


Abstract
Objectives: To investigate the effectiveness of oxycodone compared with fentanyl for attenuating the hemodynamic response during endotracheal intubation.
Methods: This study was conducted from June 2014 to February 2015 on healthy adults undergoing general anesthesia at the Yeungnam University Hospital, Daegu, Republic of Korea. Ninety-five patients were randomly assigned to one of 3 groups to receive the following drugs; Group F: fentanyl 2 µg/kg; Group O/70: oxycodone 140 µg/kg; Group O/100: oxycodone 200 µg/kg. Five minutes after injection of the study drug, general anesthesia was induced with propofol 1.5 mg/kg and rocuronium 0.8 mg/kg. The mean blood pressure (MBP), heart rate (HR), peripheral oxygen saturation (SpO2), and bispectral index (BIS) were compared before administration of the study drug (T1), just before endotracheal intubation (T2), one minute after endotracheal intubation (T3), and 7.5 minutes after endotracheal intubation (T4). Complications were assessed.
Results: The 2 oxycodone groups showed no significant differences in MBP, HR, SpO2, and BIS compared to Group F at the time points assessed. The incidence of complications was comparable among the groups.
Conclusions: Oxycodone could successfully be used to attenuate the sympathetic response during anesthetic induction. The hemodynamic profiles and incidence of complications were clinically similar among the groups, but Group O/70 tended to show a lower rate of complications of apnea.
Laryngoscopy and endotracheal tube insertion are accompanied by elevations in blood pressure (BP) and heart rate (HR) as a result of sympathetic stimulation. The response increases and reaches its maximum level within one minute and ends within 5−10 minutes after intubation.1 These changes in BP and HR are well tolerated by healthy individuals; however, they may be fatal in patients with cardiovascular diseases or those with increased intracranial pressure. Opioids, a2-agonists, b-blockers, vasodilators, lidocaine, or magnesium sulfate have been used to reduce these hemodynamic responses.2-8 The effectiveness of these drugs to blunt sympathetic stimulation has been found to be quite different throughout medical literature, because it was studied in different settings in relation to dose or route of drugs or type of surgery. Among the opioids, medications with rapid onset such as fentanyl have been commonly used for this purpose.1,9 In the relevant studies with fentanyl, the optimal dosage and time of administration to successfully attenuate the sympathetic response was found to be 2 µg/kg at 5 minutes prior to endotracheal intubation.10 Recently, oxycodone has been used for the control of chronic pain, cancer pain, or post-operative pain in the form of intermittent intravenous (IV) injections or patient-controlled analgesia.11-13 However, its potency has not yet been accurately determined, and most studies show the conversion ratio of oxycodone versus morphine as 1:1. The potency ratio between fentanyl and oxycodone has not been investigated clearly and is simply assumed to be 1:100. However, some studies comparing postoperative pain scores concluded that the potency ratio of fentanyl to oxycodone might be approximately 1:75 or that oxycodone might be more potent than morphine (4:3).12,13 There have been no previous studies that have investigated the use of oxycodone to reduce the hemodynamic response during endotracheal intubation. So far, the effects of oxycodone and its optimal dosage during endotracheal intubation have not been studied. Therefore, we investigated the action and side effects during endotracheal intubation of IV oxycodone 140 µg/kg (1:70) or 200 µg/kg (1:100) compared to fentanyl 2 µg/kg.
Methods
This prospective, randomized, double-blind designed study was carried out between June 2014 and February 2015 at the Yeungnam University Hospital, Daegu, Republic of Korea in accordance with the principles of the Helsinki Declaration and after obtaining approval of the study from the institutional ethics committee and written informed consent from participants. Ninety-five patients, 18-65 years old, the American Society of Anesthesiologists (ASA) physical status 1-2, undergoing general anesthesia, were included in this study. Exclusion criteria included heart disease, hypertension, diabetes, severe obesity (body mass index >30), history of difficult intubation, or predicted difficult airway.
The patients were randomized using a computer randomization program into one of 3 groups: Group F: fentanyl 2 µg/kg (Fentanyl®, Myungmun, Korea), Group O/70: oxycodone (Oxynorm®, Mundipharma, UK) 140 µg/kg (1:70), Group O/100: oxycodone 200 µg/kg (1:100). Two anesthesiologists conducted the study. One was responsible for preparing the study drug, and the other for performing the anesthesia and assessing the side effects. Both the assessor and patients were blind to the group allocations and were not informed of the block size until the end of the study. Oxycodone and fentanyl were prepared in 10 mL syringes, and normal saline was added to a final volume of 5 mL to create an identical appearance. Then, the drugs were consecutively injected to each patient according to the randomization schedule.
Midazolam 0.03 mg/kg was IV injected into the patients for premedication in the preoperative holding area. In the operating room, routine monitoring devices were applied including electrocardiography (ECG), non-invasive BP, pulse oximetry, and bispectral index (BIS). After confirmation of baseline vital signs, the study drug was injected and the patients were carefully monitored for 5 minutes. During this period, patients were assessed for complications of opioid administration, particularly respiratory depression, hypotension, bradycardia, dizziness, chest stiffness, and pruritus. After that, propofol 1.5 mg/kg and rocuronium 0.8 mg/kg were injected to facilitate endotracheal intubation. Oxygen and air (FiO2 0.5) were delivered during the induction period. After the achievement of deep neuromuscular block confirmed by train of Four (TOF) monitoring, endotracheal intubation was performed, and sevoflurane 1.5% was added. If systolic BP (SBP) increased >150 mm Hg after intubation, sevoflurane was increased 0.5% in a timely manner and BP was rechecked every 2.5 minutes. Vital signs including SBP, diastolic BP (DBP), mean BP (MBP), HR, SpO2, and BIS were recorded before administration of the study drug (T1), just before intubation (T2), one minute after intubation (T3), and 7.5 minutes after intubation (T4). In case of hypotension (SBP <90 mm Hg), or bradycardia (HR <60 beats per minute [bpm]), ephedrine 4 mg, or atropine 250 µg, respectively, were injected. When hypertension (SBP >180 mm Hg), or tachycardia (HR >120 bpm) occurred, nicardipine (Perdipine®, Astellas Korea, Seoul, Korea) 500 µg or esmolol (Brevibloc®, Jeil Pharmaceutical Co., Ltd., Seoul, Korea) 20 mg, respectively, were administrated. Hypoventilation was defined as SpO2 <90% during the 5 minutes after study drug administration, and when it occurred, the patient was encouraged to breathe deeply. If oxygen saturation did not recover, oxygen supply via face mask or manual assistance with ventilation was applied, as needed.
This prospective investigation was performed as a preliminary study because there were no previous reports about the use of oxycodone as an adjuvant to tracheal intubation. An effect size of 0.38 and a sample size of 24 participants per group were found to provide a 10% difference in MBP at one minute after tracheal intubation with a power of 0.8 and a type one error of 0.05. In consideration of a dropout rate of about 10%, 95 patients were enrolled in this study. Data was computed and analyzed by using Statistical Package of Social Sciences Version 18.0 (SPSS Inc., Chicago, IL, USA). Repeated measures analysis of variance (ANOVA) were used to analyze MBP, HR, SpO2, and BIS, and the Bonferroni procedure was used for post hoc testing. Categorical data was analyzed with the chi-square test and continuous variables were analyzed using one-way ANOVA. A value of p<0.05 was considered statistically significant.
Results
Of the 95 patients enrolled, 2 patients were excluded because of protocol violations. The analysis was performed on the remaining 93 patients, and there were no demographic differences among the groups (Table 1). There were no differences in basal hemodynamic parameters among the 3 groups.
Demographic data on 93 healthy adults undergoing general anesthesia at the Yeungnam University Hospital, Daegu, Republic of Korea.
Mean blood pressure (MBP)
Mean blood pressure decreased after the administration of study drugs and induction agents, then increased immediately to reach a level around baseline after intubation, and subsequently declined progressively in all study groups. The oxycodone groups showed a more suppressed trend regarding MBP than Group F throughout the study period, but there were no significant differences among the groups. There were significant differences in all 3 groups in the values between the following time points: T1 and T2 (p=0.000), T1 and T4 (p=0.000), T2 and T3 (p=0.000), T2 and T4 (p=0.000), and T3 and T4 (p=0.000), but no differences were found at T1 and T3 (p=1.000) (Figure 1).

Changes in mean blood pressure (MBP) in each group during study period (mean ± standard deviation [SD]). Group F: fentanyl (2 µg/kg), Group O/70: oxycodone 140 µg/kg, Group O/100: oxycodone 200 µg/kg. T1 = baseline, T2 = just before intubation, T3 = one minute after intubation, T4 = 7.5 minutes after intubation. MBP showed no significant difference among the 3 groups at all periods of induction.
Heart rate (HR)
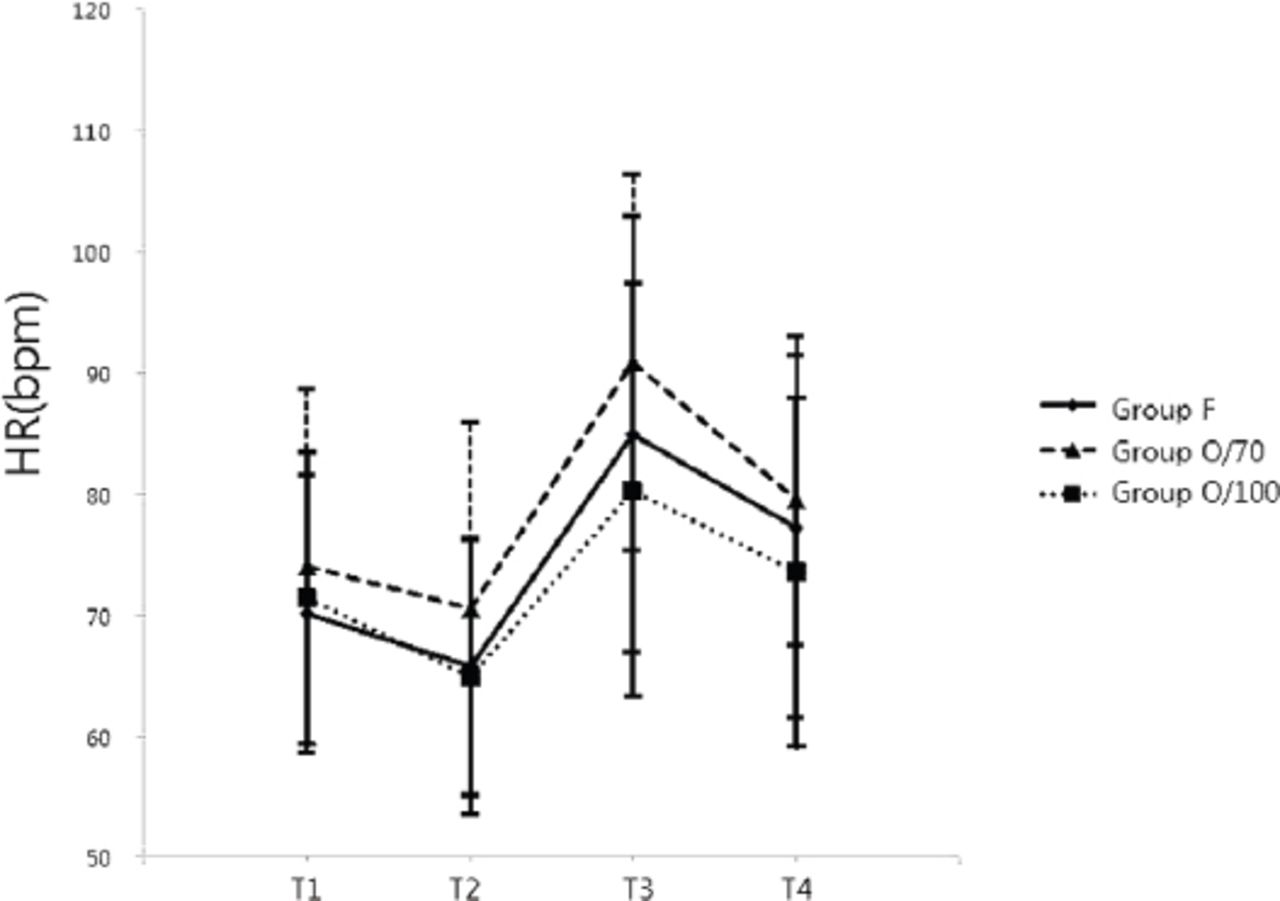
Compared to baseline, HR decreased just before intubation and peaked at T3 and then decreased progressively in all study groups. The trend of Group O/70 showed a less depressed pattern than that of Group F, while Group O/100 showed a more depressed pattern than that of Group F, even though there were no significant differences between each of the 2 groups. There were significant differences in the values assessed at T1 and T2 (p=0.000), T1 and T3 (p=0.000), T1 and T4 (p=0.004), T2 and T3 (p=0.000), T2 and T4 (p=0.000), and T3 and T4 (p=0.000) in all 3 groups (Figure 2).

Changes in heart rate (HR) in each group during study period. Group F: fentanyl (2 µg/kg), Group O/70: oxycodone 140 µg/kg, Group O/100: oxycodone 200 µg/kg. T1 = baseline, T2 = just before intubation, T3 = one minute after intubation, T4 = 7.5 minutes after intubation. A significant difference was noted between Group O/70 and Group O/100 at T3 (p=0.04).
Peripheral oxygen saturation (SpO2)
Peripheral oxygen saturation in Group O/70 increased immediately during anesthetic induction and then leveled off, while the other groups showed gradual increases. There were significant differences in time between T1 and T2 (p=0.000), T1 and T3 (p=0.000), and T1 and T4 (p=0.000), but no significant differences at T2 and T3 (p=1.000), T2 and T4 (p=0.447), and T3 and T4 (p=1.000) in all 3 groups. No significant differences were found among the groups (Figure 3).

Changes in peripheral oxygen saturation (SpO2) in each group during study period. Group F: fentanyl (2 µg/kg), Group O/70: oxycodone 140 µg/kg, Group O/100: oxycodone 200 µg/kg. T1 = baseline, T2 = just before intubation, T3 = one minute after intubation, T4 = 7.5 minutes after intubation. SpO2 showed no significant difference among the groups.
Bispectral index
Anesthetic induction decreased BIS to approxiamtely the 40s in all groups, and then the values leveled off. Bispectral index was comparable in all groups. There were significant differences in time between T1 and T2 (p=0.000), T1 and T3 (p=0.000), T1 and T4 (p=0.000), T2 and T3 (p=0.000), and T2 and T4 (p=0.000), but no significant differences at T3 and T4 (p=1.000) (Figure 4).

Changes in bispectral index (BIS) in each group during study period. Group F: fentanyl (2 µg/kg), Group O/70: oxycodone 140 µg/kg, Group O/100: oxycodone 200 µg/kg. T1 = baseline, T2 = just before intubation, T3 = one minute after intubation, T4 = 7.5 minutes after intubation. BIS was comparable in all groups.
Side effects
The incidence of side effects such as hypotension, hypertension, tachycardia, and bradycardia during the study period is shown in Table 2. The incidence of all side effects was comparable, but one patient in Group O/100 showed a decrease in HR to 22 bpm at T2, and was successfully treated with 0.5 mg of IV atropine. The incidence of hypoventilation was lower in Group O/70 (n=7) compared to Group F (n=12) and Group O/100 (n=13), but there was no significant statistical difference. The total incidence of side effects was comparable among the groups.
Incidence of side effects on 93 healthy adults undergoing general anesthesia at the Yeungnam University Hospital, Daegu, Republic of Korea.
Discussion
There had been no previous studies that compared the effectiveness of IV oxycodone and fentanyl to reduce the hemodynamic response during endotracheal intubation. In the current study, the hemodynamic responses of the 3 drug regimens were similar, and the incidence of complications was also comparable. Endotracheal intubation and laryngoscopy are almost always accompanied by increases in BP and HR, so various medications have been used to blunt such stimulations. However, no agent has yet been revealed to be superior to the others, and they are used in combination according to patients’ physical status. Opioids are widely used for this purpose, but they are often accompanied by hypotension before intubation or during surgical draping. Hypotension after the administration of induction agents pushes anesthesiologists to perform hasty intubation. If sufficient muscle relaxation is not achieved, intubation could cause vocal cord contractions or injury.14 Also, hypotension often appears during the time between endotracheal intubation and the initiation of surgery; therefore, induction agents should have adequate hemodynamic profiles during the entire period of anesthetic induction. In the current study, MBPs were all above 60 mm Hg, even during the anesthetic induction, and the overall difference showed no statistical significance among the groups. There were no significant differences in complications among the groups; therefore, we conclude that oxycodone has clinically similar hemodynamic effects to those of fentanyl during induction of general anesthesia, both in 1:70 and 1:100 ratios.
Although the difference was not significant in this study, the overall trend showed lower MBP in the oxycodone groups. The reason is unclear but we hypothesized 3 possible explanations. First, the synergistic effect of propofol and oxycodone might be higher than that of propofol and fentanyl. Second, histamine released by oxycodone might induce decreased MBP. The potency of opioids has been compared in many studies with pain scores, not by hemodynamic profiles. For instance, as oxycodone does not release significant amounts of histamine, as morphine does, oxycodone has been found to decrease BP less than morphine at equianalgesic doses.11,15 However, fentanyl belongs to the piperidine group and does not produce histamine release.16 This may contribute to the MBP difference even at equianalgesic doses of oxycodone and fentanyl. Third, oxycodone exhibits effects by binding the µ-opioid receptor, like other opioids. However, in animal studies, oxycodone has been revealed to have an additional antinociceptive profile through the k-receptor, which is located prudently on peripheral nerves.17 K-receptor agonists, U-50 and 488H, have been reported to decrease left systolic peak pressure and HR in isolated rat hearts, which was not antagonized with naloxone.18 And another k-receptor agonist, dynorphin, has been reported to decrease mean arterial pressure and dilate the superior mesenteric artery.19 That might affect MBP in both oxycodone groups even though there is no significance. Oxycodone is a semi-synthetic opioid analgesic derived from the naturally occurring alkaloid, thebaine.17 Its onset is similar to that of fentanyl (2-3 min after IV injection) and its duration of action is slightly longer (t1/2: 4 hours 52 min versus 3 hours 39 minutes).12 As the k-receptor is associated with visceral pain, the effect of oxycodone is better than that of morphine in intra-abdominal surgery.13 Also, in a comparison of oxycodone and fentanyl in postoperative pain control after laparoscopic cholecystectomy, 15 mg of oxycodone showed better analgesic effect than 200 µg of fentanyl.12 These findings suggest that the potency ratio between oxycodone and fentanyl is not 1:100 in surgeries involving visceral pain.12
Study limitations
Subjectively, complications were assessed by incidence rather than by severity. For instance, in one patient in Group O/100, manual ventilation was required to recover saturation from 66-90% SpO2. The patient needed several stimulations or interventions to maintain SpO2 over 90%, but this result was interpreted as the same as desaturated patients who recovered oxygen saturation over 90% by a single stimulation only. In other words, only incidence but not magnitude of desaturation was assessed in this study. Also, dizziness, chest discomfort, and pruritus were assessed, but could not be considered in the results because the responses were not definite. Patients who were moderately sedated may have been confused or failed to answer the questions regarding these side effects. A high percentage of these patients belonged to Group O/100, even though BIS was comparable among the groups. Therefore, assessing unpurposed behaviors may have resulted in significant differences. Further studies are needed to establish the respiratory complications of oxycodone during the anesthetic induction period.
In conclusion, oxycodone could be successfully used to attenuate the sympathetic response during endotracheal intubation as effectively as fentanyl. Although the exact conversion ratio between fentanyl and oxycodone could not be determined in this study, both 140 µg/kg and 200 µg/kg of oxycodone provided stable MBP during anesthetic induction.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received February 29, 2016.
- Accepted June 2, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.