The arrow head points to an aggregate of histiocytes. There are numerous plasma cells at the periphery (hematoxylin and eosin stain X600).

Discussion
Ocular involvement in regular GPA, can be the initial manifestation of disease, and can result in significant morbidity and possibly blindness.1,10 The infiltrating inflammatory cells include neutrophils, lymphocytes, multinucleated giant cells, and the very occasional eosinophil. In 1986, Henochowicz et al2 described a GPA patient whose nasal biopsy-demonstrated eosinophilic vasculitis and renal biopsy-demonstrated necrotizing glomerulonephritis with tissue eosinophilia. In 1988, Yousem and Lombard3 were the first to coin the term eosinophilic variant of GPA when they described 4 cases of an unusual histological variant of GPA, diagnosed by open lung biopsy which showed granulomatous vasculitis and intense stromal eosinophilia in the absence of peripheral blood eosinophilia or clinical asthma.3 All 4 cases fall within the spectrum of GPA, all 4 patients had involvement of the upper respiratory tract, but not the orbits or the mastoids. All 4 patients had chest radiographic abnormalities and necrotizing granulation in lung biopsies, but in contrast to regular GPA cases they were characterized by prominent tissue infiltrate of eosinophils. In addition, a few cases were reported as a variant form of GPA with peripheral, or tissue eosinophilia, but with no involvement of the orbits, or the mastoids.4-7 Eosinophilic granulomatosis with polyangitis (EGPA) formerly called Churg-Strauss syndrome (CSS) is typically associated with tissue eosinophilia and vasculitis, but is differentiated from eosinophilic variant GPA by the clinical history of atopy or asthma. Asthma and atopy are rare in GPA, occurring no more frequently than in the general population. Chan et al8 in 2011 described an eosinophilic variant of WG occurring in the orbit in association with local IgE production with biopsy of left orbital mass showing marked infiltration of tissue by eosinophils.
In our case, the patient had orbital and mastoids involvement with extension to dura, and sinusitis. Cytoplasmic anti neutrophil cytoplasmic antibodies and PR3 antibodies were positive and tissue biopsy from the left lacrimal gland showed necrotizing granuloma with massive infiltration of eosinophils. The tissue eosinophils could not be attributed to EGPA (CSS) because the patient had no history of bronchial asthma, and pulmonary function tests were normal with no peripheral eosinophilia. Another entity in the differential diagnosis of tissue eosinophilia is eosinophilic angiocentric fibrosis, which is a rare inflammatory disease involving the sino-nasal tract with tissue eosinophilia and distinctive perivascular fibrosis. It is differentiated from eosinophilic WG by the absence of necrosis. Fungal and parasitic infections were excluded by histopathologic analysis and tissue cultures. In addition to all of the above, the presence of C-ANCA and PR3-ANCA would make the most likely diagnosis in our case that of an eosinophilic variant of GPA.9
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received February 29, 2016.
- Accepted April 20, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.