


Abstract
Laryngocele is an uncommon condition that represents a benign dilatation of the laryngeal saccule with air and/or fluid, arising in the region of the laryngeal ventricle. Laryngoceles, or laryngomucocele can be classified as internal, or combined. The aim of presenting this rare case of a bilateral combined laryngocele, are to emphasize the importance of diagnostic laryngoscopy in upper airway pathologies evaluation, increase awareness in the general otolaryngologist community, and to highlight the external surgical method.
Laryngocele, or laryngomucocele is an uncommon condition that represents a benign dilatation of the laryngeal saccule with air and/or fluid, arising in the region of the laryngeal ventricle.1 They were first described by Dr. Dominique Jean Larrey, surgeon-in-chief of Napoleon’s army in Egypt in 1829, and then better characterized by Rudolf Virchow in 1867.1 Laryngoceles can be classified as internal, or combined; purely external laryngoceles cannot exist as laryngoceles originate in the laryngeal saccule.2 An internal laryngocele is limited to the anatomic boundaries of the larynx and appears like a mass in the false vocal cord; a combined laryngocele extends upwards and protrudes through the thyrohyoid membrane.3 The cause of their occurrence is still not well understood.4 The incidence of laryngoceles is estimated to be one per 2.5 million of the population per year, and they have been reported to occur more frequently in men than women, with a peak incidence between the ages of 50 and 60 (85% are unilateral and 15% bilateral).5 Clinically, laryngocele could be present with dysphonia, airway obstruction, and difficulty in swallowing.6 The management of combined laryngocele is still a controversial subject, with the options being endoscopic and external surgery.7 Our objectives in presenting this case, a rare case of a bilateral combined laryngocele, are to emphasize the importance of diagnostic laryngoscopy in upper airway pathologies evaluation, increase awareness in the general otolaryngologist community, and to highlight the external surgical method which was used in the treatment.
Case Report
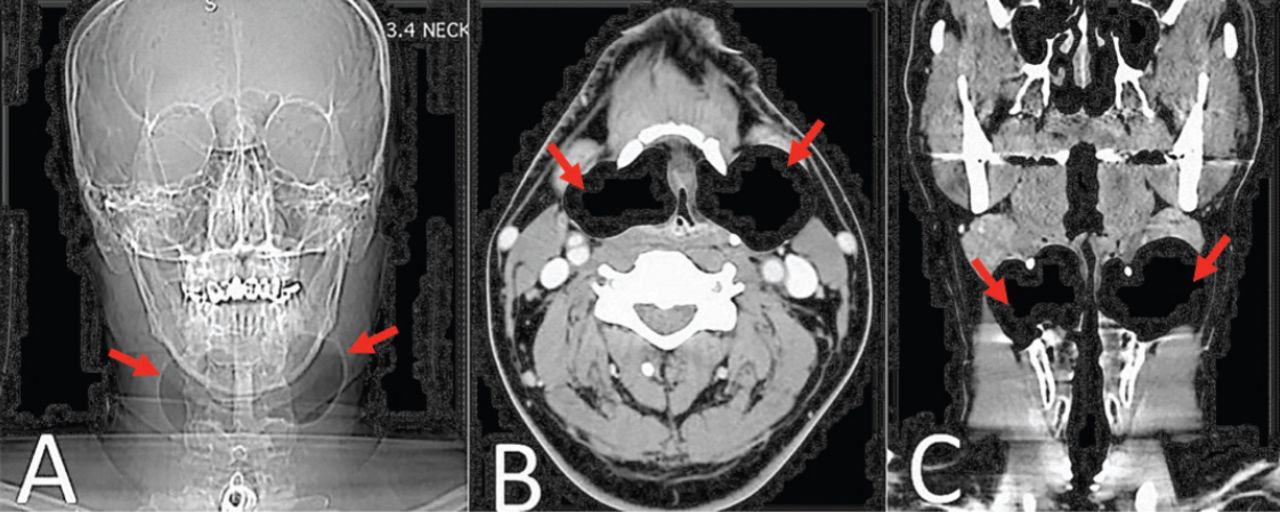
A 57-year-old, male patient presented with hoarseness, shortness of breath, and bilateral neck mass for 3 months. There was no history of fever, night sweats, weight loss, loss of appetite, fatigue, or head and neck cancer. He has been a heavy smoker (2 packs per day) for 40 years. He is a type-II diabetic, but using insulin and has history of cervical tuberculous lymphadenopathy 20 years ago, treated with triple medication for 9 months. Examination showed that he has a moderate stridor. Neck examination showed bilateral neck mass, mobile, non-tender, and soft, not attached to skin, or underlying tissue. His plain soft tissue neck x-ray and CT scan confirmed bilateral laryngoceles (Figure 1). He underwent elective tracheostomy under local anesthesia followed by laryngeal multiple biopsies from the swollen mucosa; although not clinically suspicious, to rule out underlying hidden malignancy. Surgical excision of bilateral combined laryngoceles was carried out with an external approach with trans thyrohyoid membrane approach, combined with V-shaped thyrotomy to improve exposure (Figure 2). No malignancy was identified in the final pathology.
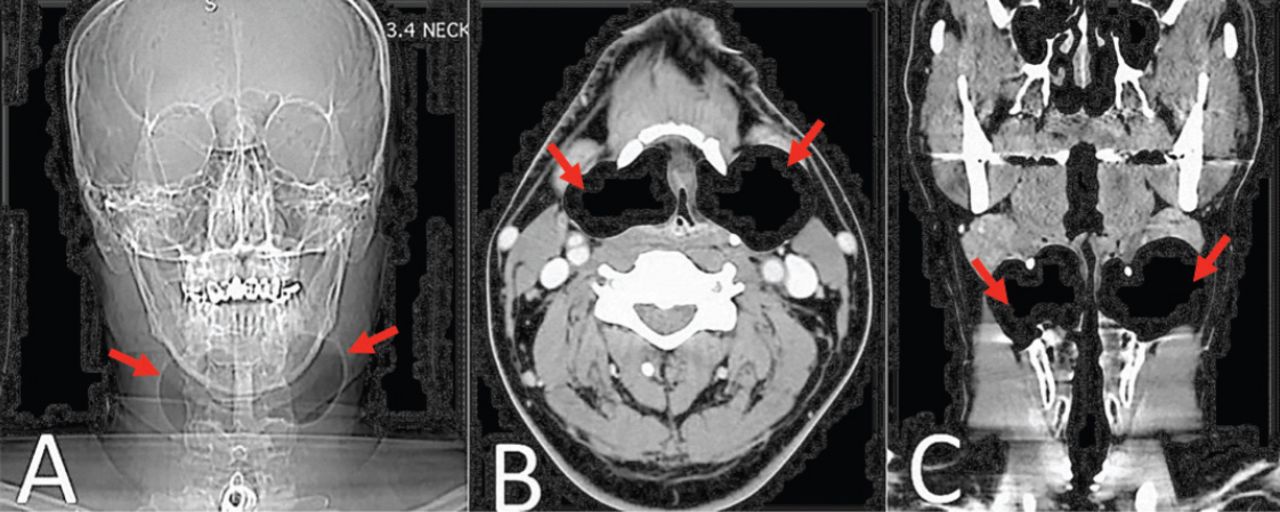
Image showing A) a plain soft tissue x-ray of the neck showing the shadow of the bilateral laryngocele. B) axial and C) coronal CT scan section of larynx confirmed bilateral combined laryngocele. Red arrows points to the laryngoceles

Clinical photos showing the A) preoperative laryngoscopy showed significant airway compromise, B) preoperative planning, and C) intraoperative exposure of left laryngocele.
Discussion
Laryngoceles are dilations of the laryngeal saccule within the ventricle of Morgagni. They have been reported to be 5 times more frequent in men than in women, with a peak incidence in the sixth decade. Eighty-five percent of laryngoceles were found to be unilateral.5 The case presented here is also a man in his sixth decade, but he had bilateral combined laryngoceles, which is a rare situation. Zelenik et al2 presented a systemic review of 50 articles in 2014; 63 patients with laryngoceles were included. There are a total of 8 bilateral laryngoceles reported in the literature.2 A combined laryngocele extends upwards and protrudes through the thyrohyoid membrane to the neck. If the neck of the laryngocele becomes obstructed this will lead to laryngomucocele, and if it becomes infected, to laryngopyocele.8 Laryngocele may interfere in speech and cause snoring or hoarseness, shortness of breath, or even upper airway obstruction as in the case hereby presented.9
The diagnosis of laryngocele is based on clinical findings, endoscopic examination of the larynx, and imaging studies. It should be noted that all patients with upper airway problems should undergo endoscopic evaluation to ascertain the diagnosis.5 Laryngeal MRI, or CT can be used: laryngoceles appear as air- or fluid-filled cystic dilatations. In smokers, one has to think on the possible underlying malignancy and CT, or MRI imaging is mandatory.10 The differential diagnosis of laryngocele includes saccular cyst, branchial cyst, neck abscess, and lymphadenopathy. It should be noted that saccular cysts usually present in younger age groups, do not communicate with the laryngeal lumen, and are usually filled with fluid.5 Various modalities of treatment have been used for laryngocele resection, with an external approach being the traditional treatment method. The latest consensus for laryngocele treatment favors an external approach for large, or external laryngoceles as presented in this patient, and endoscopic resection for internal laryngoceles.3,4,7
In conclusion, although combined laryngocele is rare, it should still be remembered in the differential diagnosis of upper airway problems, alongside the importance of endoscopy and imaging in reaching a definitive diagnosis in such cases.
Case Reports
Case reports will only be considered for unusual topics that add something new to the literature. All Case Reports should include at least one figure. Written informed consent for publication must accompany any photograph in which the subject can be identified. Figures should be submitted with a 300 dpi resolution when submitting electronically. The abstract should be unstructured, and the introductory section should always include the objective and reason why the author is presenting this particular case. References should be up to date, preferably not exceeding 15.
Acknowledgment
The authors gratefully acknowledge Dr. Haddad Alkaff and Dr. Sayed Raza from King Abdullah Medical City, Makkah, Saudi Arabia for their help in patient care.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received March 21, 2016.
- Accepted May 8, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}