


Abstract
Conjoined twins are derived from division of a single fertilized ovum after the twelfth day of fertilization. Triplet conjoined twin is considered as a unique phenomenon that is accompanied with a wide variety of congenital abnormalities and also hazardous consequences for both fetuses and parents. We present an extremely rare case of conjoined twins in a triplet pregnancy with symmetric thoracoomphalopagus that was diagnosed in prenatal period by using ultrasound scanning and MRI. In triplet pregnancies, we should be aware about the possibility of conjoined twins. If there are severe congenital malformations, termination of pregnancy should be recommended immediately after the diagnosis regardless of gestational age, particularly in early gestational age.
Conjoined twins are derived from division of a single fertilized ovum after the twelfth day of fertilization. The incidence is approximately 1 per 80,000 deliveries.1 Triplet conjoined twin is a unique phenomenon and the incidence is less than one in a million deliveries. Conjoined twins are considered as a hazardous condition due to challenges in management strategy despite of their rare incidence.2 Most parents decides to terminate pregnancy as the diagnosis is established. The recurrence rate of conjoined twins has no difference from normal twins.3 We present an extremely rare case of conjoined twins in a triplet pregnancy with symmetric thoracoomphalopagus that was diagnosed in prenatal period by using ultrasound scanning and magnetic resonance imaging.
Case Report
A 28-year-old Caucasian woman (gestation 3, parity 2, abortion 0, living children 2), who spontaneously conceived, was referred to our clinic at 17 weeks of gestation with a suspicion of conjoined twins in a triplet pregnancy. Her past medical, obstetric and surgical history did not reveal any problem. Antenatal diagnosis of the conjoined triplet twin pregnancy was made by using 2-dimensional ultrasonography with a 3.5 MHz convex probe (Voluson e6 compact-GE Healthcare, GE Medical Systems Ltd, Hertfordshire) and MRI. Transabdominal and transvaginal ultrasound scans revealed a dichorionic-diamniotic triplet pregnancy. One of the amniotic sacs contained an apparently healthy male fetus with measurements consistent with 17 weeks of gestation. In the other amniotic sac, a set of male conjoined twins fused from the top of the upper thorax down to the umbilicus with 2 separate hearts, one common liver, 4 arms, 4 legs and a single umbilical cord were identified (Figure 1). Moreover, detailed transabdominal ultrasound scan of conjoined twins showed massive ascites, hydrocephalus and pleural effusion with expanded thorax and abdomen. The diagnosis of conjoined twins with thoracoomphalopagus was confirmed by using MRI (Figure 2). Detailed information about the available management options was given to the parents including selective feticide of the conjoined twins at 17 weeks of gestation and they decided to continue the pregnancy. Following a deliberation for one month, they came back with a decision in favor of selective intracardiac potassium chloride injection to one of the conjoined twins at the 21st week of pregnancy. Cardiac arrest of conjoined twins was recognized approximately 3 minutes following this process. However, healthy fetus was alive in the next 10 minutes. One day later, a repeated scan revealed intrauterine death of healthy fetus with demise of conjoined twins. Pregnancy was terminated by hysterotomy with T-shaped incision. The mother made an uneventful recovery and was discharged 2 days later. Autopsy report of the single fetus: lungs, heart, umbilical cord were normal. The conjoined twins: the lungs was normal, the heart and thymus undergo autolysis, spleen was normal, liver undergo partial autolysis, the stomach undergo autolysis, the intestine and kidneys undergo partial autolysis, the brain undergo autolysis, umbilical cord has 2 arteries and one vein. One of the conjoined has acrania.

Ultrasonographic image of conjoined twins (thoracoomphalopagus) with 2 separate hearts (also shown with arrows) and pleural effusion (asterixes).

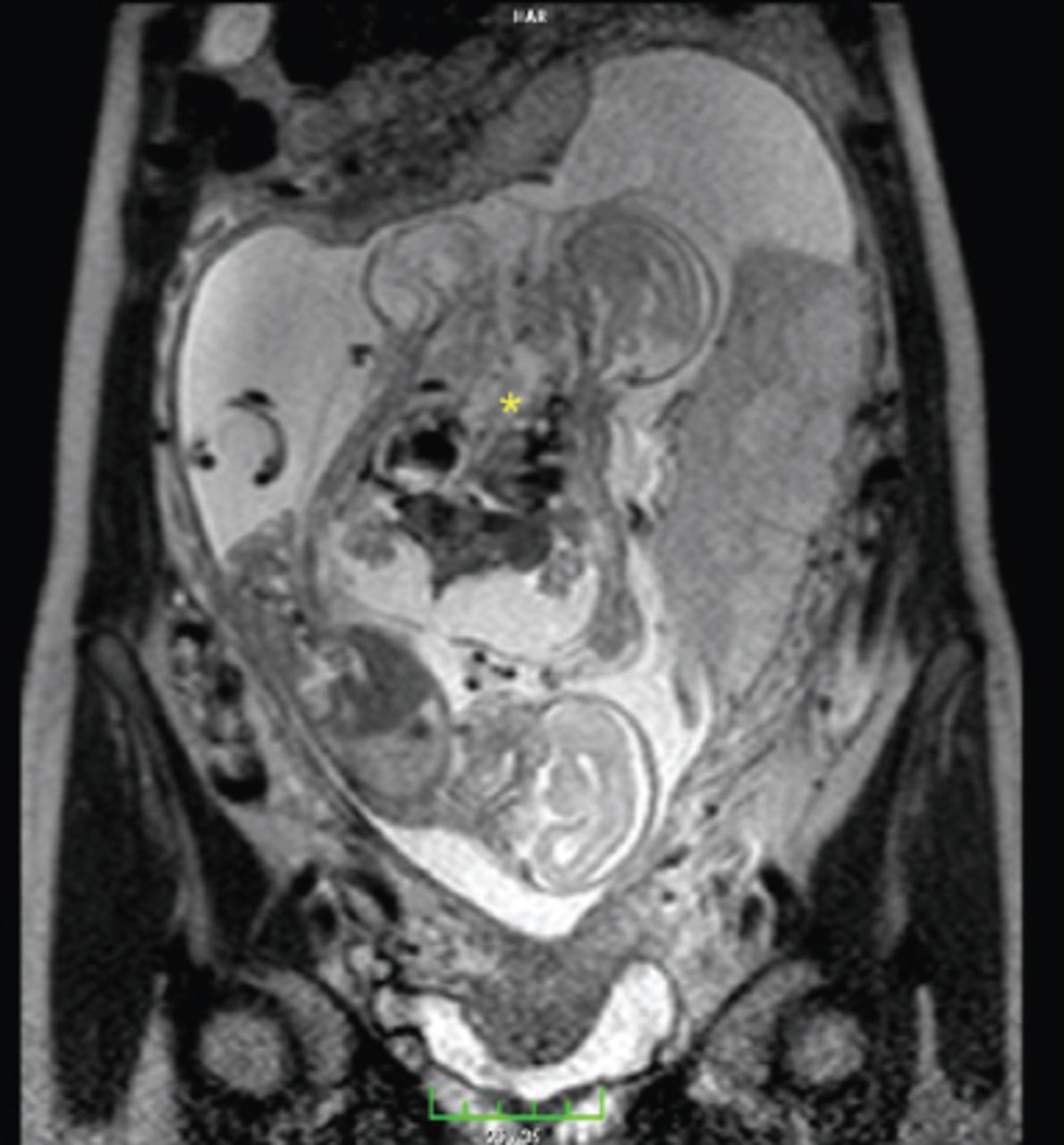
Magnetic resonance image of conjoined triplet twins with symmetric thoracoomphalopagus (asterisks) showing massive ascites, hydrocephalus and pleural effusion with expanded thorax and abdomen.
Discussion
Triplet conjoined twin is considered as a unique phenomenon that is accompanied with a wide variety of congenital abnormalities and also hazardous consequences for both fetuses and parents. Two theories have been postulated to explain how conjoined twins are formed. The traditional theory is “fission theory” that suggests conjoined twins occurs when a fertilized ovum splits incompletely leading to separation of the embryonic mass after the twelves day of fertilization.4 The second theory is “fusion theory”, which can explain all conjoined twins. Fusion theory advocates that fertilized egg is completely separated, but in somehow the stem cells of one fetus fuse with the similar stem cells of the other fetus.5 There are many classifications of conjoined twins. One of them depends on the most prominent adhesion region that encompasses the following 5 types: thoracopagus (thorax), omphalopagus (abdomen), pygopagus (sacrum), ischiopagus (pelvis), craniopagus (cranium), cephalopagus (face), and rachipagus (dorsal). Thoracoomphalopagus is one of the most common types of conjoined twins with a rate of 75%.6
Today, most of the cases are diagnosed in prenatal period using ultrasonography. This scanning procedure allows counseling of the family about the management options, including termination of the whole pregnancy, selective feticide of the conjoined twins or continuing the pregnancy. Continuing the pregnancy without any further intervention is associated with high incidence of complications including prematurity and neonatal death for the non-conjoined triplet. Although termination of the entire pregnancy includes an ethical dilemma of termination of the healthy fetus. Selective fetal reduction decreases mortality and morbidity rates for the single fetus, but there is an abortion rate varies between 5% and 10% based on gestational age.2,7 In our case, cardiac arrest of normal fetus can be related to the high dose of 6 ml of potassium chloride (KCL) administered to the conjoined fetuses or can be resulted from an unpredictable passage of the KCL through possible placental vascular anastomosis. The flow from such anastomosis may increase as pregnancy progresses. Thus, performing selective feticide at 22 weeks rather than 17 weeks may result in demise of the healthy fetus.
The purpose of selective fetal reduction is to avoid possible large incisions of both abdomen (midline incision) and uterus (classical uterine incision) to deliver term conjoined fetuses, who are not compatible with life. We performed a small T shape uterine incision following phannenstiel incision. Therefore, accurate determination of chorionicity is crucial in planning the treatment strategy and in predicting the outcomes of these pregnancies.2 Although, this can be performed precisely in the first trimester, it can be predicted in the second and third trimester depending on ultrasound criteria, which includes basically the absence of a separating membrane between twins and the failure to discriminate similar parts of the fetal body.1 Recently, development in prenatal medicine facilitates termination of conjoined twins following early diagnosis. Thus, standard approach for managing conjoined twins until term and beyond is unacceptable.8 If there is a limitation in postpartum surgical separation of the twins, termination of pregnancy should be decided regardless of gestational age.4 In addition to severity of the case, parents’ social situation, religious and psychological beliefs should be considered in the management of conjoined twins.8 If selective feticide is decided, parents should be informed of complications such as neurological sequelae, subsequent fetal demise or increased miscarriage rate fluctuating from 5% to 10%, that survivor may encounter.2 In spite of the presence of some reported vaginal deliveries of conjoined twins in the literature, cesarean section is still the first choice of delivery when possible obstetrical injuries are considered, even in preterm pregnancies.6,9 If parents decided to continue pregnancy, there is no ideal period for delivery. The possible indications for surgery include the presence of active uterine contractions and maturity of multiple pregnancy after providing well intensive neonatal care unit. Longitudinal incision is the most preferred uterine incision.10
In our case, fetal reduction was performed at 22 weeks and the presence of placental anastomosis may have led to death of healthy fetus. We believe that fetal reduction should be performed immediately after diagnosis at 17 weeks to minimize the unintended passage of KCL to the healthy fetus through placental anastomosis.
In conclusion, triplet conjoined twins is a unique phenomenon. In each case of triplet pregnancies, the clinician should be aware about the possibility of conjoined twins. If there are severe congenital malformations, termination of pregnancy should be recommended immediately after the diagnosis regardless of gestational age, particularly in early gestational age. According to our experience we can suggest that: the sooner fetal reduction the better management of triplet conjoined twins.
Acknowledgment
We would like to thank Dr. Feyza Gelebek for revising our radiology images.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received August 11, 2016.
- Accepted November 9, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.