


Abstract
Objectives: To study the effect of local wound infiltration with and without adrenaline on pain perception after thyroidectomy using the visual analog score (VAS).
Methods: A prospective randomized controlled double-blinded study was conducted between May 2015 and June 2016 at The University of Jordan Hospital, Amman, Jordan. Eighty-nine patients undergoing planned thyroidectomy were included in the study. Patients were divided randomly into 3 groups: Group A, local wound infiltration with bupivacaine 0.5% was administered; Group B, bupivacaine 0.5% with adrenaline was administered; Group C (control), no infiltration was performed. Standardized thyroidectomies were performed in the 3 groups. Pain perception was measured using VAS at 2, 4, 6, 12, and 24 hours after surgery. A comparison between the 3 groups was carried out.
Results: No significant differences among the 3 groups were observed at all time points (p=0.246). Visual analog scores were significantly lower at 12 and 24 hours after operations.
Conclusion: Local wound infiltration with bupivacaine 0.5% does not decrease pain perception after thyroidectomy performed under general anesthesia, and adding adrenaline does not enhance its effect.
Postoperative pain is one of the most important concerns for surgical patients. Although neck surgery is not considered a very painful procedure, adequate analgesia is essential. Surgeons and anesthesiologists have used various methods to prevent or treat postoperative pain, such as opioids and nonsteroidal anti-inflammatory drugs (NSAIDs), or with additional loco-regional anesthesia techniques. These techniques include local anesthetic wound infiltration, bilateral superficial cervical plexus block, and bilateral combined superficial and deep cervical plexus block.1,2 Bupivacaine and ropivacaine are the classical drugs used in loco-regional block. Combining bupivacaine with different adjuvants, such as adrenaline, dexmedetomidine, and clonidine, was reported to enhance the effect of block onset and duration of anesthesia.3-5 A limited number of studies in the literature have shown a significant effect of loco-regional anesthesia in reducing postoperative pain and opioid requirements.6,7 However, other studies could not demonstrate that effect.8 Out of this controversy, we set out to evaluate the effect of local wound infiltration on pain perception after thyroidectomy in a prospective controlled randomized manner comparing 2 types of local analgesics: bupivacaine alone and bupivacaine with adrenaline.
Methods
This was a monocentric prospective randomized controlled double-blinded study conducted at The University of Jordan Hospital, between May 2015 and June 2016. It was carried out according to the Declaration of Helsinki with the approval of the Hospital Ethics Committee (IRB: 11 May 2015- 10/2015/ 3711). All patients diagnosed with a thyroid disease who were scheduled for an elective thyroidectomy and met the inclusion criteria were included in the study. A full explanation of the procedure was provided, and written informed consent was obtained prior to randomization. These patients were randomized into 3 groups: Group A - represents local infiltration with bupivacaine 0.5%, Group B - represents local infiltration in which bupivacaine 0.5% was mixed with adrenaline, and Group C represents a control group in which no infiltration was performed. Randomization was carried out using a closed box with 90 sealed envelopes (30 for each group). One envelope was withdrawn at the time of surgery and then discarded.
Standardization of procedure
The surgical procedure was standardized for all patients. The operations were performed by 3 senior surgeons, all following the same surgical technique of neck extension, neck collar incision, upper and lower sub-platysma flaps, no transection of strap muscles, double ligation of superior thyroid vessels, ligation of inferior thyroid vessel branches close to the gland, and leaving a Readivac drain before closure in layers. Skin was closed subcuticularly with 3/0 absorbable monofilament thread. Ultracision and Ligasure were used as needed. A simple dressing was applied to all patients.
Inclusion criteria included: age 20-65 years, first time operation, no retrosternal extension, no cervical lymphadenopathy, and no diabetes or neurological disease. Exclusion criteria included: a complication within 24 hours (hemorrhage, hoarseness, or hypocalcemia), duration more than 120 minutes, and neck dissection decided intraoperatively.
Infiltration technique
Local infiltration was administered immediately before incision by a senior surgeon subcutaneously at the incision line. In Group A, infiltration was performed using 15 ml of bupivacaine 0.5%, while in Group B, it was performed using 15 ml of bupivacaine 0.5% mixed with adrenaline in a ratio of 1:200000. In Group C, no infiltration was performed.
Morphine was administered according to the weight immediately after extubation. Then, tramadol 50 mg was administered orally every 12 hours and paracetamol 1 g was administered orally every 8 hours for all patients. Pethidine was given only upon patient request.
Collected data included age, gender, educational status, preoperative diagnosis, and magnitude of procedure. Pain visual analogue score (VAS) at 2, 6, 12, 18, and 24 hours after surgery. All patients were blinded to grouping, and the VAS score was recorded by a researcher who was blinded to grouping. Twenty-four hours after surgery or a complication that met exclusion criteria.
Statistical analysis
Study data were summarized using descriptive statistics (namely, mean, median, standard deviation, range, frequency, percentage). The Shapiro-Wilk test was used to test whether continuous variables were distributed normally. Data of the 3 study groups were compared by an analysis of variance (ANOVA) test, and secondary comparisons between groups were performed with post-hoc Bonferroni and Tukey procedures. For the comparison of data at different time points, a multivariate analysis for repeated measures ANOVA test was performed (Wilk’s Lambda). For comparison of categorical variables, Chi-squared and Fisher’s exact tests were used. Statistical analysis was performed using the Statistical Package for the Social Sciences version 16.0 (SPSS Inc., Chicago, IL, USA). Statistical significance was set to p<0.05 except for Box’s M test, for which the significance was set at 0.001.
Results
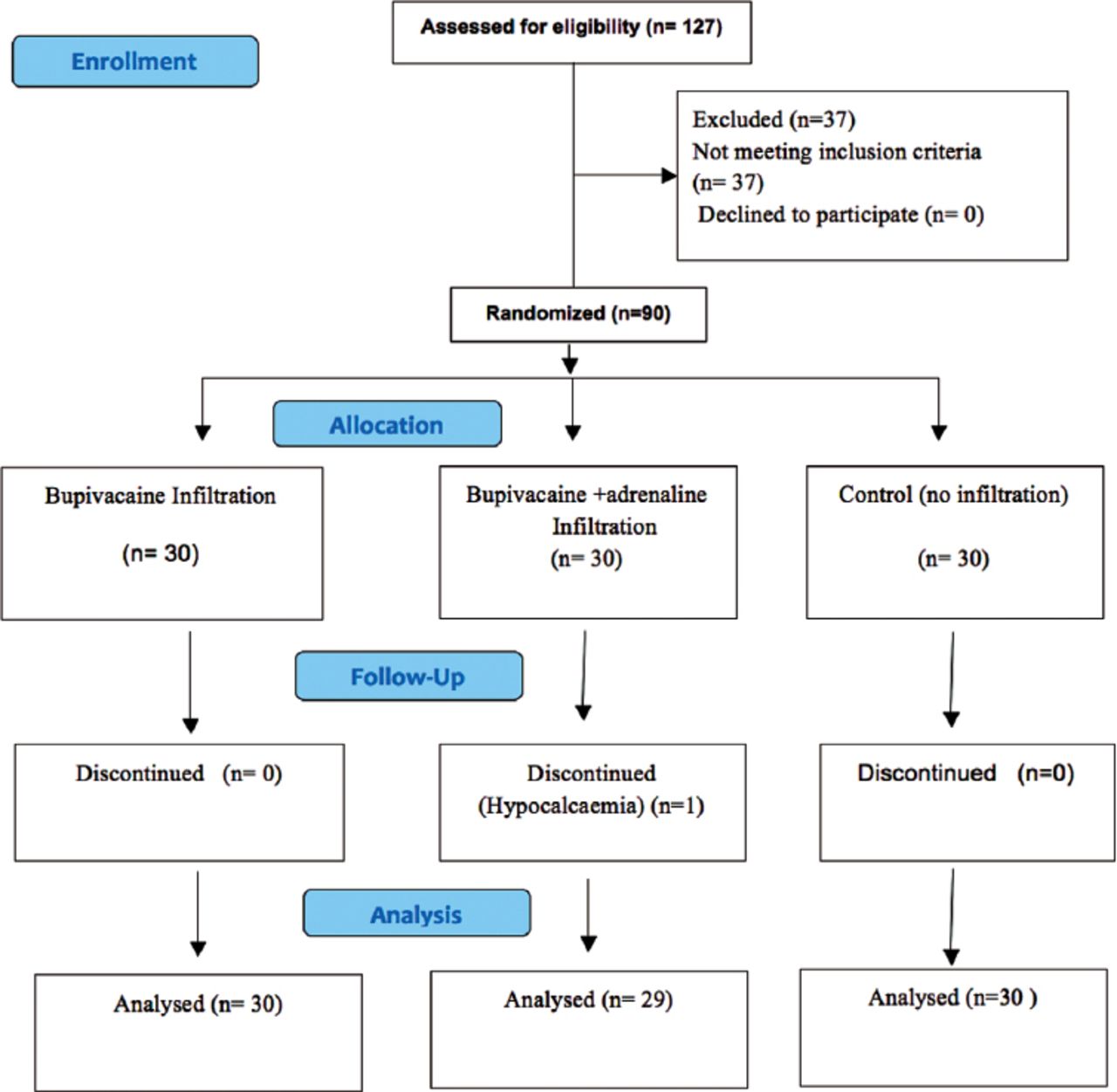
One hundred twenty-seven patients undergoing planned thyroid surgery at the Jordan University Hospital during the study period were assessed for eligibility. Thirty-seven were excluded as they did not match the inclusion criteria of the study. Ninety patients met the inclusion criteria; none of them refused to consent to the study. Thus, 90 patients were enrolled in the study. These were randomized to a control group and 2 study groups during the study period. One patient was excluded from the bupivacaine with adrenaline group because of symptomatic hypocalcemia. Data for 89 patients were analyzed as shown in Figure 1.
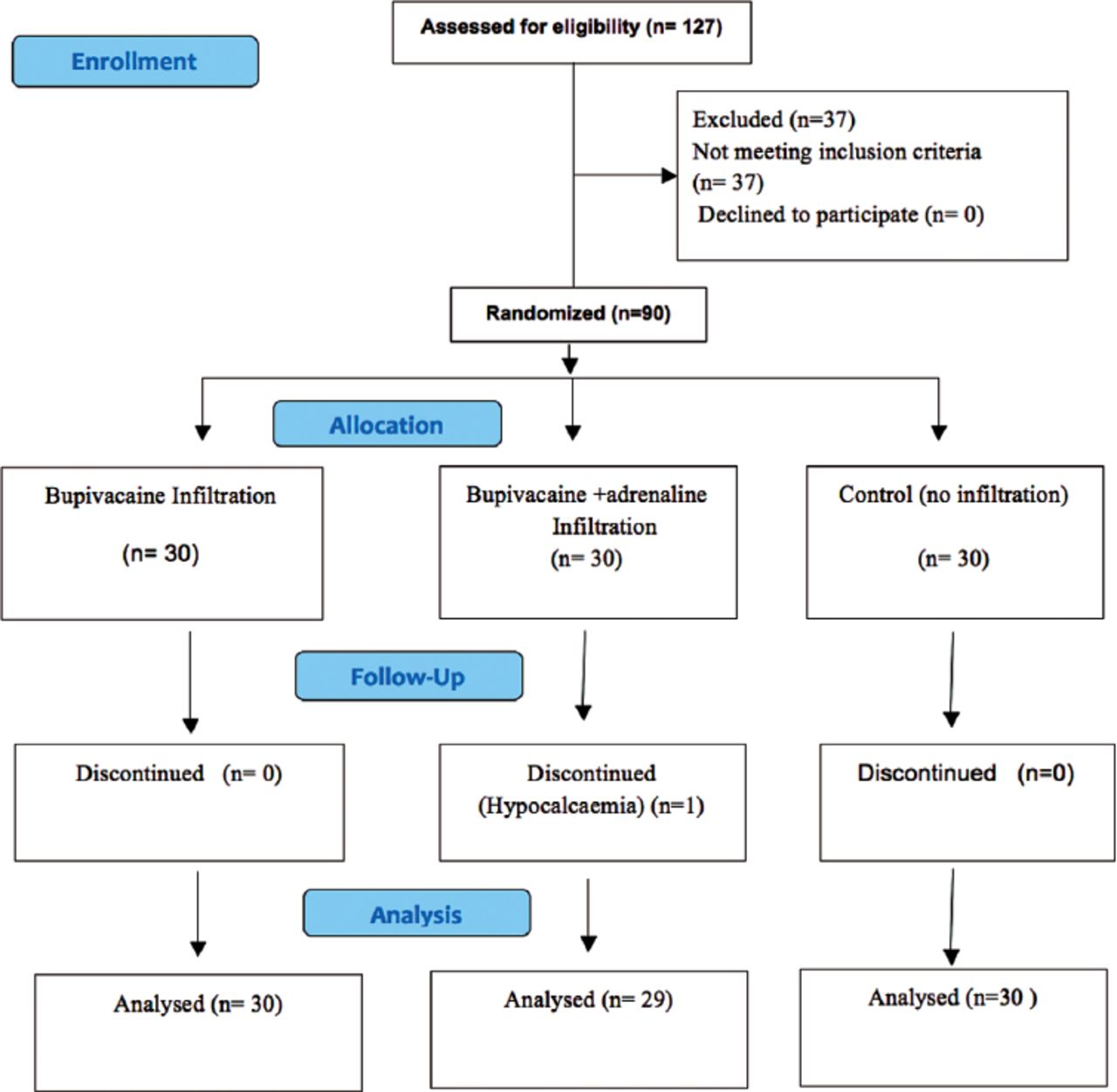
Flowchart of the 89 patients undergoing planned thyroid surgery at the Jordan University Hospital during the study period.
The 3 groups were comparable in terms of age, gender, and educational status. The benign/malignant ratio was lower in the control group, which is attributed to the random allocation. The demographics are illustrated in Table 1.
Demographic variables of 89 patients undergoing planned thyroid surgery at the Jordan University Hospital during the study period.
No significant differences were observed at any time point (p=0.246). Pain VAS were significantly lower at 12 and 24 hours after operations (24 hours was different from all other treatments, while 12 hours was different from 2, 4, and 6). No significant differences were observed between 2, 4, and 6-hour pain scores. The results are shown in Table 2.
Pain visual analogue score (VAS) for bupivacaine, bupivacaine with adrenaline and control group at different time points.
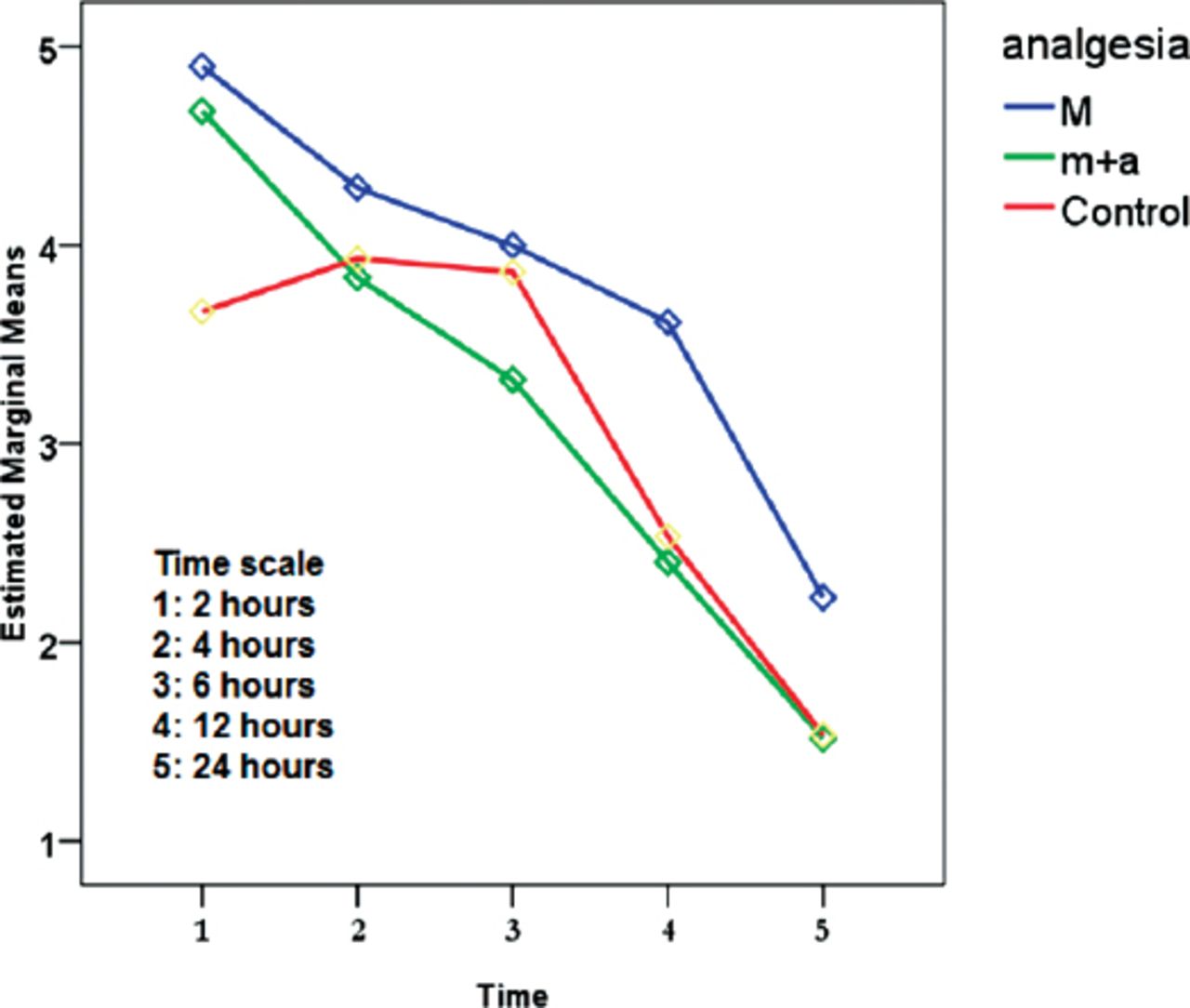
The trend of VAS score in relation to time for the 3 groups during the first 24 hours after surgery is demonstrated in Figure 2.

Trend of visual analogue score for bupivacaine (m), bupivacaine with adrenaline (m+a) and control groups during the first 24 hours after surgery.
Postoperative analgesia for the 3 groups was assessed; the control group received less amount of pethidine in comparison to the 2 study groups. Overall 24 patients received a single injection, 7 patients received 2 injections while 2 patients received 3 injections. The other 56 patients did not require parenteral analgesia as demonstrated in Table 3.
Postoperative analgesia required by bupivacaine, bupivacaine with adrenaline and control groups.
Discussion
Local tissue infiltration is a well-studied method of pain management. Its efficacy in decreasing postoperative pain was demonstrated in many procedures like cholecystectomy, hysterectomy, and hernia repair.9,10 The main advantages of this technique are its simplicity, safety, and low cost. In thyroid surgery, there are many procedures for loco-regional infiltration that include local wound infiltration (LWI), bilateral superficial cervical plexus block (BSCPB), and bilateral deep cervical plexus block (BDCPB). All share the same principle of cervical plexus sensory blockage, but at different levels. The BDCPB is performed by a single injection at the mid lateral border of the sternocleidomastoid muscle. The BSCPB is performed by infiltration at the midpoint of the lateral border of the sternocleidomastoid muscle in 4 directions to block the main branches of the cervical plexus. Local wound infiltration can be performed either preoperatively by marking the proposed incision and infiltrating it or postoperatively by infiltrating the edges of the incision. Although all 3 methods were described in thyroid surgery, LWI has the advantage of being practically easier and does not require special measurements and a trained person to perform.
Bupivacaine is considered the classic long-acting analgesic drug used for wound infiltration. Different additives have been used to prolong regional blockades and shorten the onset times of blocks. Vasoconstrictors have been used to constrict vessels, thereby reducing vascular absorption of the local anesthetic. Other drugs as opioids, clonidine and verapamil have been added to local anesthetics to enhance its effect, the results were variable.
In the literature, there are contradictory reports regarding the efficacy of loco-regional infiltration methods in controlling pain after thyroidectomy performed under general anesthesia. Shih et al11 reported that BSCB significantly lower the severity of postoperative pain during the first 24 hours and shortens the hospital stay. Kale et al12 concluded that, whether given pre-surgically or post-surgically, BSCB significantly reduced pain intensity and opioid requirement. Gozal et al6 reported that bupivacaine wound infiltration in thyroid surgery reduces postoperative pain and opioid demand. On the other hand, Eti et al13 prospectively concluded that bilateral superficial cervical plexus block or local anesthetic wound infiltration with 0.25% bupivacaine did not decrease the analgesic requirement after thyroid surgery. Herbland et al14 concluded that bilateral superficial cervical plexus block with 0.75% ropivacaine administered before or after surgery does not affect postoperative pain after total thyroidectomy.14 Miccoli et al15 reported that the benefit of local wound infiltration with local analgesia in decreasing postoperative pain is limited to a short period after surgery.15 This controversy encouraged us to examine the effect of bupivacaine wound infiltration on pain perception after thyroidectomy and to compare it to an enhanced form mixed with epinephrine, in which we anticipated a longer duration and better patient satisfaction.
In the current study, we noticed that post-thyroidectomy pain was not as severe as expected. The mean VAS score was less than 5 for the 3 groups throughout the period of study. The VAS score for the control group was less than both the bupivacaine and the bupivacaine with adrenaline groups most of the time. The mean VAS scores for the 2 study groups were comparable, and the difference was statistically insignificant. The pain perception reached its maximum in the first 6 hours for the 3 groups and remained steady throughout that period. Then, it decreased at 12 hours, with a further decrease at 24 hours post-surgery to be minimal in most of the patients. The 3 groups shared the same pattern. None of the patients required opioids after 6 hours of surgery, and no one reported bruises or disfiguring changes. One of the surgeons noticed that the surgical field, especially the sub-platysmal dissection, was easier and almost bloodless in the marcaine with adrenaline group, but we could not validate this comment objectively.
Bupivacaine and adrenaline infiltration is not without risk. In fact, there are many reported cases in the literature describing complications related to local infiltration, ranging from a mild hematoma to a very serious cardiac and central nervous system toxicity and even death. Neither bupivacaine infiltration nor the enhanced form mixed with adrenaline has an impact on pain perception after thyroidectomy. We think this procedure has no measureable benefit and carries possible hazards; thus, it should be abandoned.16-19
This study has the advantages of being prospective, randomized, controlled and double-blinded. The strict inclusion and exclusion criteria assured comparable samples in terms of magnitude of operation, degree of dissection, and tissue injury. We studied the pain course during the first 24 hours rather than the maximum pain perceived.
Study limitations
There are few limitations that might have interfered with the results; the benign/malignant ratios were not comparable in the 3 groups, the subjects in the study belong to one ethnic group and there were some variables that were not studied, such as body mass index, thyroid size, and length of incision.
In conclusion, adding adrenaline does not improve the analgesic effect of wound infiltration with bupivacaine after total thyroidectomy performed under general anesthesia.
Ethical Consent
All manuscripts reporting the results of experimental investigations involving human subjects should include a statement confirming that informed consent was obtained from each subject or subject’s guardian, after receiving approval of the experimental protocol by a local human ethics committee, or institutional review board. When reporting experiments on animals, authors should indicate whether the institutional and national guide for the care and use of laboratory animals was followed.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 2, 2017.
- Accepted July 25, 2017.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}