


Abstract
Human chorionic gonadotropin has been used for decades, in addition to specific investigations, to detect pregnancy, trophoblastic tumors, as well as congenital defects. Rarely, it can be elevated in non-trophoblastic tumors such as squamous cell cancers and germ cell tumors. A 33-year-old Asian Syrian female had irregular menses accompanied with feelings of heaviness in the vagina. In addition to routine investigations, we measured the serum beta human chorionic gonadotropin (ß-HCG) level (based on the patient’s complaint of amenorrhea), which was 50.05 ml UI/ml. Cervical biopsy revealed a non-keratinized large cell squamous carcinoma. After excluding other causes, ß-hCG elevation was explained by the ectopic secretion of cancer cells line. Cervical biopsy was suggestive of large cell non-keratinizing squamous cell carcinoma and positive for human chorionic gonadotropin on immunohistochemistry. As a result, we manage the possibility of ectopic secretion of ß-HCG from non- trophoblastic disease.
Human chorionic gonadotropin has been used to detect pregnancy, which elevates in case of normal pregnancies as well as ectopic pregnancies. In addition, it can be utilized in diagnosing and following up trophoblastic tumors. Furthermore, it is a component of double and triple tests used in prenatal medicine to screen for fetal congenital abnormalities.1 In this case, the patient was diagnosed with cervical large squamous cell carcinoma (SCC), and the peculiar finding was abnormal elevation of serum beta human chorionic gonadotropin (ß-hCG). Moreover, this elevation was not high enough to be explained either by pregnancy, nor by trophoblastic tumors. We describe a case with uterine cervical large SCC accompanied with unexplained elevated serum ß-hCG. After ruling out pregnancy by repeating ß-hCG every 48 hours for one week, which had no doubling, and trophoblastic disease, depending on low levels of ß-hCG that did not exceed 60 mlU/ml, we suggest that this elevation can be explained by ectopic secretion of ß-hCG from the cancer cell line.
Case Report
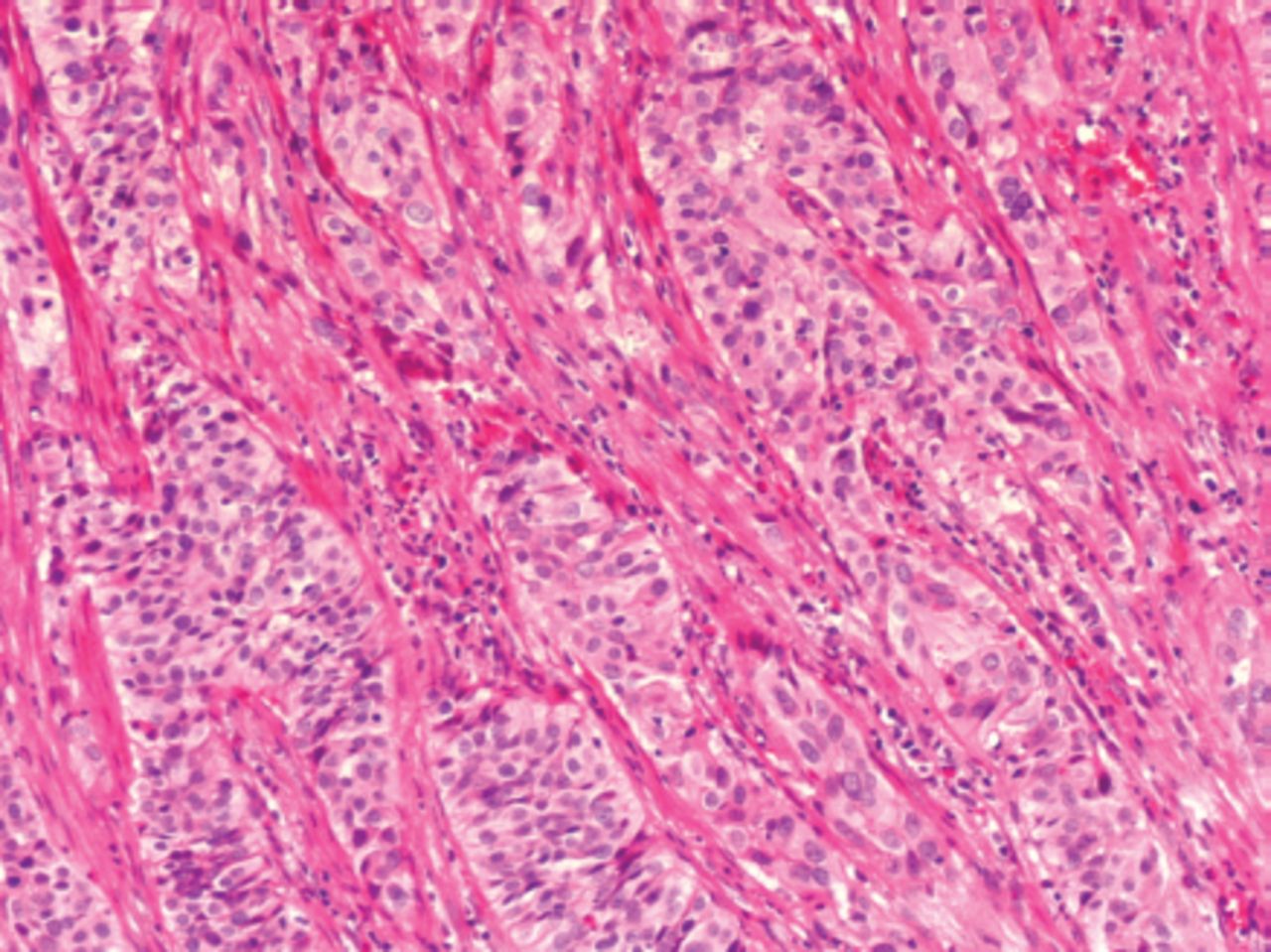
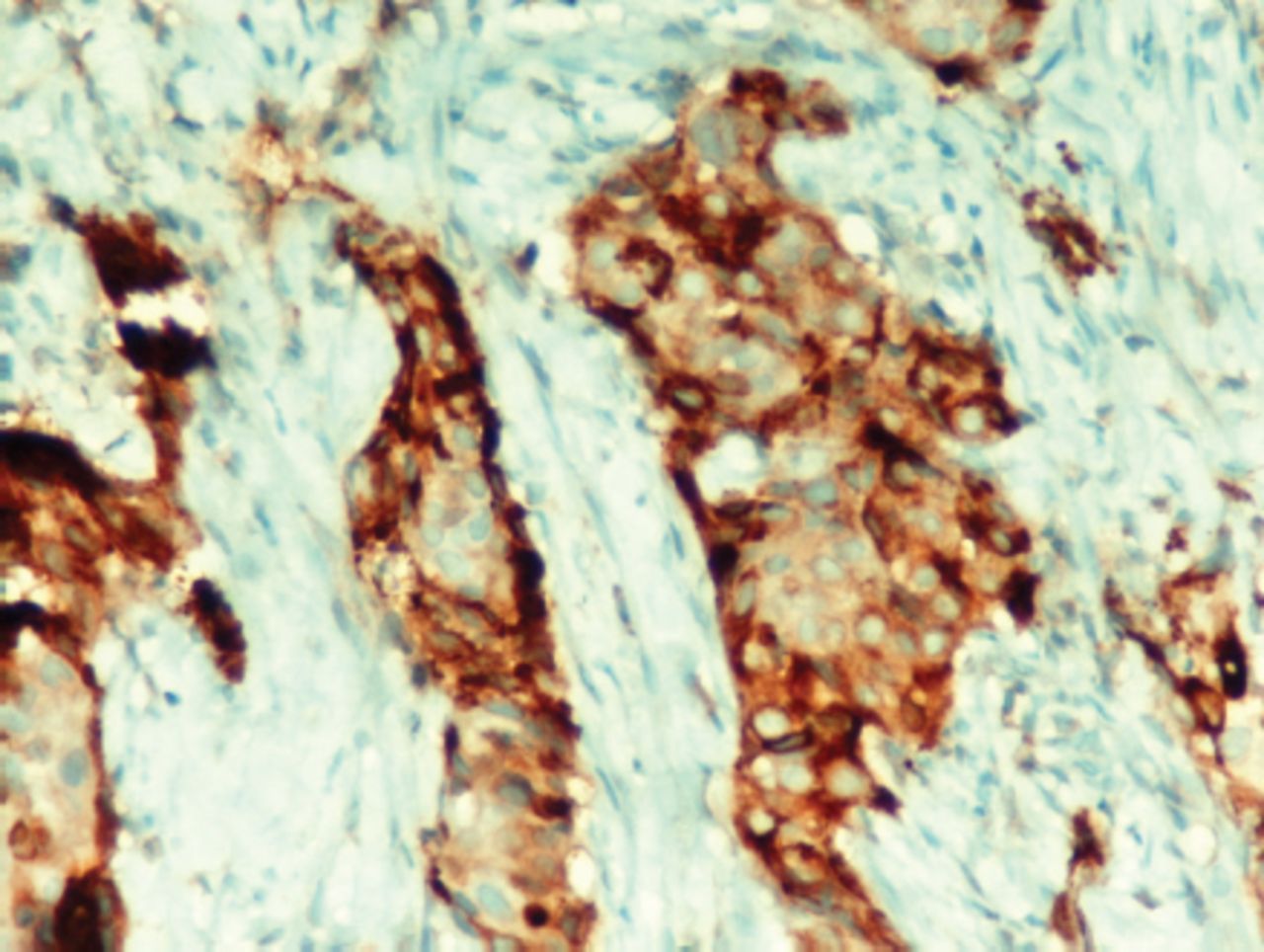
A 33-year-old Asian woman, gravida 6, parity 5 (last birth 4 years ago), abortion one, (6 years ago) presented with feeling of heaviness and pressure in the pelvis that was progressing for the last 2 weeks accompanied with amenorrhea as well as progressing dysuria. Bimanual examination revealed a fixed cervix. Palpation of the rectovaginal septum revealed a thick, hard, and irregular septum. During digital rectal examination, parametrial, uterosacral, and pelvic sidewall involvement was palpated. Ultrasonography demonstrated a 57mm x 40mm cervical mass. Cervical biopsy consisted of multiple fragments of white yellow, soft and firm tissue, measuring 1.1x1x0.4 cm for the largest fragment, and 0.4x0.3x0.2 cm for the smallest one. On routine pathologic examination, hematoxylin and eosin (H&E) showed infiltrative nests of neoplastic squamous cells with eosinophilic cytoplasm and prominent nucleolus, and lacked keratin pearls. Histopathologic findings were consistent with non-keratinizing SCC (Figure 1). Immunohistochemical stain showed cytoplasmic positivity with ß-hCG. For the immunohistochemistry, we used Ventana hCG (polyclonal) antibody (catalog number, 760-2650, Cell Marque, Roche Matrial USA). We used placental tissue as an external control, and showed positive staining that confirms true staining in our case (Figure 2).

Atypical infiltrative squamous islands in the fibrohyalinized cervical stroma, Hematoxylin and eosin x200.

Cytoplasmic positivity with beta human chorionic gonadotropin in squamous cell carcinoma, X400
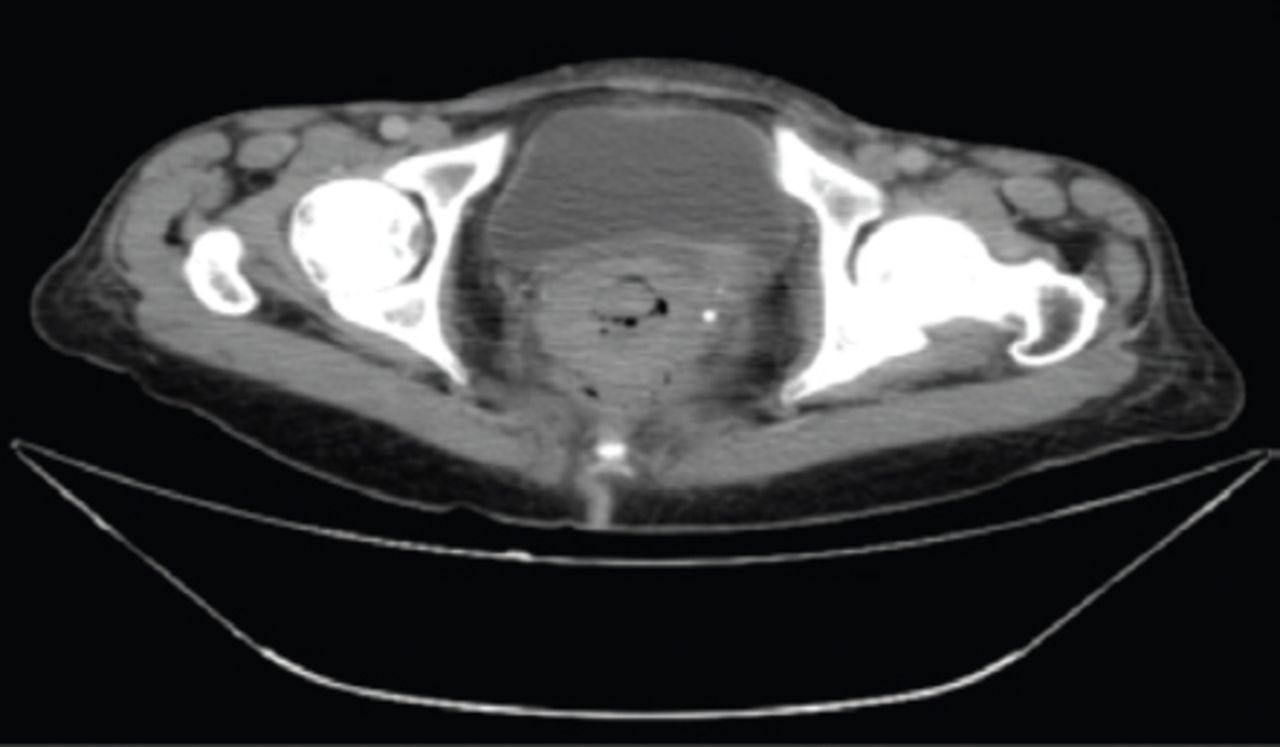
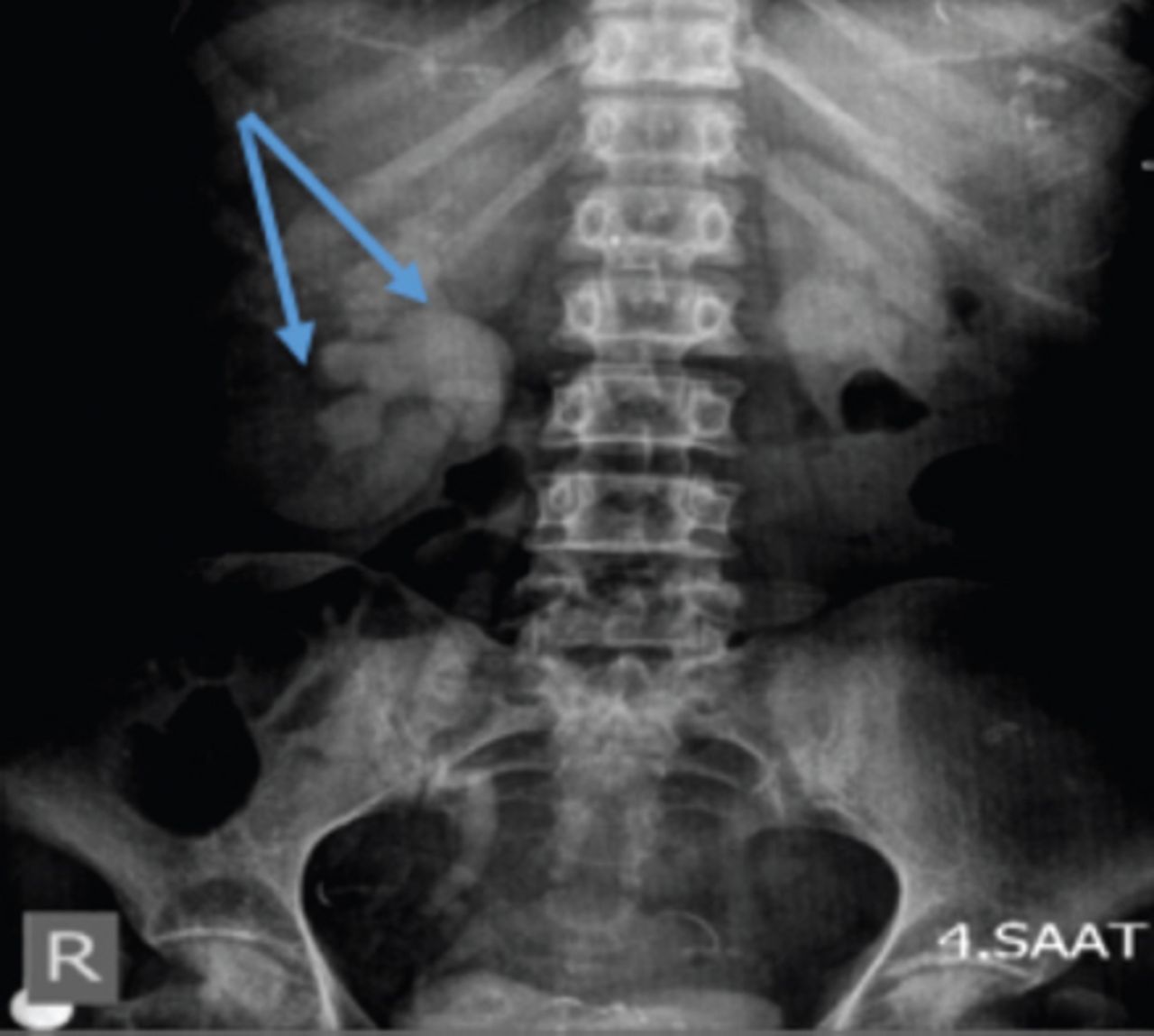
Computed tomography with contrast scans of the abdomen and pelvis showed a heterogeneous mass in the cervix that measures 5 cm (Figure 3), in addition, (3.5 x 2) cm liver metastasis were detected. There was no any mass in the ovaries, which excluded the possibility of germ cell tumor. Intravenous pyelogram (IVP) imagining illustrated a bilateral dilated pelvicalyceal system of the kidney with dilated tortuous right ureter (Figure 4).

A heterogeneous mass in the cervix that measures 5 cm, in addition, (3.5 x 2) cm liver metastasis has been detected.

Bilateral dilated pelvicalyceal system of kidneys with dilated tortuous right ureter.
She was classified as end stage disease. We referred the patient to the radiochemotherapy unit. Her b-hCG level was found to be slightly elevated (50.05 mlU/ml). As far as we know, this value is inexplicable either by pregnancy, nor by trophoblastic tumors, so it can be attributed to the ectopic expressions of ß-hCG from the squamous cancer cell line.
Discussion
Uterine cervical cancer is considered the third most common cancer diagnosed in women worldwide. Also, it is the fourth leading cause of death from malignancy among women.1 Human papilloma virus infection has been postulated to be the primary cause of cervical cancer. Thus, screening tests and early diagnosis have significantly reduced the incidence of cervical carcinoma. Human chorionic gonadotropin hormone consists of a 92 amino acid alpha subunit, and a 145 amino acid beta subunit, which share mutual evolutionary sequences with transforming growth factor (TFG) which can stimulate advanced cancer to invade and metastasize by inhibiting apoptosis process in cancer cells and producing collagenases and metalloproteinases, invasion proteases from cancer cells leading to metastases. It is postulated that advanced tumors differentiate tissues that can produce ectopic ß-hCG.3 Several researches postulate the possibility of utilizing ß-hCG as a tumor marker in diagnoses and follow up SCC, not only in uterine cervix cancers,4 but also in SCC of lung cancer.5 Furthermore, leiomyosarcoma of uterus can secret ß-hCG from the tumor cell line.6 We described a patient diagnosed with cervical large SCC accompanied with elevated serum ß-hCG and positive tissue expression of ß-hCG. We excluded other causes of ß-hCG elevation such as choricarcinoma, which has a biphasic pattern on microscopic examination. The tumor was composed of cytotrophoblasts (small, round mononuclear cells with pale cytoplasm) and syncytiotrophoblasts (multinucleated cells) with variable atypia, nuclear pleomorphism, hyperchromasia, and prominent nucleoli. It has a high mitotic activity and may have extensive necrosis with minimal trophoblastic tissue. As no cytotrophoblasts and syncytiotrophoblasts were seen, we excluded choriocarcinoma.
On CT scan, both ovaries were normal, excluding germ cell tumor as a source of elevated ß-hCG. According to Li et al,7 ß-hCG expression is probably associated with tumor aggressive behavior in diminishing tumor cell apoptosis and increasing vascularization. Furthermore, Hameed et al8 suggested that poorly differentiated squamous cell carcinoma of the uterine cervix showing immunoreactivity for ß-hCG should be distinguished from choriocarcinoma and other trophoblastic tumors. Elevated serum ß-hCG levels suggest the correlation between its levels of fluctuations with aggressive behavior of cancer cell line. Moreover, ß-hCG is considered a tumor growth factor (TFG) that can increase the aggressive behavior of these cells which can be the target in managing end stage cancers. Recently, studies3 have been conducted to utilize hCG vaccines for patients with advanced cancers. Initial clinical trials have encouraging results that doubled cancer survival rate. These vaccine studies suggest that hCG has a profound effect in managing advanced cancer.3
In conclusion, when we encounter a patient with slightly elevated serum ß-hCG, we have to keep in mind the possibility of large SCC as a resource of ectopic secretion. More advanced research is warranted to evaluate the treatment choices of invasive cancers that are directed to ß-hCG molcules
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received January 26, 2016.
- Accepted March 23, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}
{kind=link}
{kind=link}